
Abstract
BACKGROUND AND PURPOSE: Our goal was to determine whether preoperative MR imaging of facial muscles predicts facial function after facial nerve grafting.
METHODS: A retrospective review of all patients undergoing facial nerve grafting between 1997 and 2001 revealed 26 patients. Twelve of the patients had adequate preoperative MR images available for review and had undergone clinical follow-up for at least 12 months. Eight had malignant parotid tumors, and four had benign skull base or parotid tumors. Preoperative facial muscle MR imaging appearance was categorized as symmetrical or asymmetrical. The asymmetrical images were further classified into mild or pronounced asymmetry. Preoperative facial function was classified by using the House-Brackmann scale. Postoperative function was graded with the May scale.
RESULTS: Four patients had symmetrical facial muscles shown by preoperative MR imaging, three had mild asymmetry, and five had pronounced asymmetry. No or mild asymmetry had an 86% positive predictive value for good to excellent functional outcome. Eighty percent of patients with pronounced asymmetry experienced poor functional outcomes. Six of eight patients with malignant and perineural tumors at surgery had asymmetrical facial muscles revealed by preoperative MR imaging studies.
CONCLUSION: Symmetrical or mildly asymmetrical facial muscles are predictive of good facial function after nerve grafting. Pronounced asymmetry of facial muscles on MR images is predictive of poor facial function after grafting. Asymmetric facial muscles on preoperative MR images are associated with perineural tumor spread in patients with malignant disease.
Facial nerve paralysis is an uncommon but emotionally and physiologically devastating condition. These patients often have incomplete eye closure, which will cause corneal ulceration if not adequately addressed. They also may have trouble maintaining oral competence leading to drooling and difficulty chewing. These deficits are the result of muscle denervation. Skeletal muscle, when denervated, undergoes initial edematous pseudohypertrophy and then loss of myofibrils with fat and collagen deposition (1). Physiological denervation changes can be represented on MR images and CT scans. CT shows late denervation changes, such as asymmetrical muscle volume, fatty infiltration, and involvement of muscles sharing common innervation (2, 3). MR imaging is able to delineate more acute denervation changes, including muscle edema (4, 5) and abnormal enhancement (6–8). Other findings, such as abnormal muscle position, can also indicate muscle denervation (7).
When the facial nerve is resected as part of a surgical procedure, very good results can be expected with various grafting techniques, the most common of which is a cable interposition graft from the great auricular nerve or sural nerve (9–12). Best results are obtained when grafting is performed at the time of resection (9, 13). Most patients who undergo surgical resection of a tumor and the facial nerve will also undergo preoperative imaging. The purpose of this study was to evaluate preoperative facial muscle appearance on MR images, specifically to see whether the appearance of the muscles on the images correlates with preoperative facial function, whether the MR imaging appearance predicts final facial function after nerve grafting, and whether follow-up imaging provides useful information regarding final outcome.
Methods
A retrospective chart review was performed, searching for all patients who underwent facial nerve grafting at our institution between June 6, 1997, and July 31, 2001. Twenty-six patients were identified. Inclusion criteria for this study included preoperative imaging (either MR imaging or CT) that included facial muscles and a minimum of 12 months of postoperative follow-up. All patients included for final analysis had undergone preoperative MR imaging. Twelve patients (seven men and five women) met the criteria. Patient age ranged from 7 to 79 years. Follow-up duration ranged from 15 to 44 months, averaging 33 months. Four patients had benign tumors, including two acoustic neuromas, one intracranial seventh nerve schwannoma, and one recurrent benign mixed tumor of the parotid. Eight patients had malignant tumors. Four cases of recurrent skin cancer with extension into the parotid gland, two cases of adenoid cystic carcinoma of the parotid gland, and two cases of mucoepidermoid parotid carcinoma occurred. Seven patients underwent postoperative radiation therapy. Preoperative and postoperative facial function was graded by using the House-Brackmann scale (14). House-Brackmann grades I and II were considered excellent function, III and IV fair function, and V and VI poor function (15). Postoperative function was evaluated by using the May scale, which provides a method of evaluating individual branches of the facial nerve (16). The House-Brackmann scale is intended to assess global facial function and assumes an insult to the main trunk. Therefore, all branches would be affected. The May scale is designed specifically to assess function after facial nerve grafting. For this study, May grade III or better was considered to be a good outcome and grade IV or worse was considered to be a poor outcome. May further classifies outcomes ranging from superb to poor. Three different types of grafts were used: nine sural nerve grafts, two great auricular nerve grafts, and one hypoglossal to facial graft. The pathology reports were evaluated for perineural invasion of tumor within the specimen and at the margins.
All images were reviewed by the senior author (J.L.W.), who was not informed of the patient’s diagnosis, side of lesion, or final outcome, although for several patients, the primary lesion was visible on the preoperative images. The facial muscles were evaluated and categorized as symmetrical or asymmetrical. The asymmetrical group was further divided into mild or pronounced asymmetry. Follow-up images, if available, were evaluated by using the same criteria.
Results
All muscles of facial expression that were included on images were evaluated. Four patients had symmetrical facial muscles (Fig 1) seen on preoperative MR images, three had mild asymmetry (Figs 2 and 3), and five had pronounced asymmetry (Figs 4–6). All asymmetrical findings were on the ipsilateral side of the lesion. Five (72%) of seven patients with normal or mildly asymmetrical facial muscles shown by preoperative imaging had good preoperative facial function. Three patients with pronounced asymmetry of facial muscles had excellent preoperative facial function, one had fair function, and one had poor function (Fig 7). Six of the seven patients with symmetrical or mildly asymmetrical facial muscles shown on preoperative MR images had good to superb facial function outcome (Fig 8). Imaging that showed normal or mildly asymmetrical facial muscles had an 86% positive predictive value for at least a good outcome. Four (80%) of the five patients with pronounced asymmetry of facial muscles experienced poor results after nerve grafting.

Axial MR image of patient with symmetrical facial muscles (arrows).

Axial MR image of patient with mild atrophy of the right buccinator (large solid arrow) and normal left buccinator (small open arrow).

Axial MR image of patient with mild atrophy of left facial muscles (large arrow) compared with right facial muscles (small arrow).

Images of patient with pronounced asymmetry.
A, Sagittal view MR image shows normal left orbicularis (long arrow) and normal left frontalis (short arrow).
B, Image of same patient shown in A shows pronounced atrophy of right orbicularis (long arrow) and frontalis (short arrow).

Coronal view MR image shows pronounced atrophy of the right platysma compared with left (arrows).

Axial view MR image shows pronounced atrophy of left facial muscle compared with right (arrows).
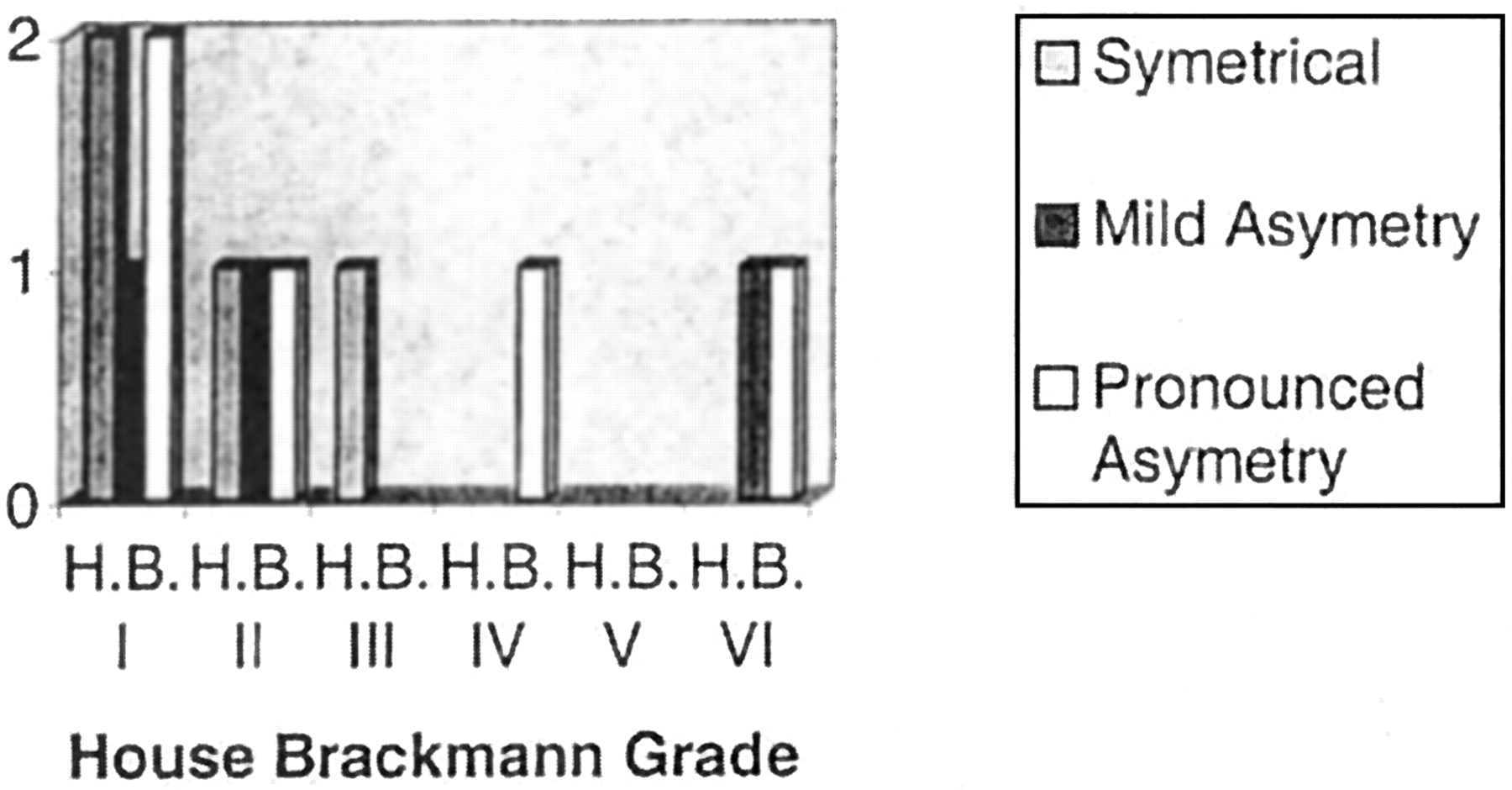
Graph shows House-Brackmann grades for preoperative imaging and preoperative facial function.

Graph shows May grades for preoperative imaging and final facial function after nerve grafting.
Six of eight patients with malignant tumors had perineural invasion of tumor revealed by pathologic evaluation. All patients with perineural invasion of tumor had some degree of muscle atrophy on the ipsilateral side. Four of the six patients had pronounced facial muscle asymmetry shown on preoperative MR images, and two had mild asymmetry of the facial muscles. Three of the four patients with pronounced asymmetry shown on preoperative images had excellent preoperative facial function. After grafting, one patient achieved a fair result and two experienced complete paralysis whereas the fourth patient, who had poor preoperative facial function, experienced a poor grafting result (Fig 9). Two patients with malignant tumors had perineural extension of tumor histologically ruled out, and both patients had normal preoperative facial muscle imaging findings and excellent facial function after grafting.

Chart compares preoperative imaging, preoperative facial function, and final facial function.
Follow-up MR images were available for six patients. Continued atrophy of the facial muscles was shown in two patients who ultimately experienced poor facial function, and greater atrophy of facial muscles was shown in two patients who achieved good outcomes. One patient had two follow-up studies available. The first, obtained 6 months after grafting, showed degeneration, and the second, obtained at 15 months, showed improvement of atrophy. The patient ultimately achieved good facial function. No change in the mild asymmetry that was shown by preoperative MR imaging was shown for one patient who achieved a good surgical result. Improvement of asymmetry at 6 months was shown for one patient who achieved good facial function.
Discussion
Facial paralysis is psychologically and emotionally difficult for many patients. There are many causes of facial nerve paralysis, the most common of which is Bell palsy (17). Tumors account for 5% of all cases of facial nerve paralysis but are the cause of 35% of cases being misdiagnosed as Bell palsy (17). Both benign and malignant tumors can cause facial weakness, and weakness can also be the result of surgical resection. Malignant tumors of the parotid gland often require resection of the facial nerve to provide oncologically sound surgery (10). Skull base procedures for benign tumors, such as acoustic neuromas, seventh nerve schwannomas, glomus tumors, and meningiomas, can also result in facial nerve injury and paralysis (11, 12). Iatrogenic injury, trauma, and infectious agents are additional causes of facial nerve paralysis (11, 12, 17). Regardless of the cause, it is in the patients’ best interest to restore facial function to be as nearly normal as possible. Facial nerve grafting is a reliable technique for restoring facial nerve continuity, and final function is often acceptable (9, 10, 12, 13, 18).
Most patients who undergo skull base procedures or radical parotidectomies will also undergo preoperative MR imaging. It would be beneficial to the patient and the surgeon if there were a test that could provide the patient and the surgeon with realistic expectations for recovery before surgery. Several factors have been shown to have negative prognostic implications for patients undergoing facial nerve grafting, including presence of preoperative palsy, duration of palsy, and patient age >60 years (9, 13, 18). Normal symmetry or mild asymmetry of the facial muscles had an 86% positive predictive value for good final outcome, whereas pronounced asymmetry of the facial muscles had an 80% chance of poor outcome. These results indicate that facial muscle appearance on MR images is predictive of final facial nerve function after nerve grafting.
Eight patients in this study had malignant tumors, and six of them were shown by pathologic evaluation to have perineural invasion. The two patients who did not have tumor involving the facial nerve had normal facial muscle symmetry shown by imaging and achieved excellent final facial outcomes. All the patients with perineural spread, however, had asymmetrical facial muscles shown by imaging and experienced fair to poor outcomes. In addition, three patients who clinically had normal facial function but had perineural invasion of tumor experienced poor recovery of facial function. Subacute denervation patterns were identified by Fischbein et al (3) in patients with confirmed perineural spread of tumor. It seems that MR imaging is a sensitive indicator of perineural spread, and muscle asymmetry, as seen on MR images, may be an earlier finding of facial nerve involvement than facial palsy.
Nerve and muscle degeneration and regeneration are orderly processes that have been well described (1, 19), and MR imaging findings reflect the biology of denervated muscles. Injury to motor nerves results in an orderly neuronal and muscular degeneration and regeneration process. These events occur in four places: the neuron body, proximal axon, distal axon, and muscle (1, 19). Axonal sprouting occurs at the proximal stump during attempts to reinnervate the muscle (19). Several patients had signs of muscle atrophy revealed by preoperative MR imaging but had normal facial function. It may be that a critical mass of functioning muscle allows a patient to have normal function. It is possible that these patients, although they had pronounced asymmetry, were able to compensate and achieve normal physical examination results. Histologic evidence of regeneration can be found within 7 hr of injury and can continue for several months (19). Muscles go through a process of atrophy and then fibrosis and fatty infiltration during the degeneration process (1). These physiological changes have been described as acute, subacute, and chronic MR denervation changes (4, 20).
Similar MR imaging findings have been noted in head and neck muscle groups. Russo et al (8) described acute, subacute, and chronic denervation patterns in the tongue and muscles of mastication after denervation injuries. Chronic changes that were seen in the tongue and muscle of mastication were muscle enhancement T2 prolongation, increased muscle volume, and fatty infiltration. Similar findings were described for the muscles of mastication in a patient with a known pontine hemorrhage (21). Fischbein et al (3) described subacute denervation changes, including T2 prolongation and contrast enhancement, for two patients with pathologically proved perineural invasion of malignant tumors along the facial nerve. Romo and Curtin (7) also showed that atrophy of the posterior cricoarytenoid muscle indicates recurrent laryngeal nerve palsy. In this study, the chronicity of the denervation was difficult to appreciate because the muscles of facial expression are much smaller than the muscles of the tongue or mastication. Subtle changes indicating length of denervation were not seen, and changes in muscle volume were the main indicator of facial muscle denervation.
Follow-up imaging is often ordered after surgical resection of malignant tumor to assess for recurrence. Six patients in this study had undergone postoperative imaging at various time intervals. Degeneration of facial muscle symmetry was shown for four patients; two ended with poor facial function, and two subsequently achieved excellent facial function. One of the patients who showed initial degeneration underwent subsequent MR imaging at 15 months postoperatively. The imaging showed improving symmetry, at which time the patient’s facial muscle function was improving. It is possible that the condition of the facial muscles seen on later follow-up images is reflective of ultimate function. One patient for whom no change in preoperative mild asymmetry was shown achieved excellent results, as revealed by follow-up MR imaging. One patient for whom improvement of symmetry was shown on the initial postoperative images ended up achieving an excellent result. It is possible that patients who experience no worsening of asymmetry and those who achieve initial improvement gain good facial function, whereas if degeneration is revealed by postoperative imaging, good results are not as likely.
Conclusion
Mild asymmetry or normal symmetry of facial muscles seen on preoperative MR images is strongly suggestive of good final facial function after nerve grafting. On the other hand, pronounced asymmetry of facial muscles on MR images is predictive of poor facial function after grafting. Patients who have pathologically confirmed perineural invasion have poor final function, even with normal preoperative facial function. Facial muscle asymmetry on preoperative images seems to be a sensitive predictor of perineural invasion, and these MR imaging changes may precede clinical facial palsy. Preoperative imaging may be helpful in predicting recovery of facial function.
Acknowledgments
The authors thank Peter E. Andersen, MD, Sean O. McMenomey, MD, and James I. Cohen, MD, for contributions to this study and for performing most of the operations for this study.
References
- Received May 30, 2002.
- Accepted after revision July 16, 2002.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.