
We read with great interest the article of Turk et al,1 in which the authors describe their experience with restenoses after intracranial stent placement. In this article, most of the restenoses were diagnosed by means of conventional intra-arterial digital subtraction angiography (DSA) on routine follow-up investigations. Although DSA is currently the gold standard for detecting intracranial adjacent or in-stent restenosis (ISR), we would like to point out that less-invasive techniques for follow-up investigations should be considered, especially in patients with an increased risk for ISR, such as young and female patients.1 With respect to these techniques, we would like to report the following case.
A 48-year-old currently asymptomatic woman was seen in our institutional neurovascular clinic for a routine duplex follow-up investigation. Three months before presentation, a symptomatic intracranial stenosis of the right middle cerebral artery had been treated with an intracranial stent. The indication for the stent placement had been recurrent symptoms despite dual antiplatelet therapy (aspirin and clopidogrel).
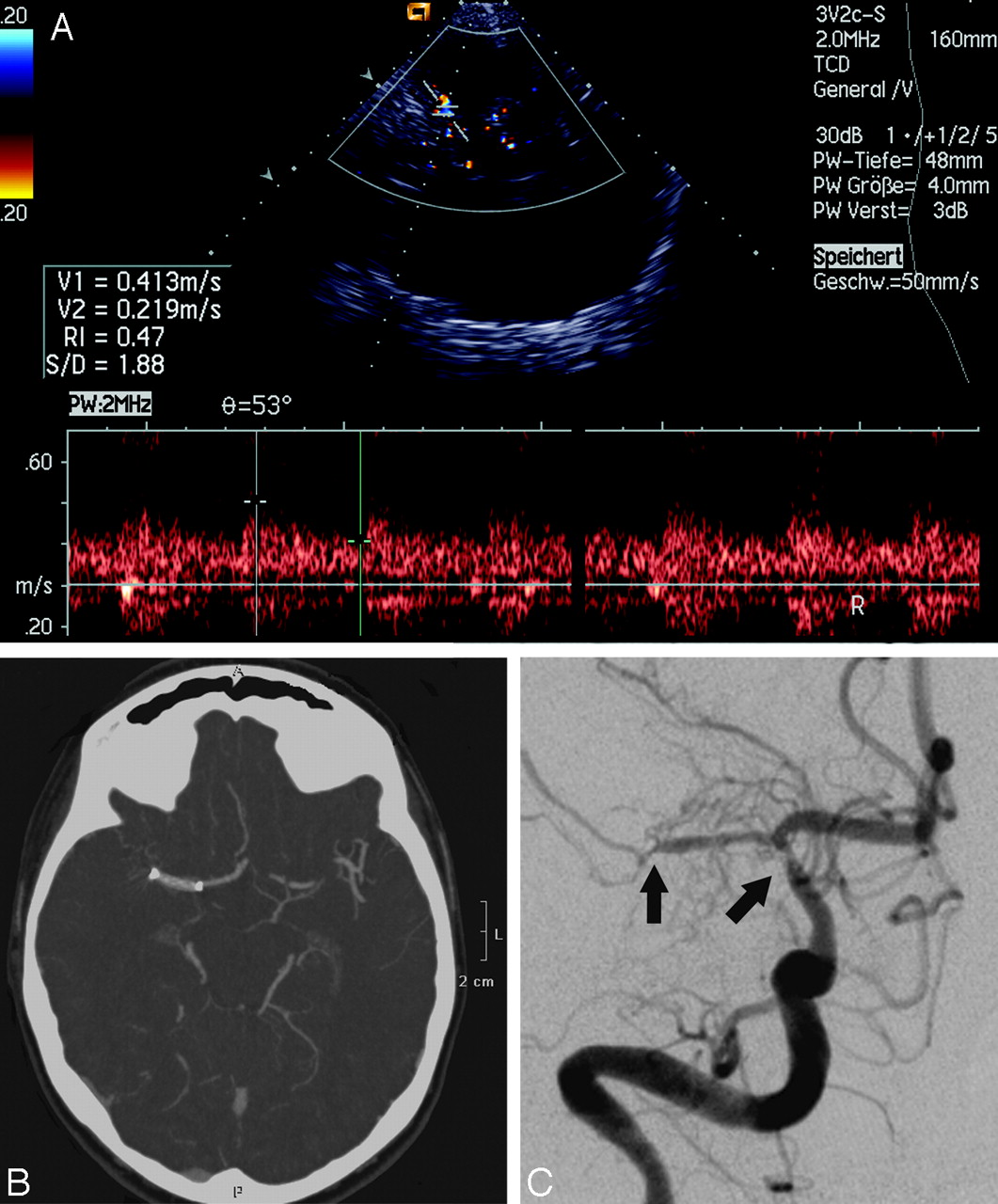
Transcranial duplex sonography revealed a blunted Doppler signal intensity with flattened systolic flow acceleration at the distal end of the stent (Fig 1A). CT angiography (Fig 1B) corroborated this finding showing a compromised arterial filling distal to the stent but failed to depict the stent lumen. Subsequent DSA (Fig 1C) documented bilateral stenoses on both sides of the stent.
This case illustrates that ISR can be assessed noninvasively with transcranial duplex sonography. A typical finding of an intracranial stenosis on transcranial Doppler sonography is mean flow velocity flow acceleration >100 cm/s.2 However, within high-grade or tandem stenoses, as in our patient, reduced blood flow velocities can be found. These can then be graded according to the thrombolysis in myocardial ischemia flow grades.3
Patients with intracranial stents require close follow-up. If the anatomy of the temporal bone window allows sufficient transcranial insonation, noninvasive Doppler or duplex sonography should be considered as the primary technique to screen for ISR. However, in some cases, there will still be a need to confirm abnormal findings with additional imaging techniques. Whether traditional CT angiography, MR angiography, or flat-panel-detector angiographic CT4 is sufficient in this scenario is still under debate.

A, Transcranial duplex sonography of the right middle cerebral artery showing compromised flow velocities distal to stent in a depth of 48 mm. B, CT angiography demonstrates a reduced filling at the distal part of the stent. C, Finally, intra-arterial digital subtraction angiography reveals bilateral restenoses on both sides of the stent (black arrows).
References
- Copyright © American Society of Neuroradiology









{kind=link}