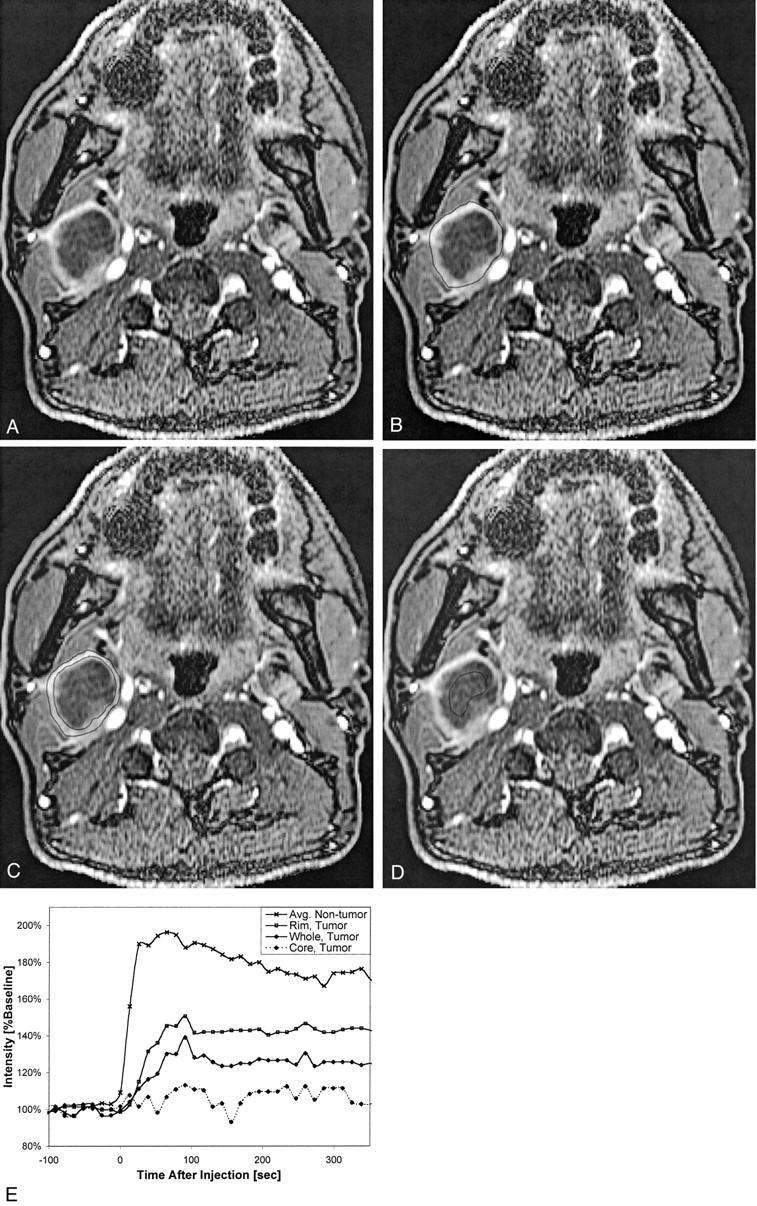
Fig 4.

Patient 7, a 52-year-old man who had previously undergone partial glossectomy for squamous cell carcinoma of the tongue, received no additional therapy, and then presented with a palpable right neck mass. Fine needle aspiration confirmed recurrent squamous cell carcinoma in the neck, and MR imaging revealed right cervical necrotic lymphadenopathy. The patient then underwent re-excision of the primary site and a right radical neck dissection.
A, Coil-corrected axial view enhanced dynamic image (10.4/2.3; flip angle, 30 degrees), acquired 195 s into the acquisition, shows a large, centrally necrotic, right level IIA lymph node.
B, Same image as that shown in A, with the region of interest encompassing the whole node shown.
C, Same image as that shown in A, with the region of interest encompassing only the rim shown.
D, Same image as that shown in A, with the region of interest encompassing only the necrotic core shown.
E, Plot of signal intensity versus time from this node, with curves generated from regions of interest placed on the whole node, the rim only, and the necrotic core only. Note that the “rim” curve is very similar to the “whole” curve but appears reduced in magnitude by a scaling factor related to the necrotic core. All these curves appear very different from the average non-tumor curve that is shown for comparison, but a statistically significant comparison was not possible because of the small number of grossly necrotic nodes.









{kind=link}
Related Articles
Cited By...
- Characterization of cervical lymph nodes using DCE-MRI: Differentiation between metastases from SCC of head and neck and benign lymph nodes
- Dynamic Contrast-Enhanced MR Imaging in Head and Neck Cancer: Techniques and Clinical Applications
- Optimization of Ultrasmall Superparamagnetic Iron Oxide (P904)-enhanced Magnetic Resonance Imaging of Lymph Nodes: Initial Experience in a Mouse Model
- Multiparametric MR Imaging of Sinonasal Diseases: Time-Signal Intensity Curve- and Apparent Diffusion Coefficient-Based Differentiation between Benign and Malignant Lesions
- Current Concepts in Lymph Node Imaging