
Abstract
Summary: We present a case of delayed thromboembolic events that occurred 9 weeks after endovascular treatment of an anterior communicating artery aneurysm with GDC.
Acute thromboembolic events are a well-known complication of cerebral artery aneurysm treatment with GDC. Periprocedural complication rates have been reported to range between 2.5% and 28% (1–3). These events present as transient ischemic attacks or strokes and usually occur at the time of the procedure or within the first 48 hr (2). However, the occurrence of delayed thromboembolic events (weeks or months after the procedure) in a patient with stable coil packing of the aneurysm sac has not been previously described in the literature.
Case Report
A 54-year-old man presented to the emergency room of an outside hospital with a severe headache of sudden onset. An initial CT study revealed no acute hemorrhage. Because of the patient’s symptoms, MR angiography was performed and revealed an anterior communicating artery aneurysm. The patient was then referred to our medical center, where CT angiography was performed to further define the aneurysm anatomy. CT angiography showed an 11 × 7 mm lobulated anterior communicating artery aneurysm with a 4-mm neck (Fig 1). The geometry of the aneurysm was thought to be suitable for either surgical or endovascular therapy. Both options were offered to the patient who chose to undergo attempted endovascular treatment.

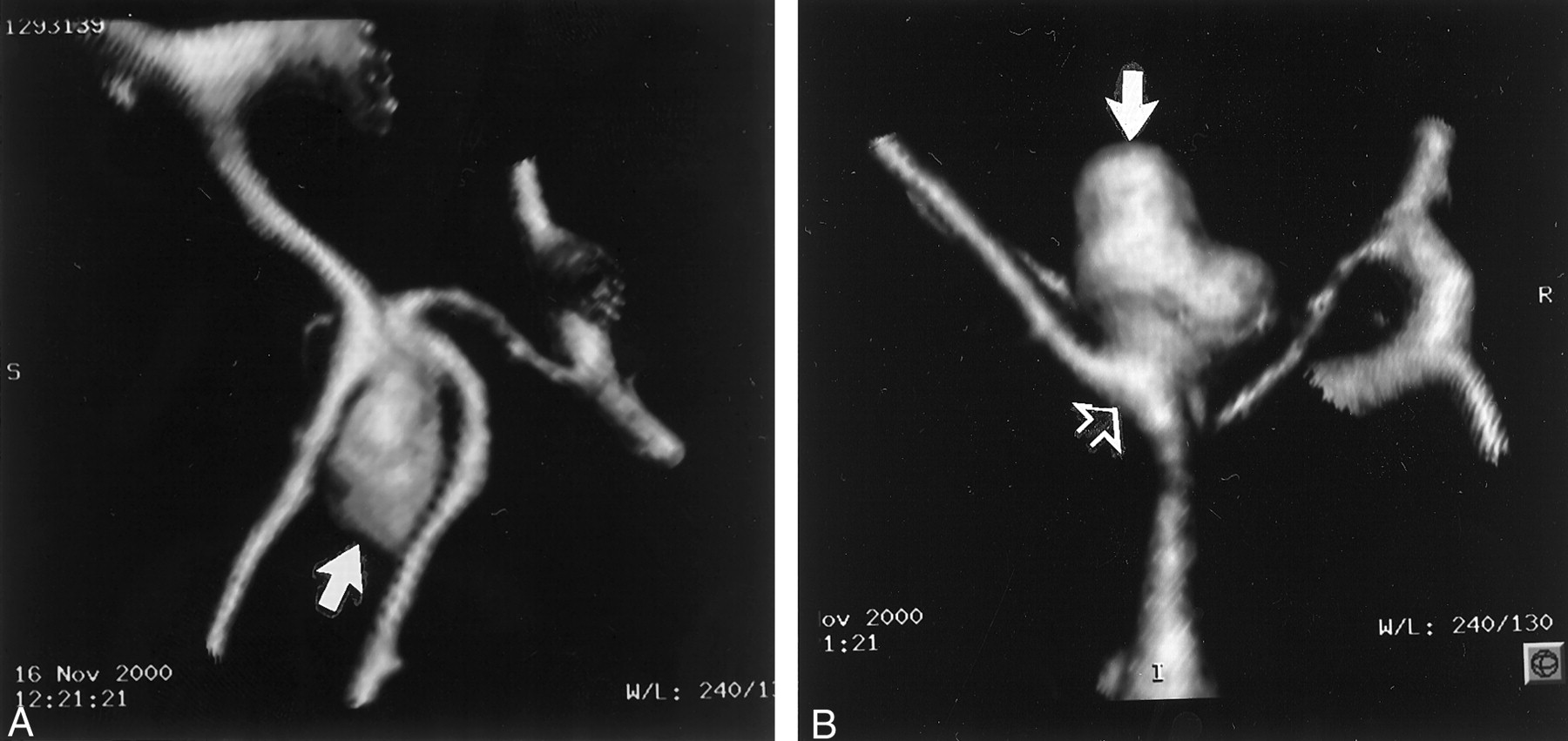
CT angiograms obtained to further define aneurysm anatomy in the case of a 54-year-old man.
A, Water’s projection with 3D reconstruction shows a 11 × 7 mm anterior communicating artery aneurysm (arrow).
B, Lateral view shows a lobulated anterior communicating artery aneurysm (solid arrow) with a 4-mm neck (open arrow).
The aneurysm was treated with 12 Guglielmi detachable coils (GDCs). The postoperative angiograms showed total occlusion of the aneurysm sac with no residual contrast material filling of the aneurysm sac or neck. No coil loops extended beyond the aneurysm sac into the anterior communicating artery, which remained patent (Figs 2 and 3). The patient tolerated the procedure well without any periprocedural complications. CT of the head performed immediately after coil placement showed no intracranial bleed or evidence of acute thromboembolic events. The patient experienced an unremarkable post-procedural course and was discharged several days later with entirely normal results of a neurologic examination. Neither aspirin nor other antiplatelets were administered because of clinical suspicion that this aneurysm may have been an occult rupture at the time of presentation, despite the negative CT findings.

Preoperative injection of the left internal carotid artery shows the anterior communicating artery aneurysm (straight arrow) with cross filling of the right anterior cerebral artery (curved arrow).

Postoperative angiograms showed total occlusion of the aneurysm sac, with no residual contrast material filling of the aneurysm sac or neck.
A, Magnified postoperative anteroposterior angiogram shows the densely packed aneurysm sac (straight arrow). No coils extend into the well-visualized aneurysm neck (curved arrow).
B, Subtracted postoperative anteroposterior angiogram shows no residual blood flow in the aneurysm sac (solid arrow). Cross filling of the anterior cerebral artery (curved arrow) can be seen.
The patient presented 9 weeks later complaining of right foot drop, which progressed to complete right lower extremity monoplegia over 36 hr. CT of the head performed 36 hr after initial onset of symptoms showed no acute bleed. MR imaging performed 9 hr later showed multiple bilateral diffusion-weighted abnormalities scattered in the distribution of the anterior cerebral arteries, consistent with acute embolic infarcts (Fig 4). No abnormalities were present in the middle or posterior cerebral artery territories, suggesting the anterior communicating artery as the embolic source. Cerebral angiography was performed the next day, and the findings were unchanged from those of the immediate postoperative study. There was no shift in the positioning of the coils or residual filling of the aneurysm sac.

Axial diffusion-weighted MR images obtained 9 weeks after endovascular treatment.
A and B, Multiple regions of high signal intensity are depicted bilaterally in the distribution of the anterior communicating arteries, consistent with acute embolic infarcts.
The patient was discharged 2 days later after being placed on antiplatelet therapy and showing mild improvement in the right lower extremity weakness. The only remaining neurologic deficit 6 weeks later was mild toe extensor weakness.
Discussion
Thromboembolic events are a well-known complication of endovascular treatment of cerebral aneurysms. They are the most important cause of permanent morbidity associated with the procedure (3). The vast majority of previously reported thromboembolic events associated with coil placement occurred within 48 hr of the procedure (1, 2). Lenthall et al (4) reported a single case of delayed occlusion of the superior cerebellar artery associated with reconfiguration of GDC at the neck of a treated aneurysm. Delayed thromboembolic events occurring de novo with stable coil packing have not previously been described in the literature. In this case, the progressive nature of the patient’s symptoms combined with multiple diffusion abnormalities in the distribution of the anterior cerebral arteries on MR images suggest multiple embolic events originating from the treated anterior communicating artery aneurysm.
Because of the known risk of periprocedural thromboembolic events, heparin is routinely used during GDC placement. However, heparin has limited effectiveness, possibly because of its lack of inhibition of platelet aggregation (3). Although no definitive evidence exists at this time to support the use of antiplatelet medications during or after endovascular aneurysm treatment, the theoretical benefits have led to their use at some institutions.
Postoperative anticoagulation was not used in this case because of a recent institutional experience with a patient who rebled while receiving antiplatelet medications after endovascular treatment of a ruptured intracranial aneurysm. However, no empirical evidence exists to suggest that anticoagulation increases the risk of rebleeding in an endovascularly treated aneurysm.
This case illustrates that thromboembolic events can occur many months after endovascular aneurysm coil placement. Aneurysms with relatively large necks, as in this case, theoretically may be at increased risk of thromboembolic events because of the increased surface area of exposed thrombogenic material. The occurrence of delayed thromboembolic events at 9 weeks suggests that there may be benefits to the use of antiplatelet medications after endovascular coiling extending well beyond the periprocedural time frame. However, the effectiveness of antiplatelet medication in preventing delayed thromboembolic events and the risks of rebleeding of endovascularly treated aneurysms need further investigation.
Conclusion
The occurrence of delayed thromboembolic events 9 weeks after endovascular coil placement suggests that there may be a role for prolonged antiplatelet therapy after GDC aneurysm treatment.
- Received November 19, 2001.
- Accepted after revision January 14, 2002.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.