
Abstract
Summary: The authors present 3 patients who underwent neuroendovascular procedures in which DynaCT produced by a flat-panel detector facilitated management of complications. As part of a combined CT/angiography suite, DynaCT offered the major advantage of immediate detection or exclusion of intracranial complication without patient transfer. The quality of cone-volume CT-generated images produced by DynaCT was sufficient to make a diagnosis.
For patients undergoing neuroendovascular procedures such as intracranial aneurysm coiling, earlier recognition and management of complications can improve clinical outcomes.1–3 When a complication occurs during a neuroendovascular procedure, the patient is usually transported emergently from the angiography suite to the nearest CT scanner to determine a diagnosis. This protocol can endanger the patient not only from the transport itself but also from the delay in critical decision making. To overcome this shortcoming, Siemens has developed a new combined angiography/CT suite that uses flat-panel detector (FD) technology for higher-resolution angiography that is also capable of producing improved cone-beam volume CT images. In this new suite, 3D rotational digital subtraction angiography (DSA) or cone-beam volume CT can be obtained interchangeably with the same FD C-arm motion without patient transfer.
Technique
A biplane flat-panel detector angiographic suite (AXIOM Artis FD Biplane Angiosuite with DynaCT; Siemens Medical Solutions, Erlangen, Germany) was used (Fig 1A). A DynaCT acquisition was obtained by using the following parameters: 20-second rotation; 0.4° increment; 1024 × 793 matrix in projections at zoom 0 after resampling; 217° total angle; ∼11°/s, ∼27 frames/s, system dose 1.2 μGy/frame, total of 538 projections. Images were automatically corrected for gain of the image intensifier during the acquisition. Image reconstruction was performed on a commercially available dedicated workstation (X-Leonardo with DynaCT; Siemens Medical Solutions). Advanced postprocessing for beam hardening, scatter, and truncation correction was performed. The volume dataset produced with typical voxel size 0.4 mm by X-Leonardo was interactively viewed/windowed/leveled and manipulated in orthogonal planes (Fig 1B). The time required from acquisition to 3D-image rendering was 3–5 minutes. Radiation dose to patients was similar to that of a conventional CT head dose, up to 60 mGy. Differentiation of soft tissue densities was approximately 10 HU.

A, DynaCT acquisition demonstrating rotation of FD C-arm (curved arrow) during actual case. B, A screen shot of acquired orthogonal images immediately available to the user after acquisition and postprocessing.
Case Reports
Case 1
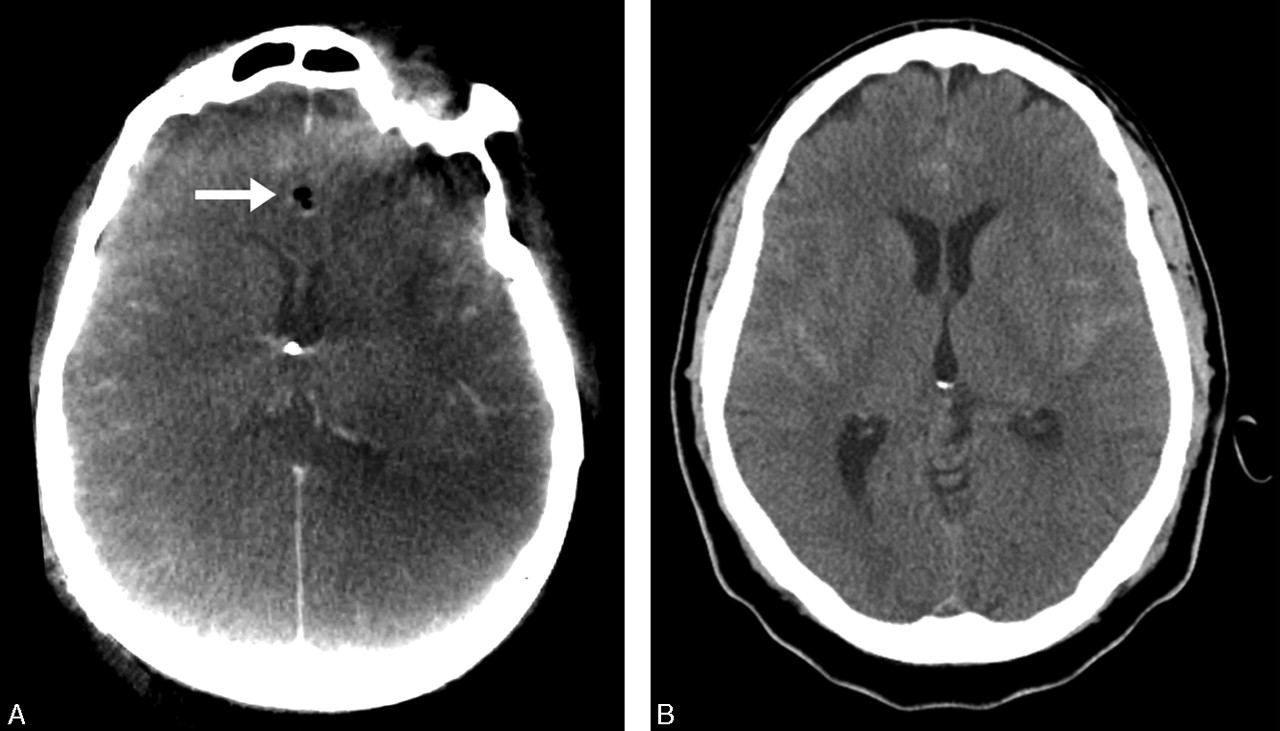
This 33-year old man, presenting with a grade III Hunt and Hess (H&H) subarachnoid hemorrhage (SAH), was treated for a ruptured left P2 posterior cerebral artery aneurysm. During the procedure, proximal to the aneurysm, vessel perforation occurred that was immediately treated with Guglielmi coil detachment. With the patient on the angiography table, DynaCT was then urgently performed, which, compared with preprocedure CT, demonstrated increased SAH and new intraventricular blood and acute hydrocephalus, despite the presence of a ventriculostomy catheter (Fig 2A, -B). In the angiography suite, another ventriculostomy catheter was emergently placed. The patient was transferred to the intensive care unit and on awakening from anesthesia, he was found to be neurologically unchanged.

DynaCT was performed following vessel perforation (A ) and demonstrated increased ventriculomegaly compared with preoperative CT scan (B).
Case 2
This 51-year-old man, presenting with a grade I H&H SAH, underwent coiling of an anterior communicating artery aneurysm. After coiling, the contralateral right A2 became compromised secondary to thrombus. Treatment with 8 mg of intra-arterial abciximab (ReoPro) resulted in complete recanalization of the right A2 and distal anterior cerebral artery segments but not in aneurysm reopening after closure with coils. At the end of the procedure, the patient suddenly became hypotensive and was noted to be in ventricular fibrillation. Immediate resuscitation was begun. We suspected an aneurysm rehemorrhage and, as part of the resuscitation efforts, successfully placed an emergent ventriculostomy but without return of bloody CSF. Immediately after resuscitation efforts were stopped, postmortem DynaCT demonstrated no evidence of new hemorrhage or hydrocephalus when compared with the preoperative CT scan (Fig 3A, -B), which indicates a primary cardiac event.
This patient experienced cardiac arrest and aneurysm rehemorrhage was suspected. After emergent ventriculostomy placement, however, DynaCT (A) demonstrated no new intracranial hemorrhage, which indicates a primary cardiac event. Note good catheter placement and interhemispheric air (arrow). Preoperative CT scan (B) is shown for comparison.
Case 3
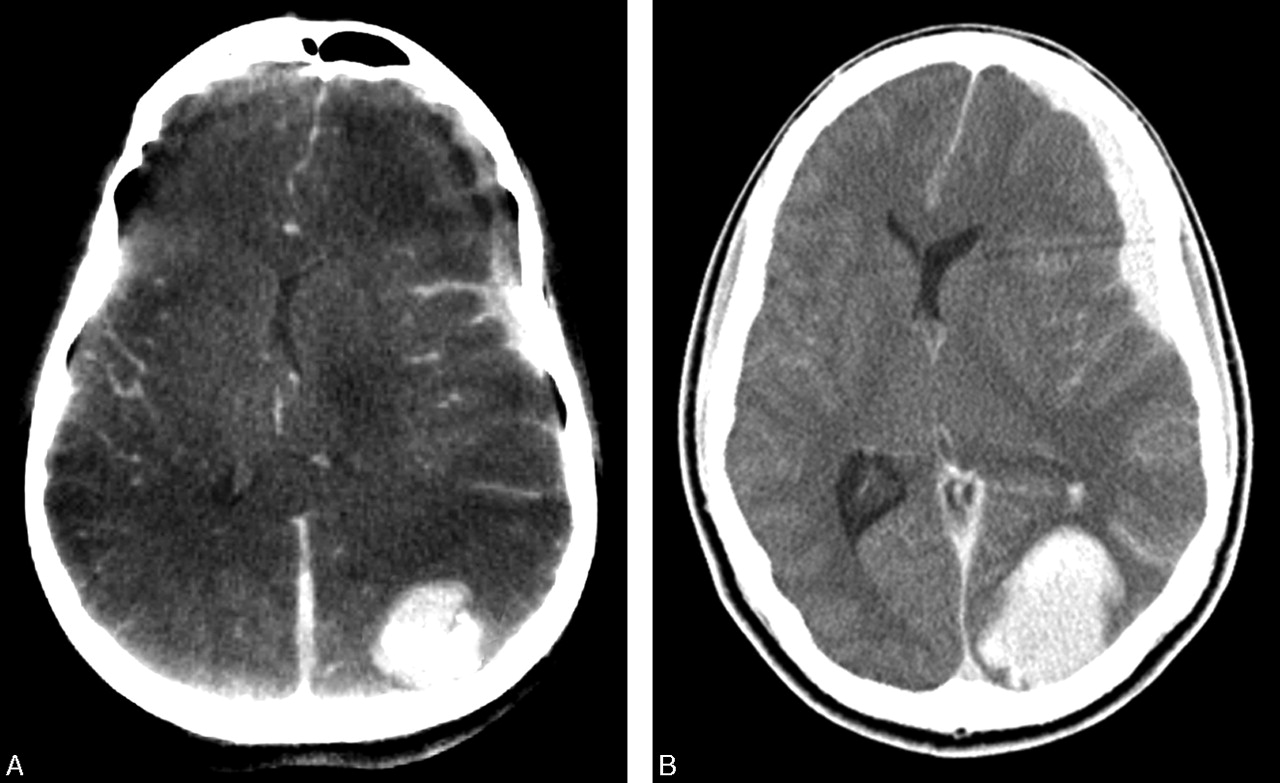
This 33-year-old man presented with decreased left visual acuity, intermittent right hemiparesis, and hemiparesthesias from a spontaneous extracranial left internal carotid artery (ICA) dissection. His left visual acuity worsened because of decreased retinal perfusion. Cerebral angiogram confirmed left ICA dissection “string” sign of the distal cervical ICA extending into the proximal petrous segment. The left ICA dissection was stented, which improved ICA caliber and antegrade flow. Control cerebral angiography of the left ICA, however, demonstrated left-to-right shift of the anterior cerebral artery branches indicating mass effect consistent with probable reperfusion hemorrhage. After immediate reversal of anticoagulation, DynaCTshowed an unexpected left subdural hematoma and focal left occipitoparietal intraparenchymal hemorrhage (Fig 4A). Emergent medical and surgical treatment for increased intracranial pressure was initiated. A conventional CT scan was performed (Fig 4B) before the patient was transferred to the operating room.

DynaCT (A) demonstrated unexpected subdural hematoma and occipitoparietal intraparenchymal hemorrhage. A conventional CT scan (B) was later obtained before patient transfer to the operating room, which revealed increased hemorrhage and mass effect.
Discussion
The images produced by DynaCT are not of the quality of conventional CT. Compared to non-FD cone-beam volume CT, DynaCT contrast images have improved spatial and resolution from lack of image distortion, higher detection dynamics, less sensitivity to overexposure, and higher efficiency.4 Despite initial concerns about inadequate image quality of the first-generation DynaCT images, our cases demonstrate that current DynaCT image quality is sufficient to make a diagnosis when a complication is suspected. In cases 1 and 3, in an operator- and time-convenient manner, while concurrently avoiding risky and time-consuming patient transfer, DynaCT enabled detection of intracranial hemorrhages and their extent within the angiography suite. Because DynaCT allowed earlier diagnosis and management of hemorrhagic complications, the extent of brain injury suffered by our patients may have been minimized.1–3 In case 2, a negative DynaCT reassured us that a suspected intracranial hemorrhage had not occurred. In case 1, after an emergent ventriculostomy was placed in the angiography suite, DynaCT immediately verified ventriculostomy placement. In the management of acute stroke, DynaCT can be performed to exclude intracranial hemorrhage before planned intra-arterial thrombolysis.5 Periprocedural DynaCT performed during brain or dural arteriovenous malformation embolization can detect obvious or occult hemorrhagic complications from vessel perforation or from venous penetration of embolic material or venous thrombosis.6,7 In head and neck embolization procedures using direct percutaneous access, in combination with biplane fluoroscopy, DynaCT can be used for more precise needle placement.
Conclusion
Within the angiography suite and without moving the patient, DynaCT enabled immediate detection or exclusion of intracranial hemorrhage and hydrocephalus, and its use facilitated the management of neuroendovascular complications.
Acknowledgments
The authors thank our outstanding radiology technologists who have worked tirelessly to improve DynaCT images: Mathew Joshua, Alex Eusebio, Danny Hom, Michael D. Lamon, and Virender Ahuja.
- Received June 7, 2005.
- Accepted after revision August 21, 2005.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Association of Contrast Enhancement After Reperfusion With Outcomes According to Blood Pressure Lowering in Patients With Acute Ischemic Stroke
- The impact of software-based metal artifact reduction on the liquid embolic agent Onyx in cone-beam CT: a systematic in vitro and in vivo study
- Imaging as a Selection Tool for Thrombectomy in Acute Ischemic Stroke: Pathophysiologic Considerations
- Clinical evaluation of volume of interest imaging combined with metal artifact reduction reconstruction techniques in coiling and stent assisted coiling during neurointerventional procedures
- Accuracy of image-guided percutaneous injection into a phantom spinal cord utilizing flat panel detector CT with MR fusion and integrated navigational software
- Latest generation of flat detector CT as a peri-interventional diagnostic tool: a comparative study with multidetector CT
- Three-dimensional image fusion of CTA and angiography for real-time guidance during neurointerventional procedures
- Intra-arterial versus intravenous abciximab therapy for thromboembolic complications of neuroendovascular procedures: case review and meta-analysis
- Metal artifact reduction for flat panel detector intravenous CT angiography in patients with intracranial metallic implants after endovascular and surgical treatment
- Accuracy of flat panel detector CT with integrated navigational software with and without MR fusion for single-pass needle placement
- The Added Value of Volume-of-Interest C-Arm CT Imaging during Endovascular Treatment of Intracranial Aneurysms
- Republished: Advanced digital subtraction angiography and MR fusion imaging protocol applied to accurate placement of flow diverter device
- Advanced digital subtraction angiography and MR fusion imaging protocol applied to accurate placement of flow diverter device
- Evaluation of a Metal Artifacts Reduction Algorithm Applied to Postinterventional Flat Panel Detector CT Imaging
- Effect of Structural Remodeling (Retraction and Recoil) of the Pipeline Embolization Device on Aneurysm Occlusion Rate
- Predictive value of flat-panel CT for haemorrhagic transformations in patients with acute stroke treated with thrombectomy
- The utility of cone beam volume CT in the evaluation of thrombosed intracranial aneurysms in subarachnoid hemorrhage
- Subarachnoid Hyperattenuation on Flat Panel Detector-Based Conebeam CT Immediately after Uneventful Coil Embolization of Unruptured Intracranial Aneurysms
- The utility of cone beam volume CT in the evaluation of thrombosed intracranial aneurysms in subarachnoid hemorrhage
- Frameless multimodal image guidance of localized convection-enhanced delivery of therapeutics in the brain
- A checklist for cerebral aneurysm embolization complications
- Initial experience with a combined multidetector CT and biplane digital subtraction angiography suite with a single interactive table for the diagnosis and treatment of neurovascular disease
- Flat Panel Catheter Angiotomography of the Spinal Venous System: An Enhanced Venous Phase for Spinal Digital Subtraction Angiography
- Monitoring Peri-Therapeutic Cerebral Circulation Time: A Feasibility Study Using Color-Coded Quantitative DSA in Patients with Steno-Occlusive Arterial Disease
- Transcranial Access Using Fluoroscopic Flat Panel Detector CT Navigation
- Use of Angiographic CT Imaging in the Cardiac Catheterization Laboratory for Congenital Heart Disease
- Flat Detector CT in the Evaluation of Brain Parenchyma, Intracranial Vasculature, and Cerebral Blood Volume: A Pilot Study in Patients with Acute Symptoms of Cerebral Ischemia
- Intraorbital access using fluoroscopic flat panel detector CT navigation and three-dimensional MRI overlay
- Feasibility of Angiographic CT in Peri-Interventional Diagnostic Imaging: A Comparative Study with Multidetector CT
- Color-Coded Digital Subtraction Angiography: The End of a Monochromatic Era?
- C-Arm CT Measurement of Cerebral Blood Volume in Ischemic Stroke: An Experimental Study in Canines
- DynaCT evaluation of in-stent restenosis following Wingspan stenting of intracranial stenosis
- Impact of Intra-Arterial Injection Parameters on Arterial, Capillary, and Venous Time-Concentration Curves in a Canine Model
- C-Arm CT Measurement of Cerebral Blood Volume: An Experimental Study in Canines