
Abstract
Summary: Infarcts of the corpus callosum have not been well documented in the radiologic literature. We present five cases that were unusual in either their clinical or radiologic presentation or both. Biopsies were performed in three of the five cases, and in time, all lesions evolved in a pattern consistent with infarct. Recognition of the varied clinical and radiologic presentation of infarcts of the corpus callosum will obviate the need for biopsy in most patients.
Infarcts of the corpus callosum have not been well documented in the radiologic literature. They are not common (1–3), and according to Chrysikopoulos et al (4), this is most likely due to a rich blood supply from three main arterial systems, specifically the anterior cerebral, anterior communicating, and posterior cerebral arteries. Corpus callosum infarcts may present with slowly evolving and/or non-localizing neurologic signs and symptoms that suggest the diagnosis of tumor rather than infarct. In addition, they may exhibit radiologic features more often associated with neoplasm, such as masslike enhancement or extension across the midline, that prompt biopsy. We present five patients with corpus callosum infarcts, three of whom underwent biopsy because of their clinical or radiographic presentation or both. The use of appropriate imaging studies, including MR angiography and follow-up examinations, can eliminate the need for unnecessary biopsies.
Case Histories
Case 1
A 50-year-old woman with a past medical history significant for insulin-dependent diabetes mellitus and hypertension presented with two episodes of transient left-sided weakness. Non-contrast CT upon admission showed a 2-cm low-density lesion within the genu of the corpus callosum. Old infarcts in the right parietal and posterior frontal regions were also noted. Follow-up contrast-enhanced CT (Fig 1A) 2 days later again showed a non-enhancing lesion within the corpus callosum. There was mass effect on the frontal horns of the lateral ventricles. Contrast-enhanced T1-weighted MR imaging (Fig 1B) revealed an expansile, hypointense lesion within the body and genu of the corpus callosum that was hyperintense on the T2-weighted images (Fig 1C) and attributed to be the cause of the patient's symptoms. No abnormal enhancement was seen. Based on the clinical and radiologic findings, a low-grade glioma was considered, and a biopsy was performed 12 days after the initial CT examination. The results of the biopsy confirmed an infarct.
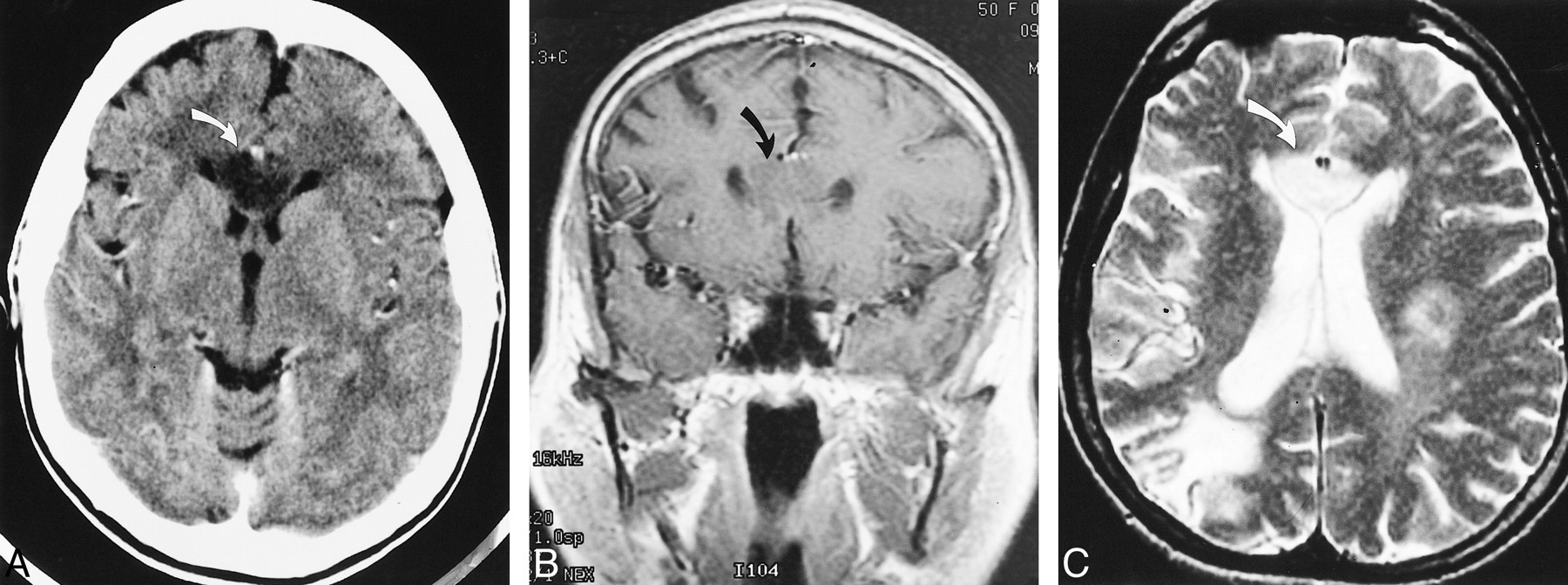
Case 1. Axial postcontrast CT image (A) and coronal postcontrast T1-weighted image (B) (480/20/1 [TR/TE/excitations]) show a non-enhancing lesion within both sides of the genu (curved arrow) of the corpus callosum with mass effect on the frontal horns. Axial T2-weighted image (C) (2500/105/1) shows corresponding high signal intensity within the genu of the corpus callosum (curved arrow), crossing the midline. An old infarct is noted within the right posterior border zone and scattered foci of T2 signal abnormality are seen in the left frontal and parietal regions. A biopsy of the lesion was obtained, confirming an infarct
Case 2
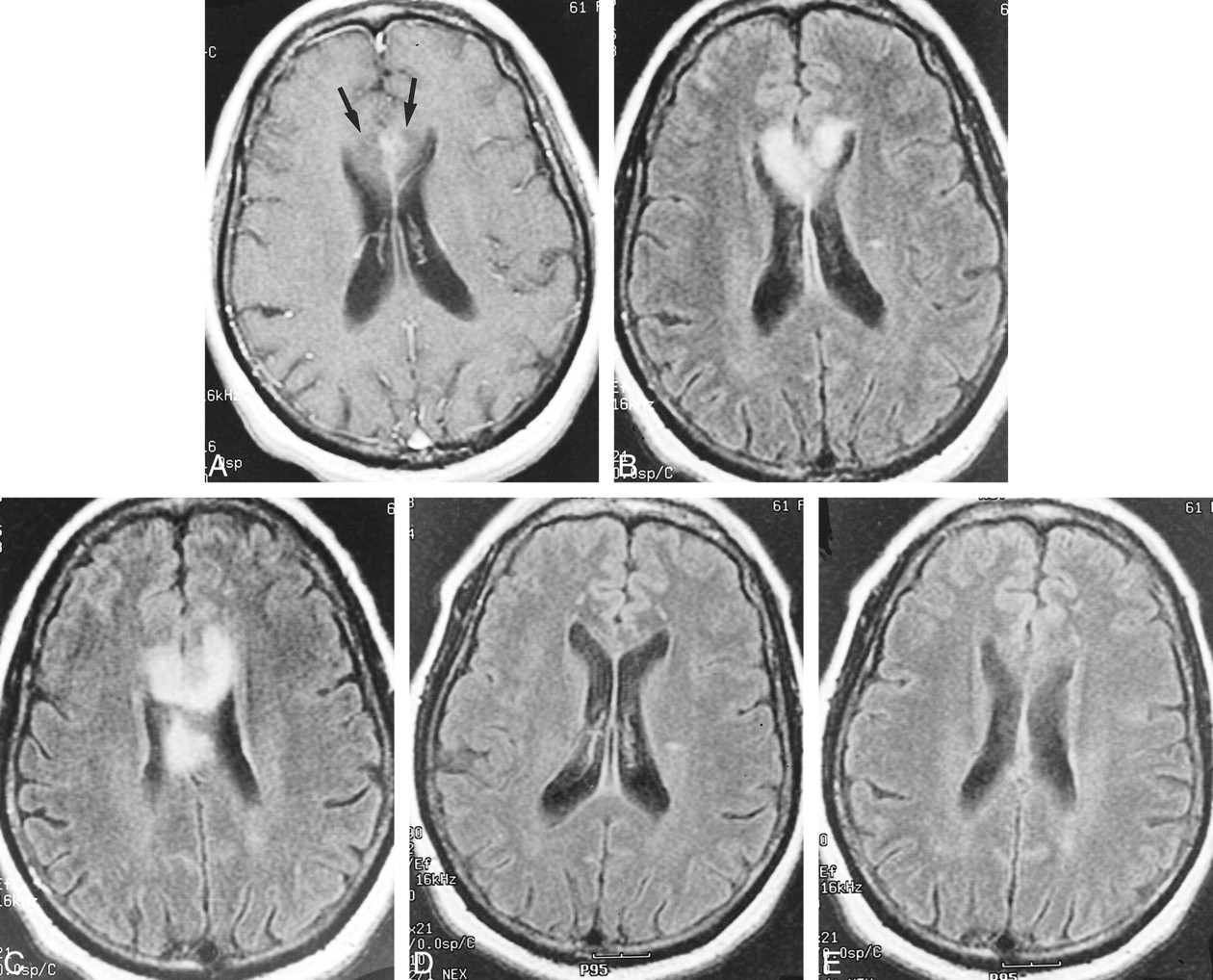
A 61-year-old woman with a long history of hypertension and insulin-dependent diabetes mellitus was in her usual state of health, when 2 to 3 weeks prior to admission, she developed slurred speech, difficulty with handwriting, and right-sided weakness. Her physical examination was significant for a 20% to 30% motor deficit of the right lower extremity. Initial non-contrast CT performed upon admission showed a low-density lesion extending across the genu of the corpus callosum, with mild mass effect on the frontal horns that, given the clinical findings, was considered the causative lesion. Contrast-enhanced MR imaging performed 2 days later showed subtle enhancement on the postcontrast T1-weighted images (Fig 2A) and abnormal high signal intensity on the fluid-attenuated inversion recovery (FLAIR) and long-TR images (Fig 2B and C) within the genu and body of the corpus callosum. The patient returned 3 weeks later for follow-up MR imaging. FLAIR images from that study (Fig 2D and E) showed almost complete resolution of the callosal signal abnormality. MR angiography was performed, which showed markedly small anterior cerebral arteries relative to the other cerebral vessels.

Case 2. Postcontrast axial T1-weighted image (A) (500/20/1) shows subtle enhancement with surrounding hypointensity within the genu of the corpus callosum (arrows). FLAIR images (B, C) (8900/140/1) show abnormal increased signal within both sides of the genu and body of the corpus callosum. Axial FLAIR images (D, E) (8900/140/1) from follow-up MR imaging performed 3 weeks later showed almost complete resolution of the abnormal signal within the corpus callosum
Case 3
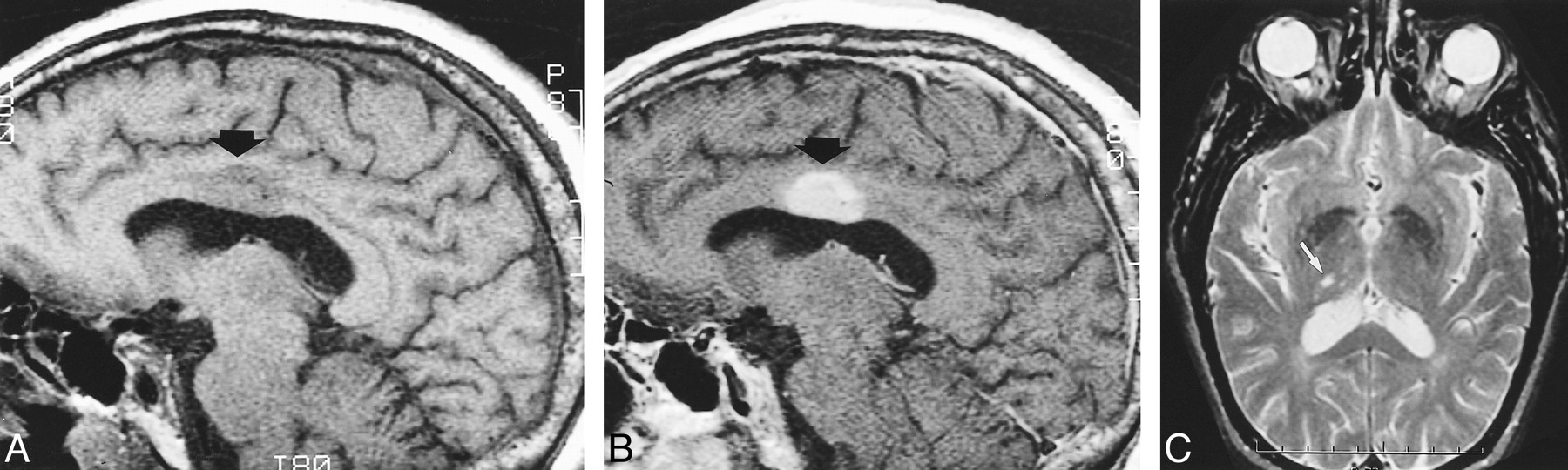
A 67-year-old man, with past medical history significant for hypertension, developed sudden-onset vertigo and left-leg paresthesia. His vertigo resolved, but his left-sided weakness persisted. An initial non-contrast CT performed upon admission showed a subtle region of low attenuation in the body of the corpus callosum on the right side. Long-TR MR imaging, performed 10 days after initial CT, depicted an ovoid hyperintense lesion within the body of the right corpus callosum that was hypointense on the T1-weighted images and enhanced homogeneously (Fig 3A and B). There was mild mass effect on the roof of the lateral ventricle. The patient's symptoms were attributed to a small infarct within the right thalamus (Fig 3C). The corpus callosum lesion was considered to be an asymptomatic tumor and a biopsy was performed 2 weeks after admission. The results of the biopsy confirmed an infarct.
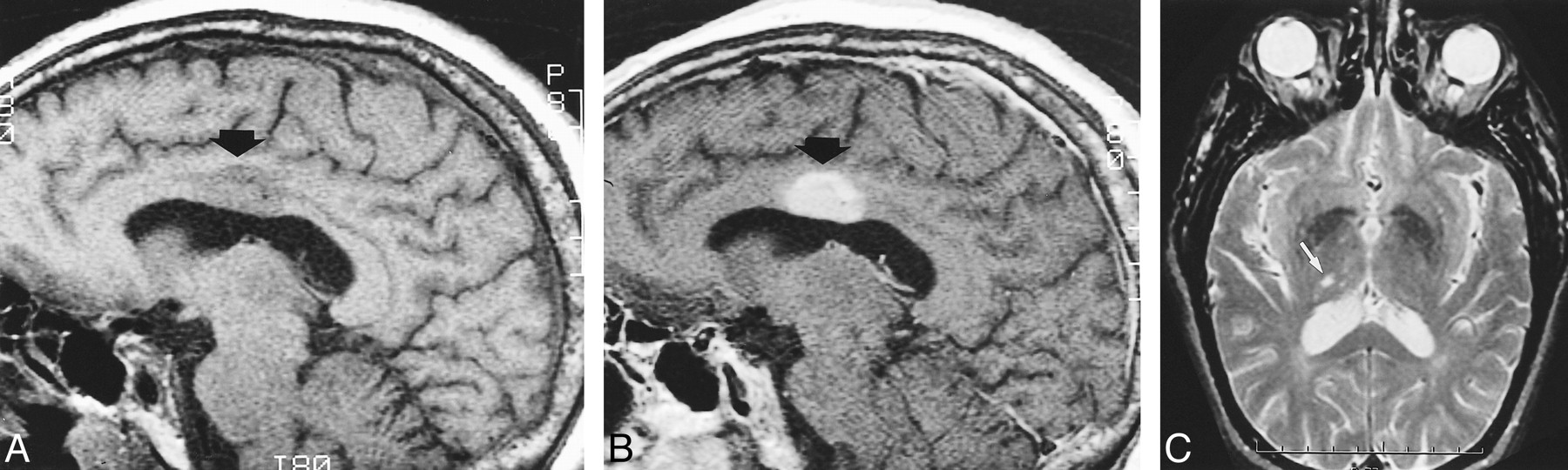
Case 3. Sagittal precontrast T1-weighted image (A) (400/12/2) shows a hypointense ovoid mass (arrow) within the body of the corpus callosum, depressing the roof of the lateral ventricle. After administration of contrast material (B) (400/12/2), it enhances homogeneously. A small infarct (white arrow) is noted within the right thalamus on the axial T2-weighted image (C) (2560/90/1). Subsequent biopsy confirmed an infarct
Case 4
A 79-year-old woman, with past medical history significant for hypertension, presented with a 3-week history of intermittent right-leg numbness and weakness. CT and MR imaging (Figures 4A and 4B) performed 4 days after admission showed low attenuation and abnormal signal intensity, respectively, within the left side of the corpus callosum and adjacent white matter, with mass effect on the left frontal horn. No other abnormality was noted. The diagnosis of tumor was considered, given the history of intermittent symptoms that continued during the next 4 weeks. Ill-defined enhancement was noted on a follow-up contrast-enhanced MR examination (Fig 4C and D), obtained 5 weeks post admission, further supporting the consideration of a neoplasm. A subsequent MR examination revealed resolution of the enhancement.
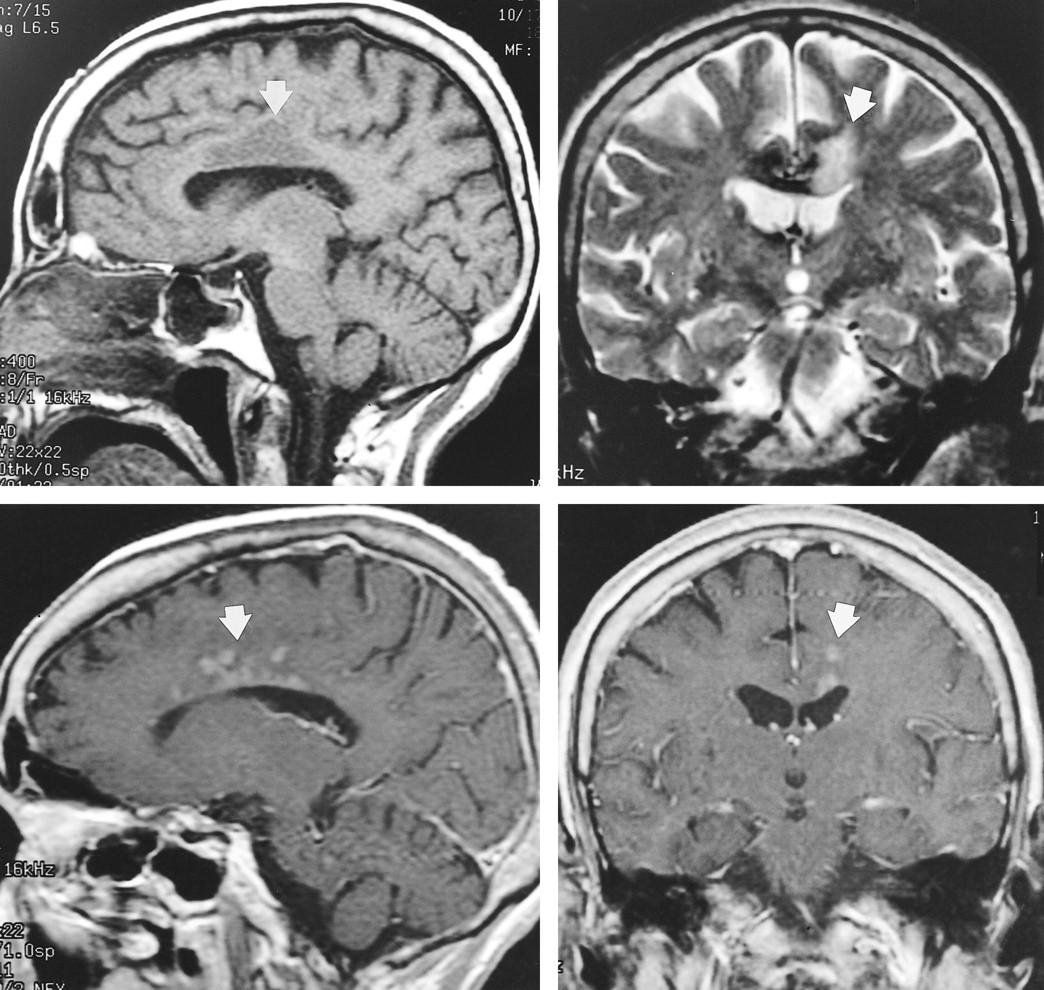
Case 4. Sagittal non-contrast T1- (A) (400/10/1) and coronal T2-weighted (B) (2500/105/1) images show abnormal signal within the body of the corpus callosum and adjacent white matter (arrow) on the left side. Sagittal (C) (400/8/2) and coronal (D) (450/20/1) postcontrast T1-weighted images from a subsequent MR examination show abnormal enhancement (arrow) within the corpus callosum and adjacent white matter
Case 5
A 47-year-old woman, with a past medical history of insulin-dependent diabetes mellitus and hypertension, presented with a 2-week history of episodic ataxia, confusion, mental slowness, and right-sided weakness. CT and MR examinations performed upon admission showed a non-enhancing expansile lesion in the left body and genu of the corpus callosum and adjacent frontal lobe, suggestive of tumor. The patient's symptoms were attributed to the lesion, and a stereotactic biopsy was performed 3 days after admission. Histologic examination confirmed an infarct.
Discussion
Infarcts of the corpus callosum are not common and are attributed to a rich blood supply from three main arterial systems: the anterior communicating artery, the pericallosal artery, and the posterior pericallosal artery (4). A detailed description of the vascular supply to the corpus callosum was published by Ture et al (5), including variations in the main arterial supply. The pericallosal branch of the anterior cerebral artery is most often the main vascular supply to the body. The subcallosal and medial callosal arteries, branches of the anterior communicating artery, provide the main supply for the anterior portion of the corpus callosum. The posterior pericallosal artery, a branch of the posterior cerebral artery, supplies the splenium.
Chrysikopoulos et al (4) offer other possible explanations for the immunity of the corpus callosum to infarction. Isolated infarcts of the anterior and posterior cerebral arteries are uncommon, accounting for 12% of all infarcts, and when present are found in conjunction with generalized atherosclerotic disease. All of the patients in our series had long histories of hypertension and three of the five patients had insulin-dependent diabetes mellitus, predisposing them to generalized atherosclerosis. Chrysikopoulos et al (4) note that the majority of strokes are thromboembolic in origin, and emboli tend to favor the middle cerebral artery distribution because of hemodynamic factors. Moreover, the penetrating vessels of the corpus callosum are small in size and generally run perpendicular to the parent artery, thus protecting the corpus callosum from emboli.
Kazui et al (6) found in their series that infarction localized to the anterior cerebral distribution was attributable most commonly to local atherothrombosis and occasionally to cardiogenic embolism. They also postulate that a hypoplastic A1 segment may facilitate the occurrence of embolism in the anterior cerebral artery distribution. MR angiography performed in one of the patients in our series (case 2) showed small anterior cerebral arteries relative to the other cerebral vessels. This was of uncertain etiology. Although stenosis was considered, no conventional angiogram was obtained.
Chrysikopoulos et al (4) found that the splenium of the corpus callosum was affected more often than was the body and genu. They attributed this to the greater incidence of posterior cerebral artery infarcts compared with anterior cerebral artery infarcts. In our series, all of the lesions involved the genu, body, or both, whereas none involved the splenium. The difference in the location of the infarcts in our study, as compared with that reported by Chrysikopoulos et al, may be due to the difference in the patient population; ie, patients with diabetes and hypertension develop generalized atherosclerosis, which in turn increases the incidence of anterior circulation infarction. Isolated anterior cerebral artery infarcts are rare, accounting for 0.6% of all cerebral infarcts (6). Chrysikopoulos et al (4) found evidence of hemorrhage in about 25% of their cases, whereas there was no evidence of hemorrhage in any of our cases. Thus, the presence of hemorrhage may suggest infarct, but the absence of hemorrhage should not exclude the diagnosis. Infarcts of the corpus callosum may exhibit a variable degree of mass effect. Mass effect is commonly seen in stroke, but when it occurs in a region such as the corpus callosum where stroke is often not considered, it suggests other entities that would require biopsy. Enhancement is often seen by the end of the 1st week and can persist for many weeks (7, 8). In many of our cases, the abnormal signal intensity or enhancement or both crossed the midline, unusual for infarct but not for tumor.
Clinically, infarcts of the corpus callosum are frequently associated with neuropsychiatric symptoms, mainly interhemispheric disconnection syndromes (9). In addition, specific syndromes such as dyspraxia contralateral to a paretic limb (10, 11) and alien hand syndrome (12, 13) have been reported, and an isolated gait disorder has been described in relation to lacunes in the anterior portion of the corpus callosum (12).
Conclusion
Infarcts of the corpus callosum are uncommon and have not been well documented in the radiologic literature. They may present atypically with slowly evolving and non-localizing signs and symptoms that are more suggestive of tumor. They may exhibit tumorlike enhancement and extend across the midline. Unnecessary biopsy can be avoided by understanding the varied clinical and radiologic features of infarcts of the corpus callosum and by using appropriate imaging studies, including diffusion-weighted imaging, perfusion imaging, and spectroscopy, if available, or MR angiography and follow-up examination. Diffusion-weighted imaging, perfusion imaging, and spectroscopy were not available at our institutions when these patients underwent imaging studies.
References
- Received November 23, 1999.
- Accepted after revision May 8, 2000.
- Copyright © American Society of Neuroradiology








{kind=link}
{kind=link}
{kind=link}
{kind=link}