
Abstract
BACKGROUND AND PURPOSE: To develop an MR imaging method that improves detection of leptomeningeal disease when compared with the current reference standard, contrast-enhanced T1-weighted imaging.
METHODS: We investigated the cases of 10 children who were at high risk of intracranial leptomeningeal disease (Sturge-Weber syndrome and medulloblastoma). The cases of Sturge-Weber syndrome were investigated by using one MR imaging examination, and the cases of medulloblastoma were investigated by using four MR imaging examinations performed over 18 months. In all cases, contrast-enhanced fluid-attenuated inversion recovery (FLAIR) images were acquired in addition to the routine sequences. The parameters of the FLAIR sequence were chosen to maximize the T1 component of the signal intensity, to maximize detection of leptomeningeal enhancement. We made subjective and objective assessments of the presence and extent of leptomeningeal disease as shown on contrast-enhanced T1-weighted images and contrast-enhanced FLAIR images.
RESULTS: In three of the four cases of Sturge-Weber syndrome, the T1 and FLAIR sequences showed comparable extent of leptomeningeal enhancement. For one child, FLAIR images showed unexpected bilateral disease and more extensive leptomeningeal enhancement on the clinically suspected side. In four of six cases of medulloblastoma, no leptomeningeal enhancement was shown on any examinations during the 18-month period. In two cases, FLAIR images showed more extensive leptomeningeal enhancement when compared with T1-weighted images.
CONCLUSION: Contrast-enhanced FLAIR imaging seems to improve detection of leptomeningeal disease when compared with routine contrast-enhanced T1-weighted imaging. This seems to be partly because of suppression of signal intensity from normal vascular structures on the surface of the brain by FLAIR, which allows easier visualization of abnormal leptomeninges. We think that these findings can be extrapolated to the investigation of leptomeningeal disease of all causes and at all ages.
Contrast-enhanced T1-weighted imaging is the standard method of detecting brain and spine lesions characterized by disruption of the blood-brain barrier. It is also the most sensitive imaging method of detecting leptomeningeal infiltration by tumor (1). This is increasingly recognized as a complication of metastatic disease from non-CNS sites in adults as more MR imaging is performed. Recognition of leptomeningeal disease is of fundamental importance in pediatric neuroimaging because it frequently occurs as a complication of some primary brain tumors and has major implications for treatment and prognosis. Contrast-enhanced T1-weighted imaging is a powerful tool in this respect, particularly in distinguishing between leptomeningeal enhancement, which is usually due to infiltration, and pachymeningeal enhancement, which is usually a secondary response to cranial surgery and/or shunt placement. The detection of leptomeningeal disease, however, can be difficult because normal meninges enhance to some degree and T1 shortening due to contrast agent in normal vascular structures may cause confusion.
We became interested in fluid-attenuated inversion-recovery (FLAIR) imaging of leptomeningeal disease because of two observations. First, our work with detection of subarachnoid hemorrhage by MR imaging showed that FLAIR was good at detecting T1 shortening caused by blood in the subarachnoid space (2), a finding that is gaining acceptance in the neuroradiologic literature. In addition, we described a new finding in a recent study investigating changes in brain perfusion after carotid stent placement. We showed leptomeningeal enhancement overlying the cerebral hemisphere supplied by the treated carotid artery (3). This was best shown on FLAIR images that were obtained to look for areas of ischemia after stent placement.
We herein describe our experience in using a modified FLAIR sequence to look for leptomeningeal disease in two situations in pediatric neuroradiology in which we would expect a high frequency of involvement: benign leptomeningeal angiomatosis associated with Sturge-Weber syndrome and malignant infiltration by medulloblastoma.
Methods
Patients
We describe the imaging of 10 children who presented to our department for clinical MR imaging examinations with presumptive diagnoses of either Sturge-Weber syndrome or medulloblastoma during a 6-month period from 1999 to 2000. Six children had a final diagnosis of medulloblastoma confirmed by histology and had an age range of 1.5 to 7 years at the time of the initial MR imaging examination. Four children were shown to have Sturge-Weber syndrome by a combination of clinical and radiologic findings. They had an age range of 7 to 11 years at the time of the MR imaging examination.
MR Imaging Methods and Analysis
All MR imaging examinations were performed on a 1.5-T superconducting system (Eclipse, Philips Medical Systems). Children with suspected Sturge-Weber syndrome were investigated by routine multiplanar, multi-sequence MR imaging supplemented by MR venography, perfusion imaging, and spectral fat saturation contrast-enhanced orbits as appropriate. FLAIR imaging was performed immediately before the routine axial view T1-weighted MR imaging, after the injection of weight-dependant volumes of contrast agent (Magnevist (dimeglumine gadopentetate); Schering AG, Berlin, Germany).
For the children being investigated for possible medulloblastoma, a standardized protocol, as defined by the United Kingdom Children’s Cancer Study Group and Societe Francaise d’Oncologie Pediatrique Panelists (4), was used but also included axial view FLAIR imaging of the brain after the injection of weight-dependant volumes of contrast agent. FLAIR imaging was performed immediately before the routine axial view T1-weighted MR imaging at the time of the initial and all follow-up procedures. Four MR imaging procedures were reviewed for each child: the presentation examination and 6-, 12-, and 18-month follow-up examinations. The sequence used in both patient groups was identical. The protocol for the fast spin-echo FLAIR imaging was as follows: 6000/95.9 (TR/TE); inversion time, 1800 ms; echo train length, 8; field of view, 20 cm; matrix, 192 × 256; number of sections, 20; section thickness, 4 mm; section gap, 2 mm.
Two neuroradiologists assessed the contrast-enhanced T1-weighted and FLAIR images with full clinical information available. Both reporters were asked to independently state whether abnormal leptomeningeal enhancement was present. In cases in which leptomeningeal enhancement was present, an objective assessment of the extent was made by each neuroradiologist some weeks after the original report. This was performed by tracing the extent of the abnormality on the axial view sections by using software on the proprietary workstation. Significant differences between the T1-weighted and FLAIR sequences were arbitrarily defined if both reviewers found a difference in the linear measurements of >20% on a single section.
Results
Complete agreement existed between both reviewers regarding the presence or absence of abnormal leptomeningeal enhancement when the contrast-enhanced T1-weighted and FLAIR images were assessed independently. Three of the four children with Sturge-Weber syndrome had intracranial manifestations of Sturge-Weber syndrome, including leptomeningeal angiomatosis, confirmed by both reporters. The fourth had V1 flammeus naevus and glaucoma recognized clinically and ipsilateral diffuse choroidal angioma defined by imaging. In two of the four cases, the T1-weighted and FLAIR sequences showed comparable extent of leptomeningeal enhancement. Both imaging sequences showed no leptomeningeal involvement in one of the four cases. In one of the four cases, FLAIR imaging showed unexpected bilateral disease and more extensive leptomeningeal enhancement on the clinically suspected side. This had major clinical relevance because the child was being assessed for possible hemispherectomy for intractable seizures (Fig 1).

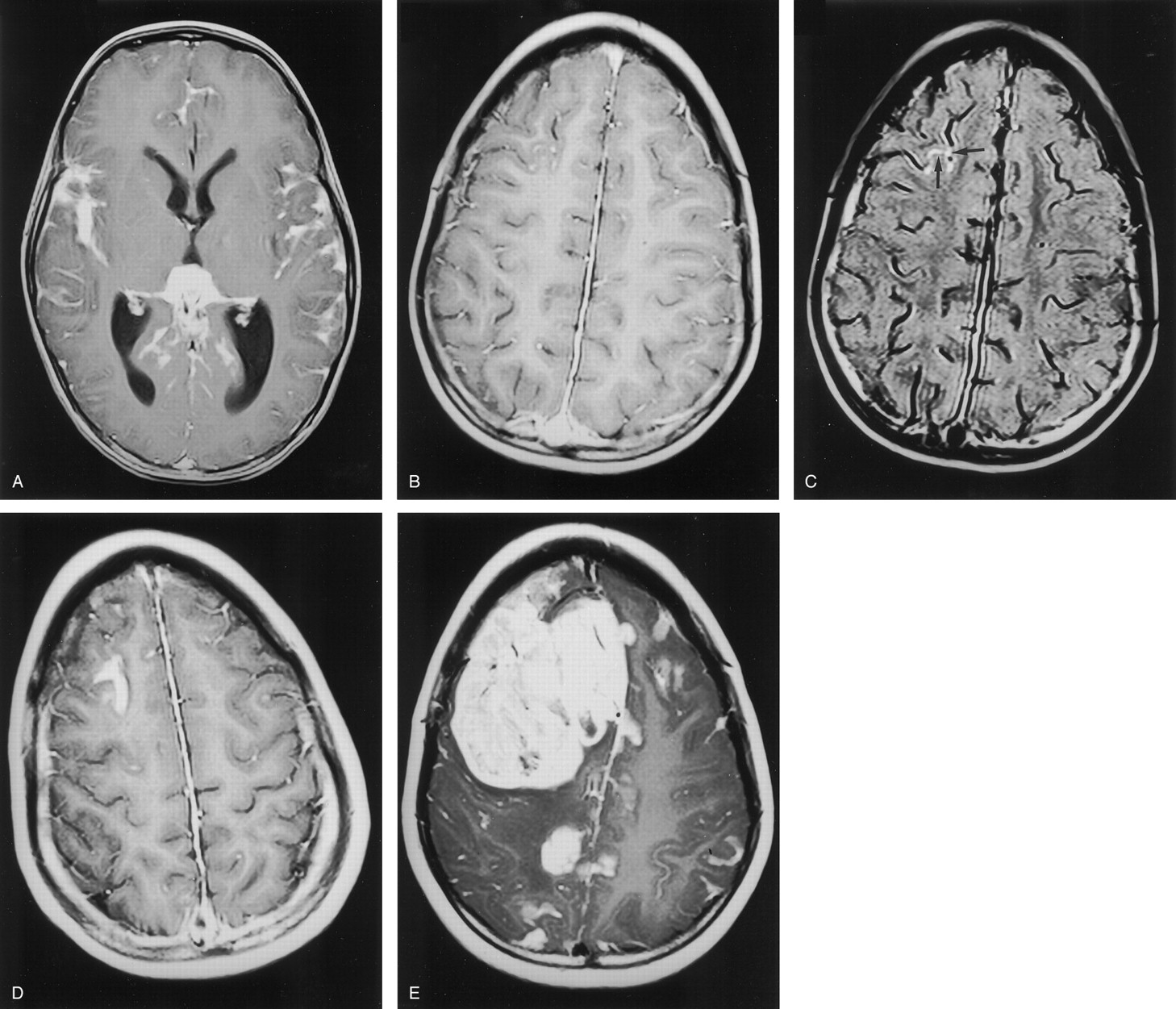
Images from the case of a 9-year-old child with suspected left-sided Sturge-Weber syndrome.
A, Axial view contrast-enhanced T1-weighted image obtained at the level of the Monro foramina. Note the prominent but normal enhancement of vascular structures in the right hemisphere.
B, Axial view contrast-enhanced FLAIR image obtained at the level of the Monro foramina shows the improved visualization of leptomeningeal disease in the left temporal lobe. Note that enhancement of normal vascular structures in the right hemisphere is suppressed.
C, Axial view contrast-enhanced T1-weighted image obtained toward the vertex.
D, Axial view contrast-enhanced FLAIR image obtained toward the vertex shows considerably more enhancement in the left frontal lobe as compared with the T1-weighted image. More importantly, abnormal leptomeningeal enhancement is shown over the right frontal lobe, indicating bilateral disease. The presence of bilateral disease precluded surgical intervention.
Four of the six children with medulloblastoma had no leptomeningeal enhancement shown by any of the four examinations during the 18-month follow-up period. In one of six cases, abnormal leptomeningeal enhancement consistent with metastatic disease was shown at presentation and was shown again at the three subsequent follow-up examinations on both T1-weighted and FLAIR images. The degree of abnormal leptomeningeal enhancement varied considerably during follow-up but was always shown to be more extensive on FLAIR images (Fig 2), as assessed by both reviewers reviewing the images together. In one of six cases, abnormal leptomeningeal enhancement was absent at the first two examinations but was confidently defined on FLAIR images but not on T1-weighted images at the third examination. By the fourth examination, a solid, malignant deposit had developed at that site (Fig 3).
Images from the case of a 3-year-old patient who presented with early morning headache and vomiting headache. A mass in the fourth ventricle was shown to be a medulloblastoma.
A, Axial view contrast-enhanced T1-weighted image obtained at presentation showed extensive leptomeningeal spread.
B, Significant response to treatment was achieved by 6 months, with no residual disease evident on the T1-weighted image.
C, Contrast-enhanced FLAIR image did show leptomeningeal enhancement in the right frontal lobe (arrows) that could be seen in retrospect on the T1-weighted image.
D, Contrast-enhanced T1-weighted image obtained at 12 months showed progressive disease in the right frontal lobe.
E, Contrast-enhanced T1-weighted image obtained at 18 months also showed progressive disease in the right frontal lobe.

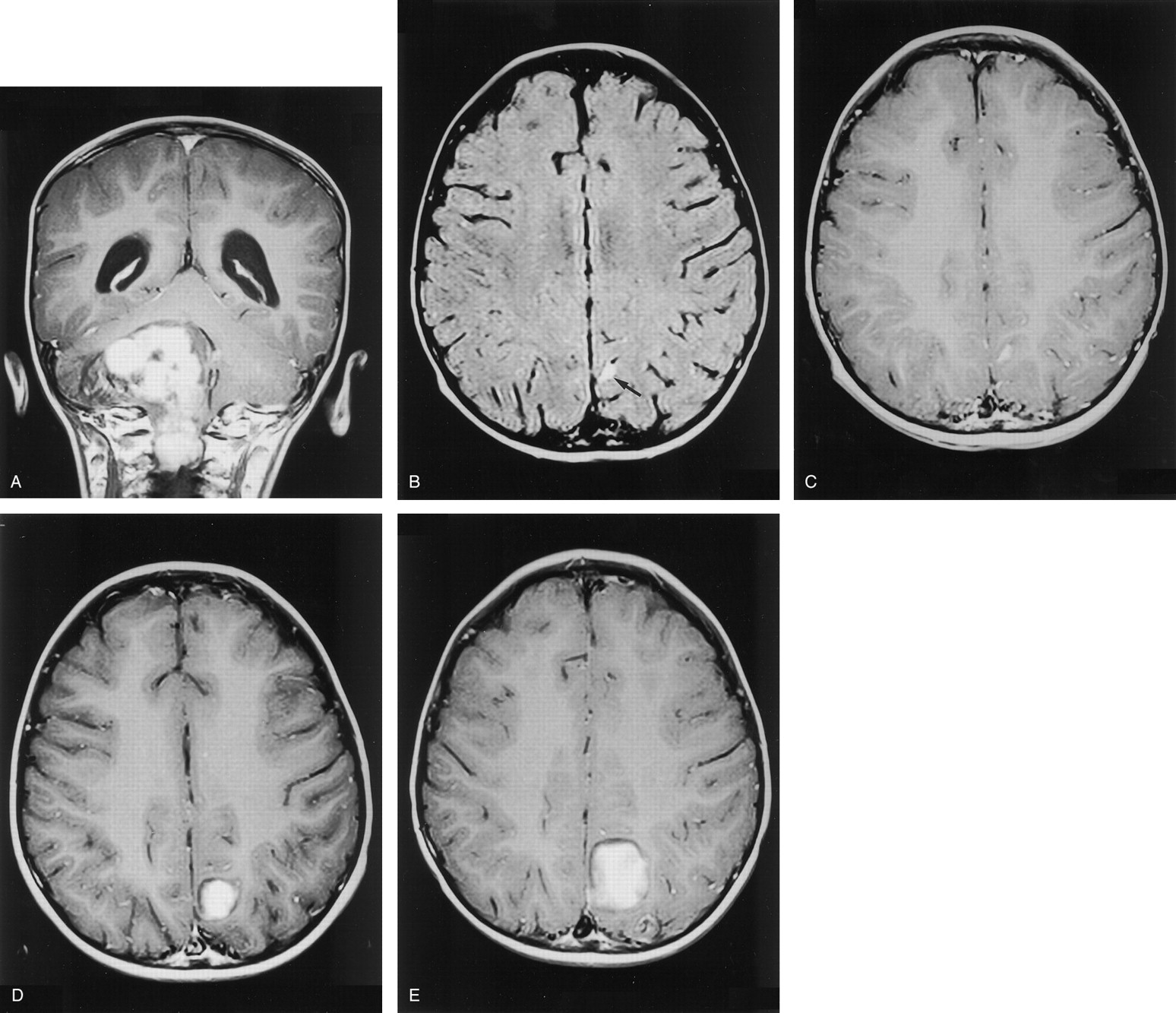
Images from the case of a 2-year-old patient who presented with symptoms and signs suggestive of a posterior fossa mass.
A, Coronal view contrast-enhanced T1-weighted image shows a large mass centered in the right cerebellar hemisphere that was confirmed to be medulloblastoma. No evidence of intracranial metastases was observed at presentation.
B, Contrast-enhanced FLAIR image obtained at 6 months shows definite abnormality in the meninges overlying the left parietal lobe (arrow).
C, In retrospect, this region is viewed as abnormal on the contrast-enhanced T1-weighted image, although it was reported as normal.
D, Contrast-enhanced T1-weighted image obtained at 12 months shows definite progression.
E, Contrast-enhanced T1-weighted image obtained at 18 months also shows definite progression.
Discussion
Detection of leptomeningeal disease based on images was difficult before the introduction of MR imaging. CT methods are not ideal in this role because enhancement after the injection of iodine-based agents is often directly related to attenuated cortical bone. The beam hardening and streak artifact caused at the bone-soft tissue interface severely reduces the sensitivity of the method. This is particularly pronounced at the skull base. Practically, CT was performed to exclude intracranial mass lesions that might contraindicate the reference standard method of detection (ie, lumbar puncture with cytologic investigation). MR imaging with IV administered contrast agents has several advantages over CT in this application, the main considerations being lack of signal intensity from cortical bone, no artifacts, and the ease with which multiplanar imaging can be performed. The sensitivity in detecting malignant leptomeningeal disease by MR imaging is greatly improved when compared with CT, although specificity remains low. Malignant leptomeningeal disease in adults is usually due to metastatic disease from non-CNS causes, and detection has a major impact on clinical management. In children, leptomeningeal disease is usually metastatic or contiguous from primary brain tumors and its detection also has a significant effect on management, particularly regarding the extent of primary resection.
We have presented our early experience in using a contrast-enhanced FLAIR sequence in detecting leptomeningeal disease in two, highly selected pediatric populations: patients with Sturge-Weber syndrome and patients with medulloblastoma. These groups were chosen because of the expected high frequency of leptomeningeal disease that is required when making an initial assessment of a new indication for this sequence. We have shown distinct advantages of contrast-enhanced FLAIR imaging over standard contrast-enhanced T1-weighted imaging of these patients, in terms of sensitivity and certainty of diagnosis. It is interesting to speculate regarding why contrast-enhanced FLAIR imaging may be better than T1-weighted imaging and whether any confounding factors exist that may influence the signal intensity on FLAIR images other than the accumulation of contrast agent. Deliganis et al (5) described eight patients who showed increased signal intensity from CSF in the basal cisterns and over the cortical sulci on unenhanced FLAIR images when inhaled oxygen levels were increased. All our pediatric patients were examined while under general anesthesia by the same anesthetist who used 33.3% oxygen, as is the case for most of our pediatric patients. Unenhanced FLAIR imaging was not performed in our cases, but we have never seen focal increased signal intensity in the meninges of anesthetized children when FLAIR sequences have been used. We do not think, therefore, that this mechanism is relevant in our cases. In our experience, the major advantage of contrast-enhanced FLAIR imaging over contrast-enhanced T1-weighted imaging is lack of enhancement in the normal vascular structures on FLAIR images compared with T1-weighted images. Any sequence that can reduce or eliminate signal intensity from normal vasculature constitutes a significant step forward. It should be noted that this observation is not due to reducing concentrations of contrast agent as it is excreted; in all our patients, the FLAIR sequence was obtained before the T1 sequence and should have experienced higher concentrations of contrast agent. The reason for the suppression of signal intensity from vascular structures is likely to be vascular flow: the contrast agent-containing blood, which is initially tagged by the inversion pulse, may not be present in the imaging section during the readout time window. This results in no enhancement within the normal vascular structures.
Conclusion
We have shown that contrast-enhanced FLAIR imaging can be a valuable method for assessing abnormal leptomeninges. The present study dealt with only small numbers of pediatric patients with only two pathologic conditions. We think, however, that the sequence will show the same diagnostic improvements for other pediatric disorders characterized by abnormal leptomeninges (eg, pial synangiosis associated with moyamoya disease) and in adults with comparable disorders.
Acknowledgments
The authors acknowledge the skill and hard work of the MR radiographers at the University of Sheffield who made this study possible. Please note that P.D.G. is the Schering Professor of Radiology at the University of Sheffield, although Schering AG, Berlin, made no direct financial input into this study.
- Received March 11, 2002.
- Accepted after revision October 16, 2002.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Leptomeningeal Enhancement in Multiple Sclerosis and Other Neurological Diseases: A Systematic Review and Meta-Analysis
- Leptomeningeal gadolinium enhancement across the spectrum of chronic neuroinflammatory diseases
- Gadolinium-based MRI characterization of leptomeningeal inflammation in multiple sclerosis
- Elevated Cerebral Blood Volume Contributes to Increased FLAIR Signal in the Cerebral Sulci of Propofol-Sedated Children
- Comparison of the Added Value of Contrast-Enhanced 3D Fluid-Attenuated Inversion Recovery and Magnetization-Prepared Rapid Acquisition of Gradient Echo Sequences in Relation to Conventional Postcontrast T1-Weighted Images for the Evaluation of Leptomeningeal Diseases at 3T
- A Spectrum of Unusual Neuroimaging Findings in Patients with Suspected Sturge-Weber Syndrome