
Abstract
SUMMARY: Aplasia of the common crus is an uncommon congenital anomaly. We present the case of a patient with common crus aplasia and discuss the relevant embryology and the role of 3D CT in evaluation of this rare congenital anomaly.
Most of the patients who present with congenital sensorineural hearing loss (SNHL) do not demonstrate an imaging abnormality.1 Only 39% of patients with congenital SNHL have a documented imaging abnormality, with large vestibular aqueduct syndrome being the most common of the congenital anomalies to be identified on imaging.2 Congenital anomalies of the semicircular canals can result in SNHL. Dysplasia of the lateral semicircular canal has been reported to be the second most common cause after large vestibular aqueduct syndrome to be so associated.3 Common crus aplasia is an uncommon congenital anomaly.4,5 We report the case of a patient with common crus aplasia and review the underlying pathogenesis.
Case Report
A 25-year-old man, a Mexican immigrant, presented to our otolaryngology clinic with difficulty in hearing. The patient's previous medical records could not be traced. On questioning, the patient reported worsening hearing loss since birth. On examination, bilateral SNHL was noted. There were no other features to suggest an association with any syndrome. The patient was referred for a high-resolution CT scan of the temporal bone. Axial and coronal 2D CT scans demonstrated dilated dysplastic lateral semicircular canals with possible dysplastic vestibules bilaterally (Fig 1). Corresponding 3D axial and coronal CT scans confirmed the presence of dilated dysplastic lateral semicircular canals and dysplastic vestibules. However, the 3D CT images raised the possibility of bilateral absence of the common crus, which was not noticed during the initial interpretation on the conventional 2D CT scans (Fig 2). A 3D volume-rendered CT image confirmed bilateral common crus aplasia (Fig 3).
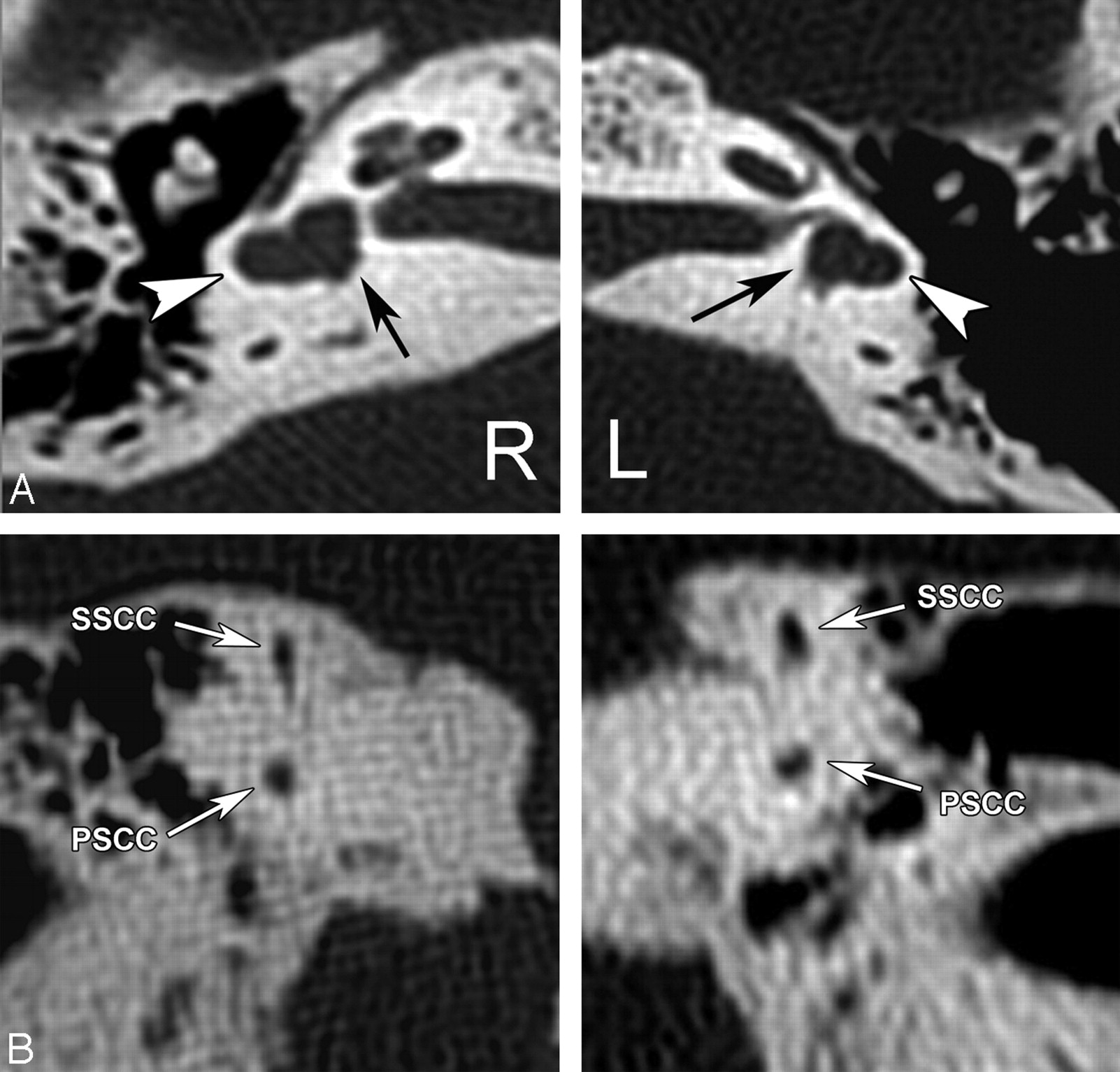
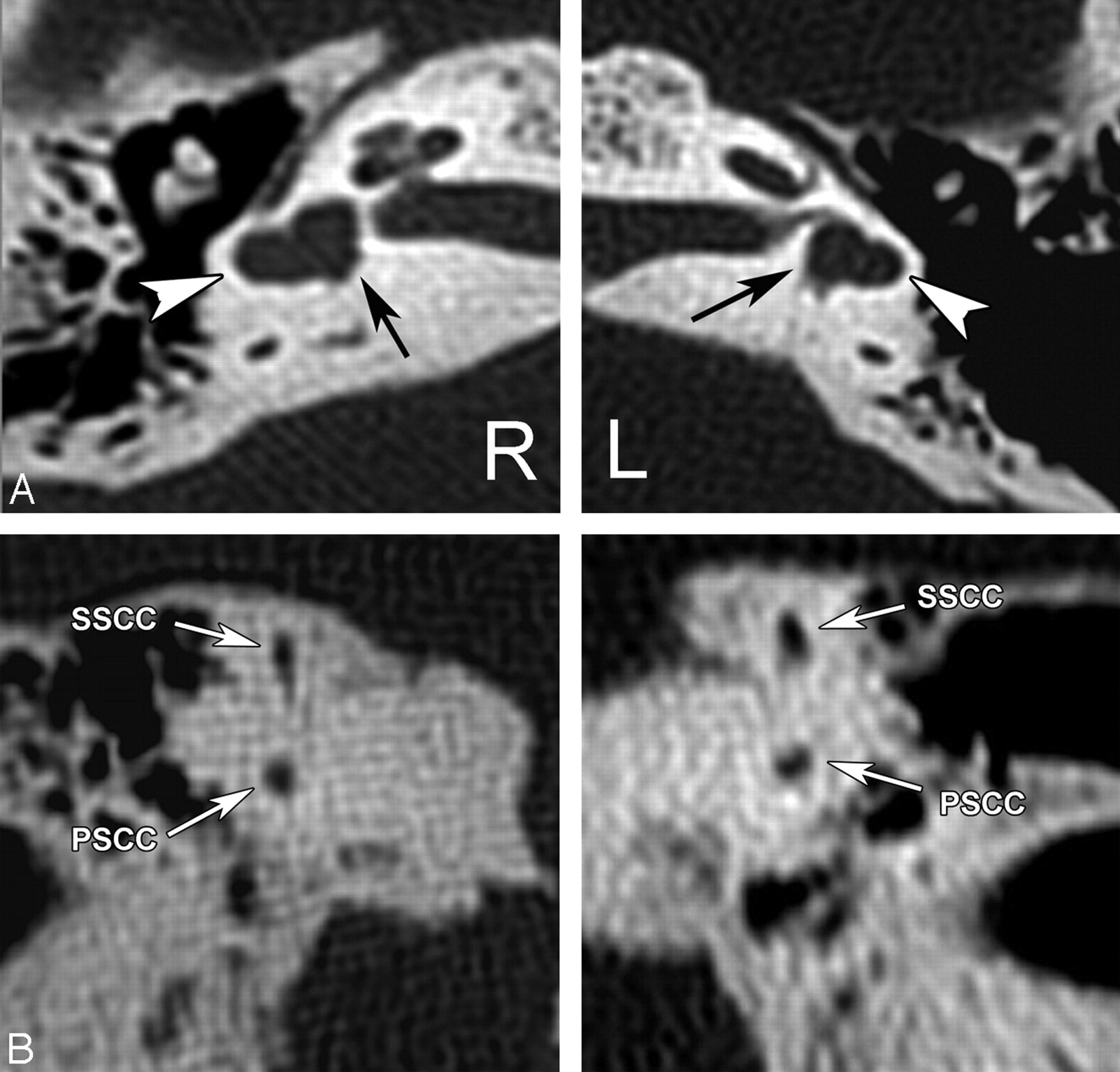
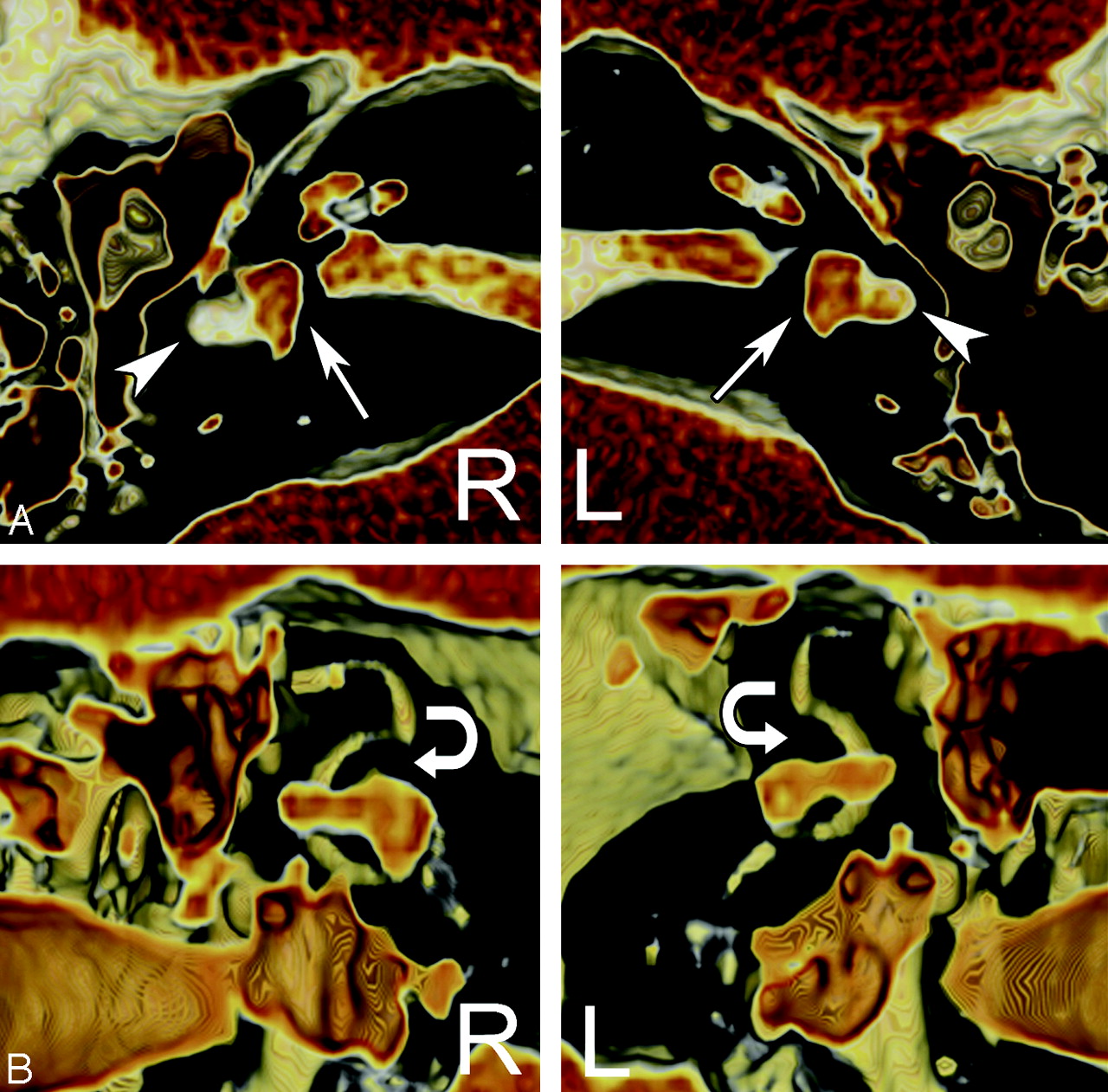
Axial (A) and coronal (B) 2D CT scans demonstrate dilated dysplastic lateral semicircular canals (arrowheads) with possible dysplastic vestibules (arrows) bilaterally. 2D coronal CT images demonstrate segments of the posterior and superior semicircular canals.
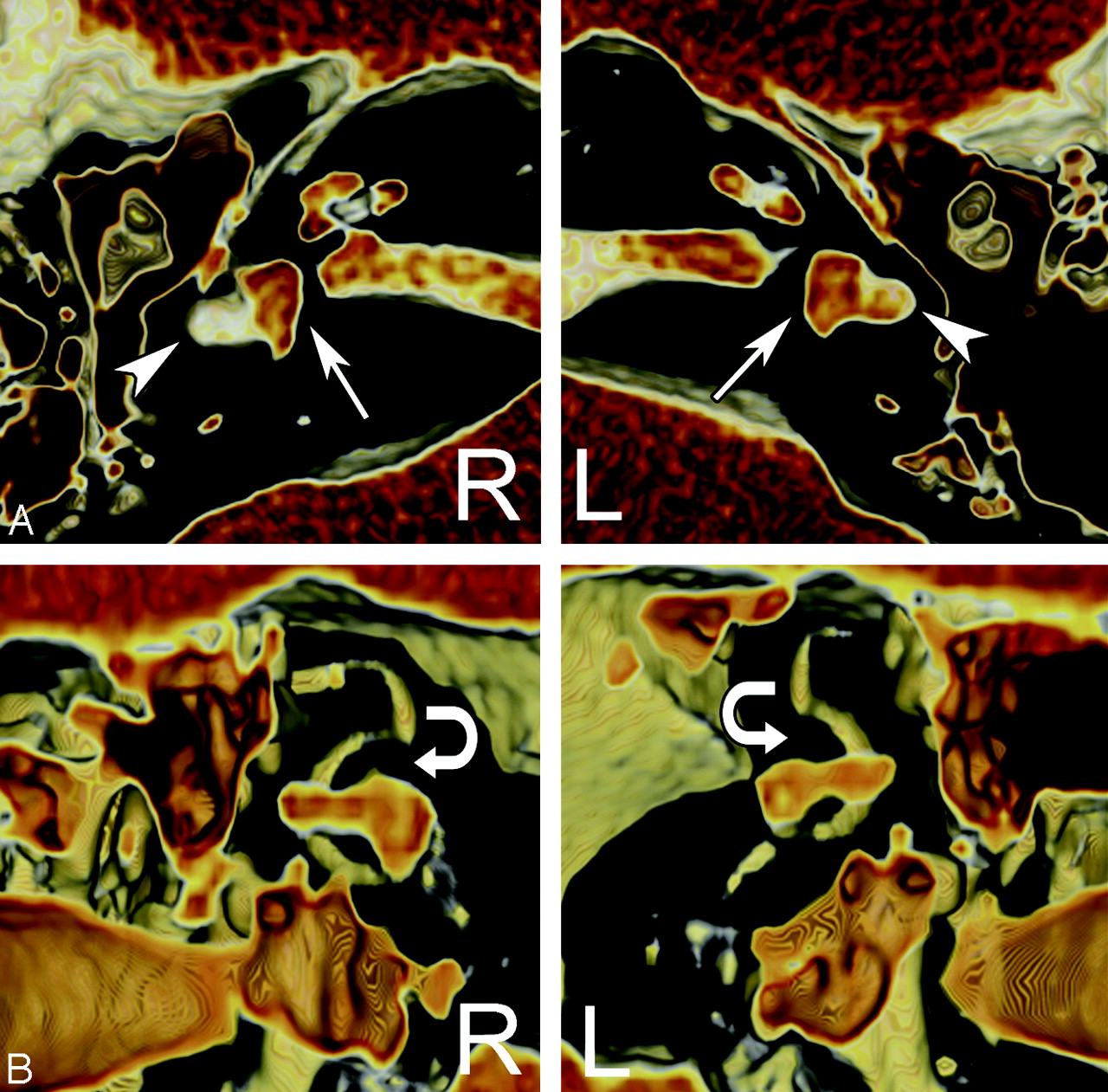
Corresponding axial (A) and coronal (B) 3D CT scans confirm the presence of dilated dysplastic lateral semicircular canals (arrowheads) and dysplastic vestibules (arrows). However, the 3D CT images raise the possibility of bilateral absence of the common crus, which was not noticed during the initial interpretation on the conventional 2D CT scans. The expected location of the common crus has been demonstrated by curved arrows.

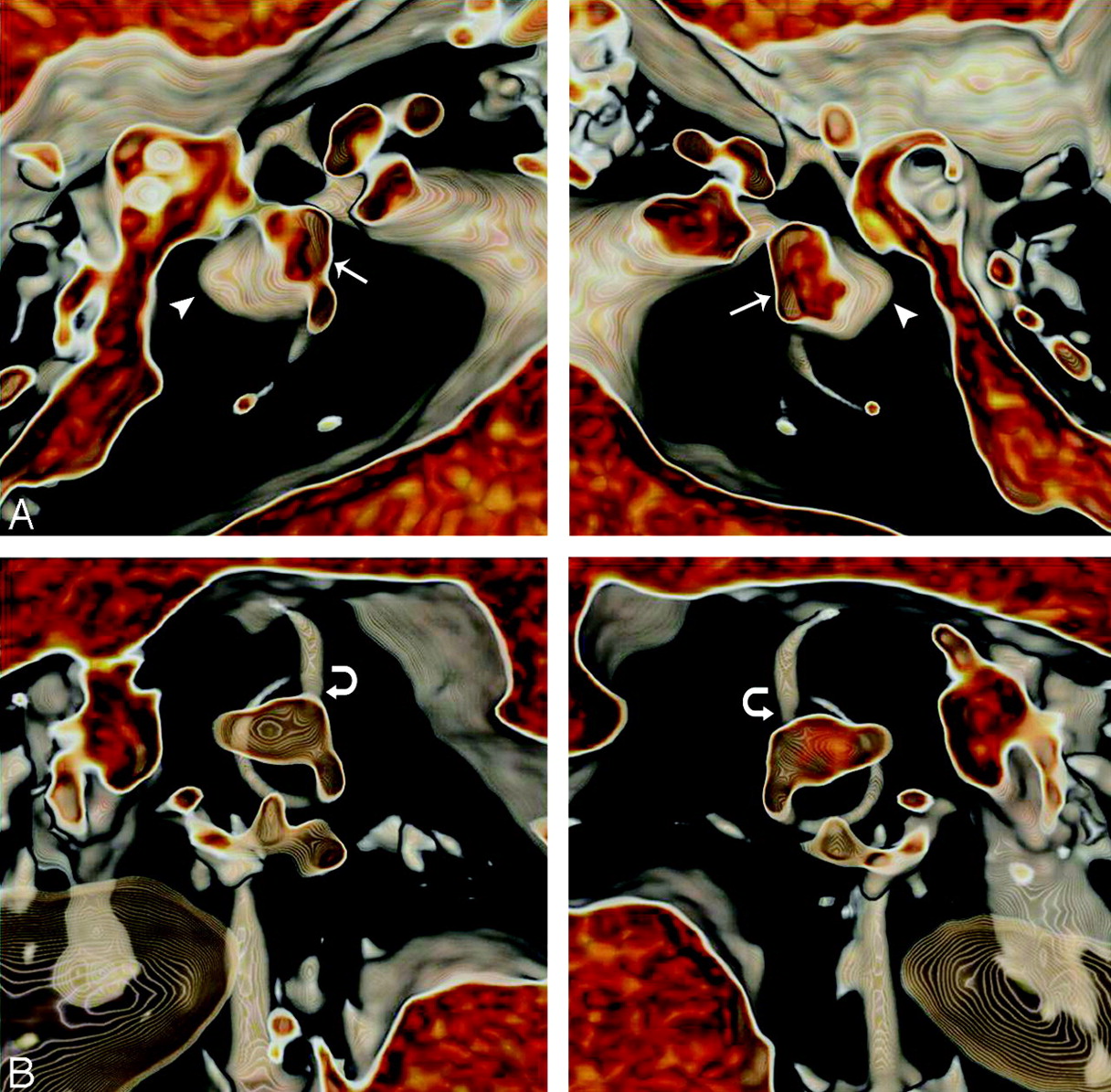
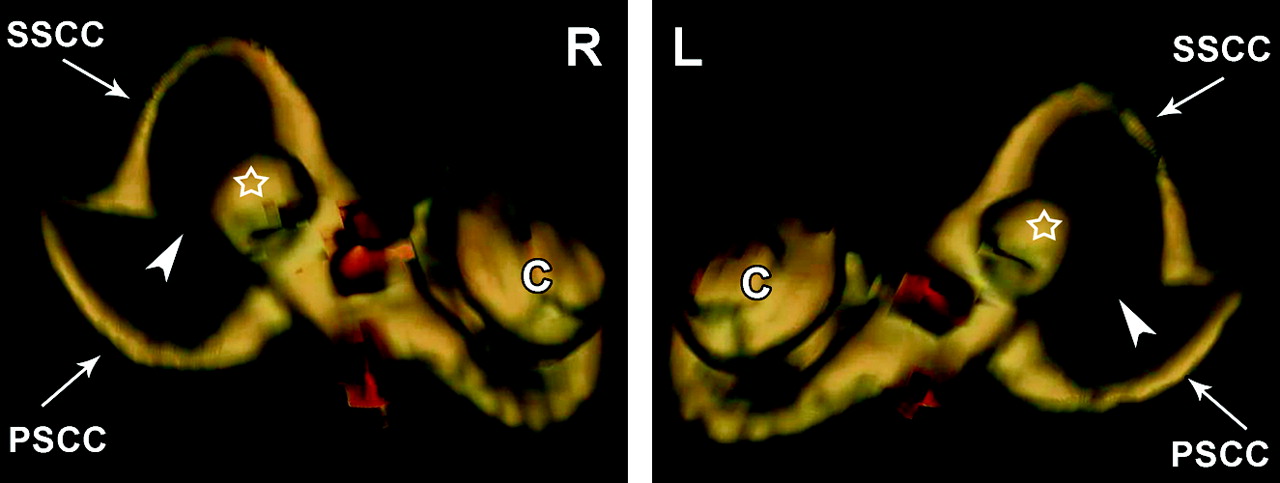
Volume-rendered 3D CT image confirms bilateral common crus aplasia (arrowheads) with dilated dysplastic lateral semicircular canals (open-star). SSCC indicates superior semicircular canal; PSCC, posterior semicircular canal.
Discussion
The 3 semicircular canals—superior, posterior, and lateral—lie in orthogonal planes with respect to each other. The posterior semicircular canal and superior semicircular canal share a common limb, the common crus, which is formed by the fusion of the posteromedial end of the superior semicircular canal and the anteromedial end of the posterior semicircular canal.4 From the point of joining, the common crus runs medially for a length of approximately 4 mm at an oblique angle of approximately 60° to the axial plane until it opens into the superomedial portion of the vestibule.
Dysplasia of the semicircular canals is a frequent congenital inner ear malformation, with abnormalities of the lateral semicircular canal being the most commonly identified anomaly noted on imaging.6 Absence of the common crus or common crus aplasia is uncommon. However, it is one of the known associations of Goldenhar syndrome.5
Common crus aplasia is usually associated with dysplasia of the lateral semicircular canal. This association can be understood if one is familiar with the embryology of the semicircular canals. The inner ear starts to develop between the fourth and eighth weeks of gestation, grows between the eighth and 16th weeks of gestation, and ossifies between the 16th and 24th weeks of gestation.7 At day 22 of development, surface ectoderm on each side of the rhombencephalon thickens to form the otic placodes, which invaginate and separate from the overlying ectoderm to become otocysts. The epithelial lining of the membranous labyrinth is derived from the otocyst, whereas the mesenchyme surrounding the outgrowing epithelial structures differentiates into cartilage and eventually ossifies to form the bony labyrinth of the inner ear.3 The semicircular canals begin as evaginations of the otocyst during the sixth week of development. The superior semicircular canal develops first, approximately from days 36 to 44, followed by the posterior semicircular canal (days 42–47). The lateral semicircular canal is formed last, starting approximately on day 44 and reaching maturity on day 49.8,9 Because the lateral semicircular canal is the last to be formed, it is most frequently subject to congenital malformation.6 Any malformation known to occur before this period, such as during the development of the posterior semicircular canal and superior semicircular canal, should therefore cause an associated abnormality in the lateral semicircular canal, as illustrated in our case. Benton et al10 propose that the formation of a single posterosuperior semicircular canal may be caused by abnormal resorption of the neuroectodermal tissue of the membranous common crus, related to inner ear damage from local hematoma or vascular abnormality. Reabsorption of the neuroectodermal tissue originating from the epithelial lining of the otocyst may result in insufficient stimulation for the surrounding mesenchyme to differentiate into cartilage and eventually bone, thus resulting in common crus aplasia. Although this theory sounds plausible, it does not explain the simultaneous occurrence of lateral semicircular canal dysplasia.
The spatial orientation of the common crus makes it difficult to evaluate for subtle morphologic anomalies of common crus on conventional axial and coronal 2D scans of the temporal bone. Volume-rendered CT images can be rotated in any plane, allowing for visualization of structures such as the common crus, otherwise not easily identified on conventional imaging (Figs 4–⇓6). According to our literature search, this is the first article that demonstrates the role of 3D CT in evaluation of common crus aplasia.

Axial (A) and coronal (B) 2D CT scans demonstrate dilated dysplastic lateral semicircular canals (arrowheads) with possible dysplastic vestibules (arrows) bilaterally. 2D coronal CT images demonstrate segments of the posterior and superior semicircular canals.
Corresponding axial (A) and coronal (B) 3D CT scans confirm the presence of dilated dysplastic lateral semicircular canals (arrowheads) and dysplastic vestibules (arrows). Coronal 3D CT images demonstrate presence of common crus bilaterally (curved arrows).

Volume-rendered 3D CT image confirms bilateral dilated dysplastic lateral semicircular canals (open-star) and vestibule. However, the common crus (arrowheads) are present. SSCC indicates superior semicircular canal; PSCC, posterior semicircular canal.
References
- Received August 25, 2008.
- Accepted after revision October 17, 2008.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.