
Abstract
SUMMARY: We present the evolution of pituitary changes in the cases of 2 patients with Sheehan syndrome as assessed by MR imaging. Both patients had severe postpartum hemorrhage, symptoms of pituitary gland apoplexy, and hypopituitarism. Sequential MR imaging demonstrated evidence of ischemic infarct in the pituitary gland with enlargement followed by gradual shrinkage during several months, to pituitary atrophy.
Clinical recognition of Sheehan syndrome (hypopituitarism resulting from postpartum pituitary gland infarction after severe hypotension secondary to massive bleeding1) is often insidious, with the diagnosis being delayed for years.2 Pituitary imaging studies late in the course have revealed atrophy of the gland, resulting in a small empty sella.3,4 Rarely, patients present with pituitary apoplexy.2 MR imaging studies have been reported in only a few cases.5,6 We report the cases of 2 patients with Sheehan syndrome with acute presentations, in which the progression of pituitary gland changes was assessed by sequential MR imaging.
Case Reports
Case 1
A 29-year-old woman delivered a full-term baby. The delivery was complicated by retained placenta and profuse bleeding, requiring emergent embolization of the uterine artery. Her hemoglobin level fell to 3.8 g/dL. Several hours later, the patient developed a severe headache and nausea. A routine CT study of her head showed no abnormality. Her symptoms resolved, and she was discharged from the hospital without additional work-up. She returned on day 17 postpartum with fatigue, fever, mild headache, failure to lactate, and postural syncope. Her temperature was 101.2°F, pulse 122, and a supine blood pressure of 90/48 mm Hg. Examination showed skin pallor, a cardiac flow murmur, clear lungs, and a soft abdomen. Laboratory evaluation revealed anemia, mild hyponatremia (sodium, 134 mEq/L), and abnormal pituitary function test results (Table) consistent with panhypopituitarism.
Results of endocrine laboratory evaluation in Cases 1 and 2
MR imaging on postpartum day 26 (Fig 1) revealed a nonenhancing, minimally hypointense lesion in the pituitary gland. MR imaging 6 months postpartum (Fig 2) showed shrinkage of the pituitary gland with CSF signal intensity in the sella (“empty sella”). The pituitary infundibulum and hypothalamus appeared normal.

Case 1. Coronal (left) and sagittal (right) gadolinium enhanced T1-weighted MR images on postpartum day 26 show central low signal intensity and peripheral enhancement in the pituitary gland.

Case 1. Coronal (left) and sagittal (right) noncontrast T1-weighted MR images 6 months later show marked diminution in the size of the pituitary gland. There is CSF signal intensity in the sella (“empty sella”).
Case 2
A 21-year-old woman delivered a full-term healthy baby after labor was induced following premature rupture of membranes. During delivery, she sustained a fourth-degree perineal laceration with severe bleeding and hypotension (blood pressure, 60/30 mm Hg). Her hemoglobin level fell to 5.5 g/dL. Two days postpartum, the patient developed fever and a severe headache. The results of blood and urine cultures, pelvic sonography, and abdominal CT studies were negative. Fever resolved within 24 hours after the patient was given broad-spectrum antibiotics. The results of pituitary function tests obtained for hyponatremia (sodium, 116 mEq/L) demonstrated hypopituitarism (Table). Replacement therapy with prednisone and levothyroxine was begun. Her headaches resolved gradually, and she was discharged from the hospital on postpartum day 9.
MR imaging obtained on postpartum day 6 (Fig 3) showed an enlarged pituitary gland with suprasellar extension to the optic chiasm. There was no evidence of hemorrhage. Postgadolinium T1-weighted images showed peripheral enhancement of the swollen pituitary gland and an irregular and poorly enhanced central portion. MR imaging 5 weeks postpartum (Fig 4) revealed a smaller pituitary gland contained within the pituitary fossa. Nonenhancing areas persisted within the pituitary gland after administration of gadolinium. The pituitary stalk appeared normal. MR imaging obtained 11 months postpartum (Fig 5) showed marked atrophy of the pituitary gland resulting in an empty sella. There was now contrast enhancement of the pituitary remnant and the distal portion of the infundibulum.
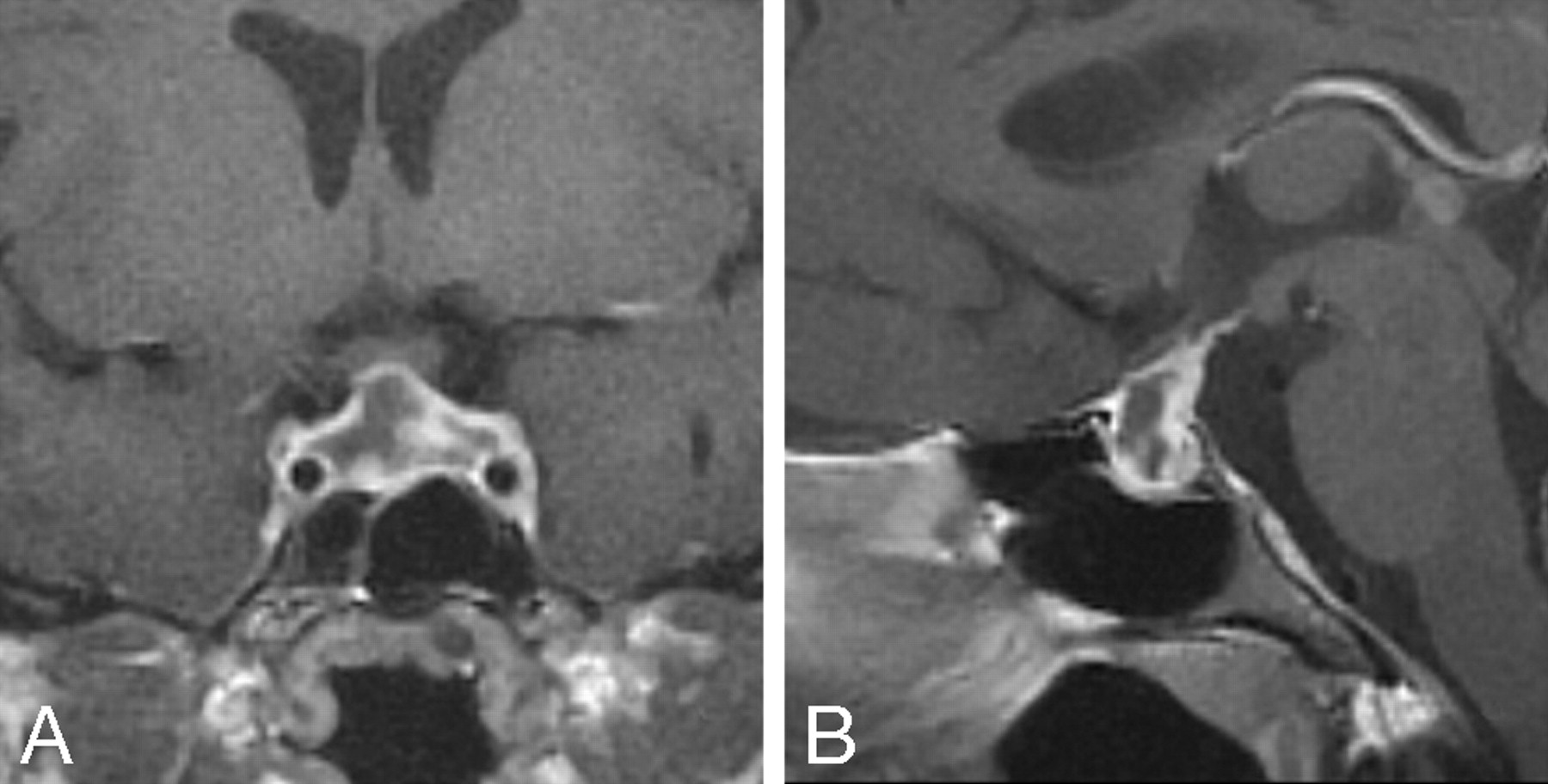
Case 2. Coronal (A) and sagittal (B) gadolinium-enhanced T1-weighted MR images on postpartum day 6 show a large low signal intensity sellar lesion with enhancement of the rim. There is extension into the suprasellar cistern, and the lesion abuts but does not compress the optic chiasm.

A and B, Case 2. At 5 weeks postpartum, the lesion is markedly smaller and no longer protrudes into the suprasellar cistern (image layout same as Fig 3).

Discussion
This case report describes the clinical and MR imaging findings of 2 patients with acute hypopituitarism after severe peripartum hemorrhage. Both cases were highly suggestive of ischemic infarction of the pituitary gland (Sheehan syndrome). MR imaging during the acute phase of Sheehan syndrome has been reported in 2 isolated cases,5,6 which, to our knowledge, are the only previous reports of time-dependent findings on MR imaging.
Although the number of reported cases is limited, some characteristic findings emerge. Acutely, MR imaging reveals an enlarged pituitary gland with central hypointensity on T1-weighted images and hyperintensity on T2-weighted images. These findings are consistent with pituitary infarction. Postgadolinium, the presumed infarcted areas are interspersed with perfused tissue, which manifests irregular enhancement. Within several weeks, the swollen pituitary gland regresses and is confined to the pituitary fossa, followed by further pituitary gland atrophy for several months. The end result is an empty sella of normal size.
The findings on MR imaging observed in Sheehan syndrome are not specific. During the acute phase of lymphocytic hypophysitis, there is more uniform contrast enhancement of a sellar or suprasellar mass7; however, in approximately 5% of reported cases, a cystic appearance is observed on MR imaging.7-9 In these cases, the findings on MR imaging can resemble those seen during the acute stages of Sheehan syndrome. This is relevant because lymphocytic hypophysitis is more common in women and typically presents in the peripartum and postpartum periods.7 Although hypopituitarism in lymphocytic hypophysitis may be transient, late-stage pituitary atrophy resulting in an empty sella has been reported in a case of biopsy-proved lymphocytic hypophysitis.10 Pituitary tumors typically show uniform enhancement on MR imaging, and the clinical distinction between a pituitary tumor and Sheehan syndrome is usually not difficult. However, tumors may exhibit central necrosis, in which case findings on MR imaging may mimic those seen during the acute phase of Sheehan syndrome.
Conclusion
The cases of our 2 patients, in conjunction with the previous cases of 2 patients reported in the literature, present a picture of the evolution of the findings on MR imaging in Sheehan syndrome that is consistent with the classic pathologic description. This evolution begins acutely with nonhemorrhagic changes in signal intensity consistent with central infarction, along with peripheral and heterogeneous central enhancement in an enlarged pituitary gland. The findings are consistent with patchy central ischemic necrosis and are followed by pituitary gland atrophy and an empty sella. These findings on MR imaging characterize Sheehan syndrome and provide early confirmation of the clinical diagnosis.
Footnotes
Previously presented in part at: Annual Meeting of the American Association of Clinical Endocrinologists, May 1–5, 2002; Chicago, Ill.
References
- Received October 16, 2007.
- Accepted after revision December 20, 2007.
- Copyright © American Society of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}