
Abstract
BACKGROUND AND PURPOSE: The laterocavernous sinus (LCS) has recently been recognized as one of the major drainage pathways of the superficial middle cerebral vein (SMCV). Our purpose was to investigate the drainage pattern of the SMCV, with special emphasis on the angiographic anatomy of the LCS.
METHODS: The drainage pathways of the SMCV were evaluated prospectively on 100 selective carotid angiograms obtained in 65 consecutive patients.
RESULTS: The SMCV was absent in 19% of cases. A classic termination into the cavernous sinus (CS) was found in 20%, a paracavernous sinus in 39%, and an LCS in 22%. The LCS drained toward the pterygoid plexus (27%), the superior petrosal sinus (18%), the posterior aspect of the CS (32%), or a combination of these pathways (23%). A complete absence of connection between the LCS and CS was observed in 63.5% of the patients.
CONCLUSION: The LCS is a laterosellar venous space that is anatomically and angiographically distinct from the CS. Secondary small anastomoses between the LCS and CS may make it difficult to differentiate the two structures. Appreciation of the course and connection pattern of the LCS is important, particularly when planning an endovascular approach to treatment of lesions in the region of the CS.
The laterocavernous sinus (LCS) is a venous structure located in between the two dural layers forming the lateral wall of the cavernous sinus (CS). Although the presence of venous spaces within the lateral wall of the CS has only occasionally been mentioned in the anatomic, radiologic, and surgical literature (1–3), San Millán Ruíz et al (4) have recently shown that the LCS is one of the principal drainage pathways of the superficial middle cerebral vein (SMCV). According to these authors, the outflow of the SMCV toward the middle cranial fossa follows three basic patterns: 1) it courses medially under the lesser sphenoid wing and terminates into the anterosuperior aspect of the CS (the classic or textbook termination of the SMCV), seen in 19.5% of patients in their study; 2) it runs medially toward the CS but continues its course posteriorly as an LCS enclosed within the lateral wall of the CS, seen in 34% of their patients; or 3) it follows a more lateral trajectory within the dural floor of the middle cranial fossa, where it takes the name of paracavernous sinus, seen in 46.5% of their patients (Fig 1).

Schematic representation of the three basic drainage pathways of the SMCV according to San Millán Ruíz et al (4). Superior view of the anterior, middle, and posterior cranial fossa (ACF, MCF, and PCF, respectively). The SMCV may continue as a paracavernous sinus coursing laterally over the MCF (a), as an LCS enclosed within the lateral wall of the CS (b), or may terminate into the anterosuperior aspect of the CS (c). Venous outflow toward the pterygoid plexus via a skull base foramen is shown for the LCS. 1, superior ophthalmic vein; 2, CS; 3, inferior petrosal sinus; 4, sigmoid sinus; 5, transverse sinus; 6, SMCV
Despite the close topographic relationship between the LCS and the CS, the two structures are separate anatomic entities with distinct functional and clinical implications (4). We present our findings concerning the drainage pattern of the SMCV as seen on 100 selective carotid angiograms, focusing our attention on the anatomy of the LCS as it may appear at digital subtraction angiography (DSA).
Methods
The drainage pattern of the SMCV was prospectively evaluated on 65 consecutive diagnostic cerebral angiograms obtained between May and June 1999 at the Johns Hopkins Hospital. Bilateral selective carotid studies were obtained in 55 patients and unilateral studies in 10 patients, resulting in 120 venous phases (hereafter referred to as cases) available for review. The indications for cerebral angiography among the patient population are detailed in Table 1. Patients ranged in age from 13 to 86 years, with a mean age of 49 years. Imaging was performed using a standard femoral approach and biplane angiographic equipment at a frame rate of one image per second. When an SMCV was present, its drainage pattern was evaluated in at least two different projections: generally, anteroposterior (AP) and lateral views. In addition, the topographic relationship between the SMCV, the CS, and the internal carotid artery (ICA) was systematically assessed with the sequential subtraction technique (5). By using venous images as masks for the subtraction process, this technique allowed simultaneous display and analysis of the arterial and venous phases of an angiographic study.
Indication for cerebral angiography in the studied patient population
Results
The quality of venous imaging was found insufficient for precise anatomic analysis in 20 of the 120 cases studied, either because of the presence of uncorrectable motion artifacts (18 cases) or of large cavernous ICA aneurysms, which obliterated the laterosellar venous spaces (two cases). The drainage pattern of the SMCV could thus be evaluated in the venous phases of 100 selective carotid studies. The SMCV was absent in 19 cases (19%). A classic termination of the SMCV into the anterosuperior aspect of the CS was observed in 20 cases (20%). A paracavernous sinus was found in 39 cases (39%), draining mainly into the pterygoid plexus (44%) or the superior petrosal sinus (SPS) (33%). An LCS was present in 22 cases (22%), draining mainly into the pterygoid plexus (27%) or the SPS (18%). A paracavernous sinus draining into the CS after a short course in the middle temporal fossa was observed twice (5%), whereas termination of an LCS into the posterior aspect of the CS occurred in seven cases (32%). A combination of two or three of these drainage routes was observed in 18% of paracavernous sinuses and in 23% of LCSs. Anastomotic channels of small caliber linking the CS with either an LCS or a paracavernous sinus were observed in 36% and 8% of cases, respectively. Slightly delayed filling of the CS with no evident connections was also observed. In such instances, the presence of small, angiographically undetectable anastomotic channels could not be excluded. An LCS was observed in the absence of the ipsilateral SMCV in two cases, in which the LCS was the continuation of a vein draining the medial aspect of the temporal lobe, corresponding to an uncal vein. The drainage patterns of the LCS and the paracavernous sinus are summarized in Table 2.
Drainage patterns of the paracavernous and laterocavernous sinuses
Discussion
The Angiographic Anatomy of the LCS
Because it constitutes, in most cases, the drainage route of an SMCV, the LCS is usually carrying venous blood coming from the ipsilateral cerebral convexity. If present, an LCS is thus best appreciated on the venous phase of an anterior circulation angiogram; that is, a selective injection of the common carotid artery or the ICA. On lateral views, the LCS appears as a bandlike opacity generally following an anterior-to-posterior and superior-to-inferior course projected over the sellar region, the cavernous portion of the ICA, and the CS itself (Fig 2A). For this reason, the LCS is difficult to set apart from the CS on a lateral view alone, and analysis of the AP view is generally needed to distinguish the LCS from the medial and lateral compartments of the CS. When there is no connection between the LCS and the CS, the AP view will show a well-delineated LCS but no opacification of the ipsilateral CS (Fig 2B and C). On the other hand, when connections linking the LCS to the CS allow for their simultaneous opacification, identification of the different laterosellar venous spaces has to rely on their respective topographic relationships with the ICA (Figs 3 and 4B). On the AP view, the medial and lateral compartments of the CS lie, respectively, medial and lateral to the cavernous segment of the ICA, abutting the ICA wall. The LCS is the outermost venous structure of the laterosellar region, separated from the lateral compartment of the CS by the inner dural layer of the lateral wall of the CS (Fig 3). This inner layer may be seen as a thin vertical opacification defect between the LCS and the lateral compartment of the CS when these venous spaces are visible together (Fig 4). The slitlike appearance sometimes adopted by the LCS (Fig 5) may, however, make its detection more difficult when the CS is opacified simultaneously (Fig 4A). By allowing the superimposition of arterial landmarks on venous structures, the sequential subtraction technique greatly helps to accurately identify the laterosellar venous spaces (Fig 4). In particular, when only the LCS is opacified, the sequential subtraction technique will show that,unlike the lateral compartment of the CS, the LCS does not abut the wall of the cavernous ICA(Fig 5A).

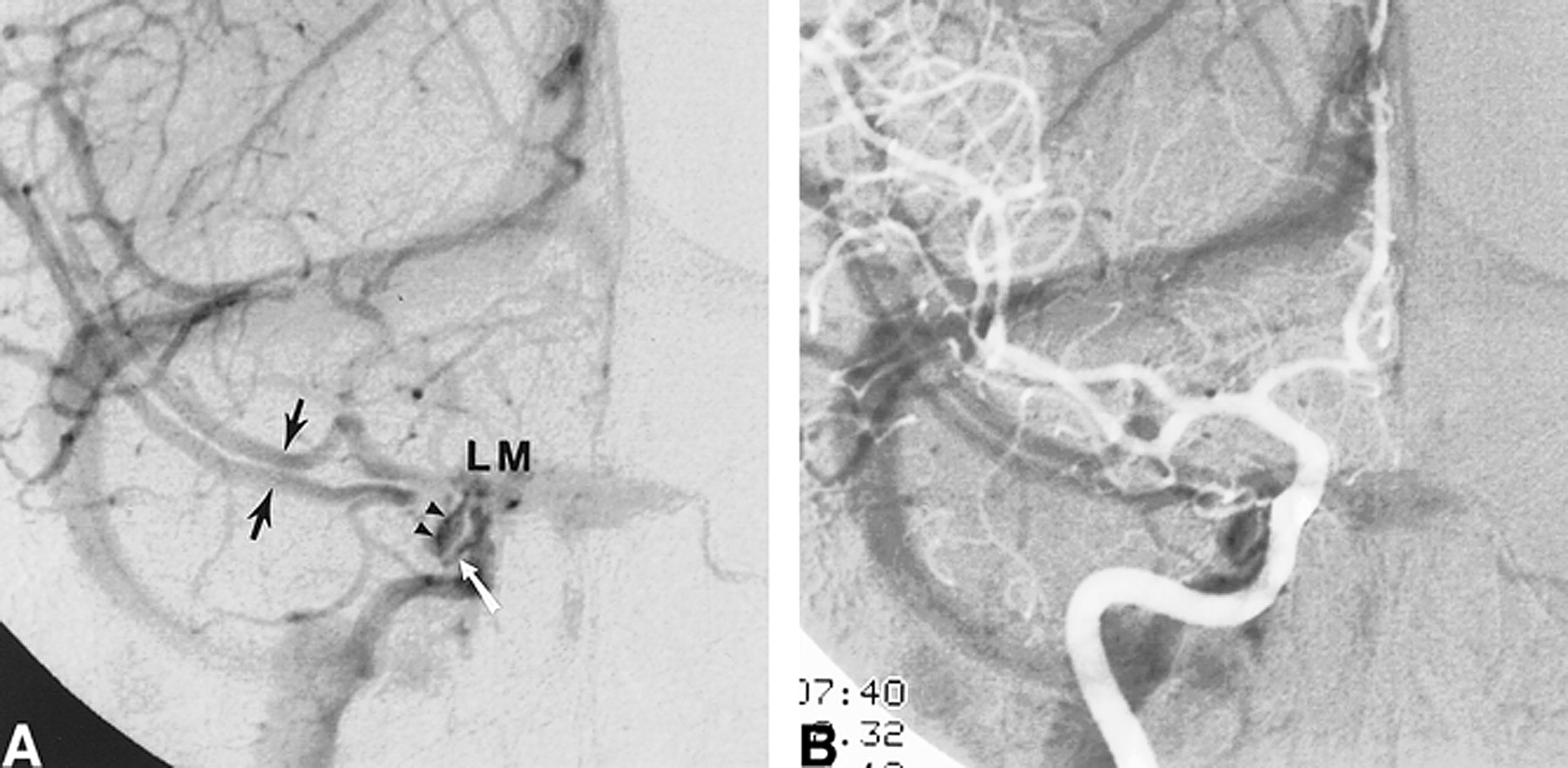
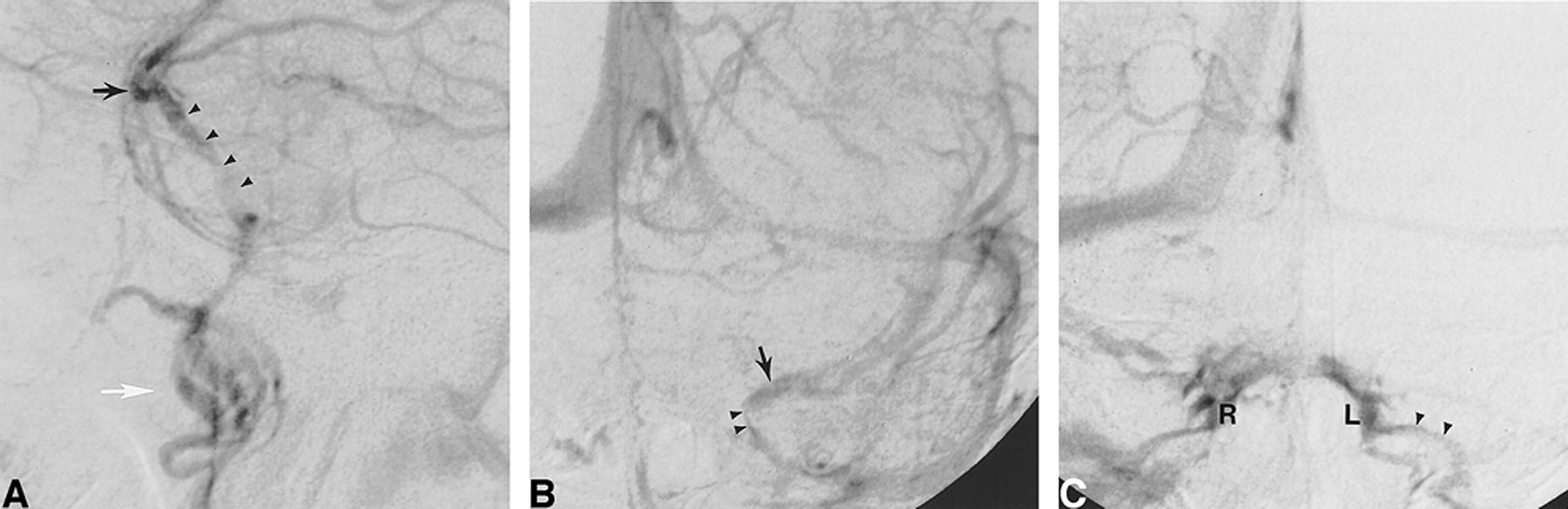
DSA, venous phase, in a 59-year-old man examined for carotid bifurcation atheromatous disease. Intracranial vasculature is normal.
A, Left ICA injection, lateral view. The left SMCV (black arrow) continues as an LCS (arrowheads), coursing posteriorly and inferiorly and projecting over the sellar region. In this case, note that the LCS drains toward the pterygoid plexus (white arrow) through foramina in the middle cranial fossa floor.
B, Left ICA injection, AP view. The left SMCV (arrow) is opacified, as is a left LCS (arrowheads). There is no opacification of the left CS.
C, Right ICA injection, AP view. Venous blood coming from the right cerebral hemisphere opacifies both the right CS (R) and left CS (L) through intercavernous connections. Note also opacification of the left inferior petrosal sinus (arrowheads), which was not visible on the left ICA injection.

Schematic representation of the laterosellar venous spaces, coronal view. The medial and lateral compartments of the CS and the LCS are shown in different shades of gray, as indicated at the bottom of the figure. The medial and lateral compartments of the CS are plexiform groups of veins lying on the medial and lateral aspects of the ICA, respectively. The LCS is a venous structure showing the morphologic characteristics of a dural sinus, located in between the outer (A) and inner (B) layers of the lateral wall of the CS. ICA indicates cavernous segment of the ICA; MCF, middle cranial fossa; P, pituitary gland; SB, sphenoid bone and sinus
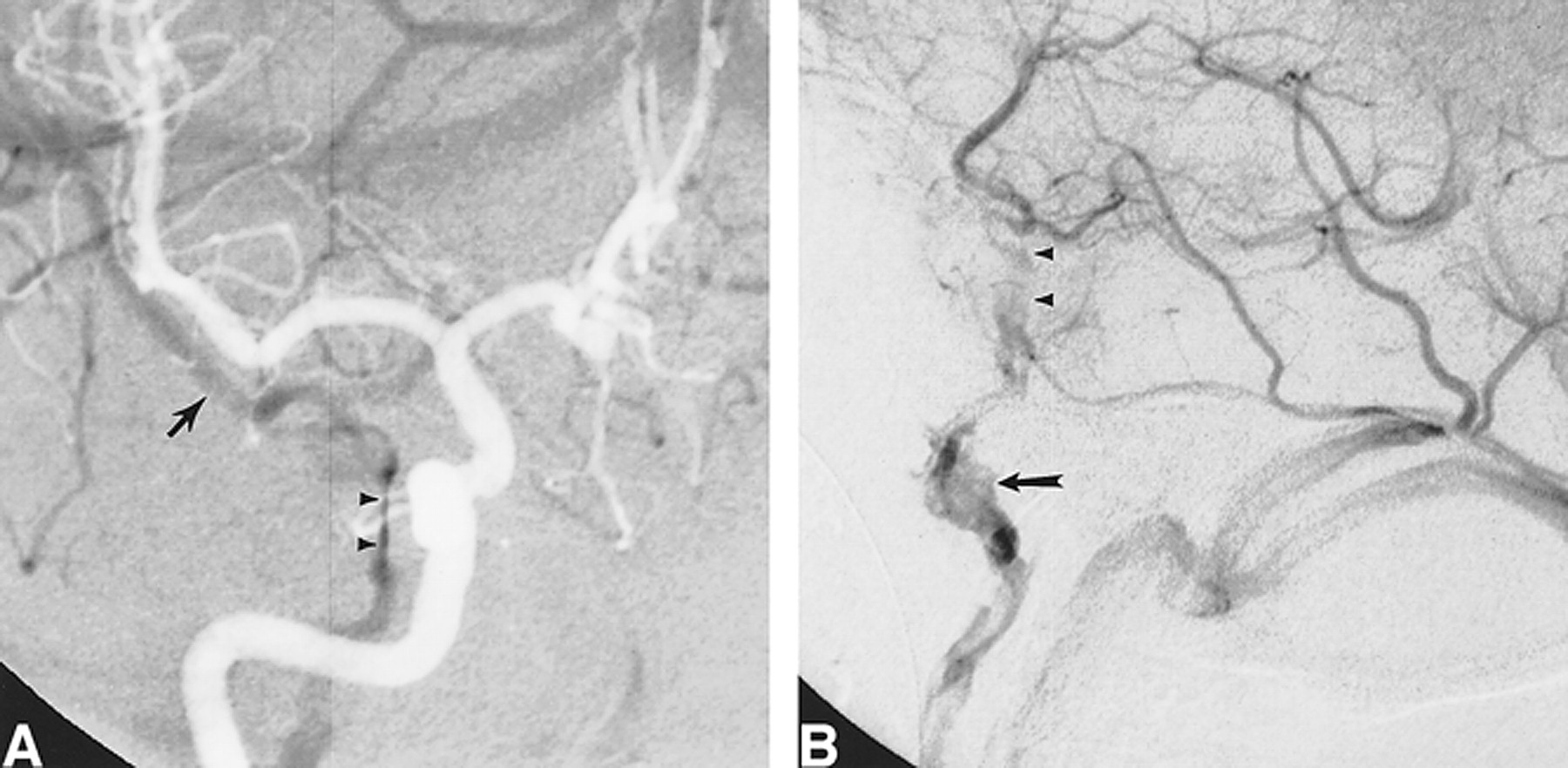
DSA, venous phase, in a 52-year-old woman examined for subarachnoid hemorrhage.
A, Right ICA injection, AP view. A duplicated SMCV (black arrows) runs medially toward the CS region to continue its course as an LCS (arrowheads), which terminates into the posterior aspect of the right CS via a small anastomotic channel (white arrow). The medial (M) and lateral (L) compartments of the CS and the right inferior petrosal sinus are well delineated. The left CS and inferior petrosal sinus are faintly opacified through intercavernous connections. The inner layer of the lateral wall of the CS is well appreciated as a curvilinear opacification defect located between the LCS and the lateral compartment of the CS.
B, Right ICA injection, AP view, sequential subtraction technique. Simultaneous visualization of the arterial (light) and venous (dark) phases confirms that the small anastomotic channel connects the LCS to the lateral compartment of the CS, the latter abutting the lateral aspect of the cavernous segment of the left ICA.
DSA, venous phase, in a 46-year-old man examined for subarachnoid hemorrhage. Cerebral angiogram showed an anterior communicating artery aneurysm.
A, Right internal carotid injection, AP view, sequential subtraction technique. The right SMCV (arrow) courses medially toward the CS region and continues posteriorly as an LCS (arrowheads). The LCS is lateral to the ICA, but not in its immediate proximity, and assumes a slitlike appearance. Since there is no connection between the LCS and the CS, the latter do not opacify and the LCS is consequently well appreciated. When connections allow for opacification of both the LCS and the CS, a slitlike LCS may be difficult to observe angiographically. Note the saccular aneurysm located at the right A1/A2 anterior communicating artery junction.
B, Right internal carotid injection, lateral view. Owing to its thin configuration, the slitlike LCS (arrowheads) faintly opacifies on a lateral view. Note the drainage pathway toward the pterygoid plexus (arrow).
Three basic drainage pathways have been described for the LCS (4): 1) toward the ipsilateral transverse sinus via the SPS (Fig 6); 2) toward the pterygoid plexus via openings in the floor of the middle cranial fossa (Fig 2A and B); and 3) toward the posterior aspect of the CS (Fig 4). Combinations of these patterns may also be observed. Interestingly, the drainage pathways toward the SPS and pterygoid plexus are similar to the outflow patterns described for the paracavernous sinus as sphenopetrous and sphenobasal sinuses, respectively (6). The predominance of the superior petrosal pathway over the pterygoid pathway found by San Millán Ruíz et al (4) in their anatomic study was not apparent in our angiographic observations, in which the outflow toward the pterygoid plexus appeared slightly dominant. This discrepancy may be related to the blood flow pattern in the SPS, which seems to be directed anteromedially toward the CS, at least from the point of termination of the petrosal vein (7). Even if anatomically present, the SPS may thus fail to opacify on anterior circulation studies, and would be clearly delineated only when it represents the major or unique drainage pathway of the SMCV. This hypothesis is compatible with our angiographic findings (Fig 6).
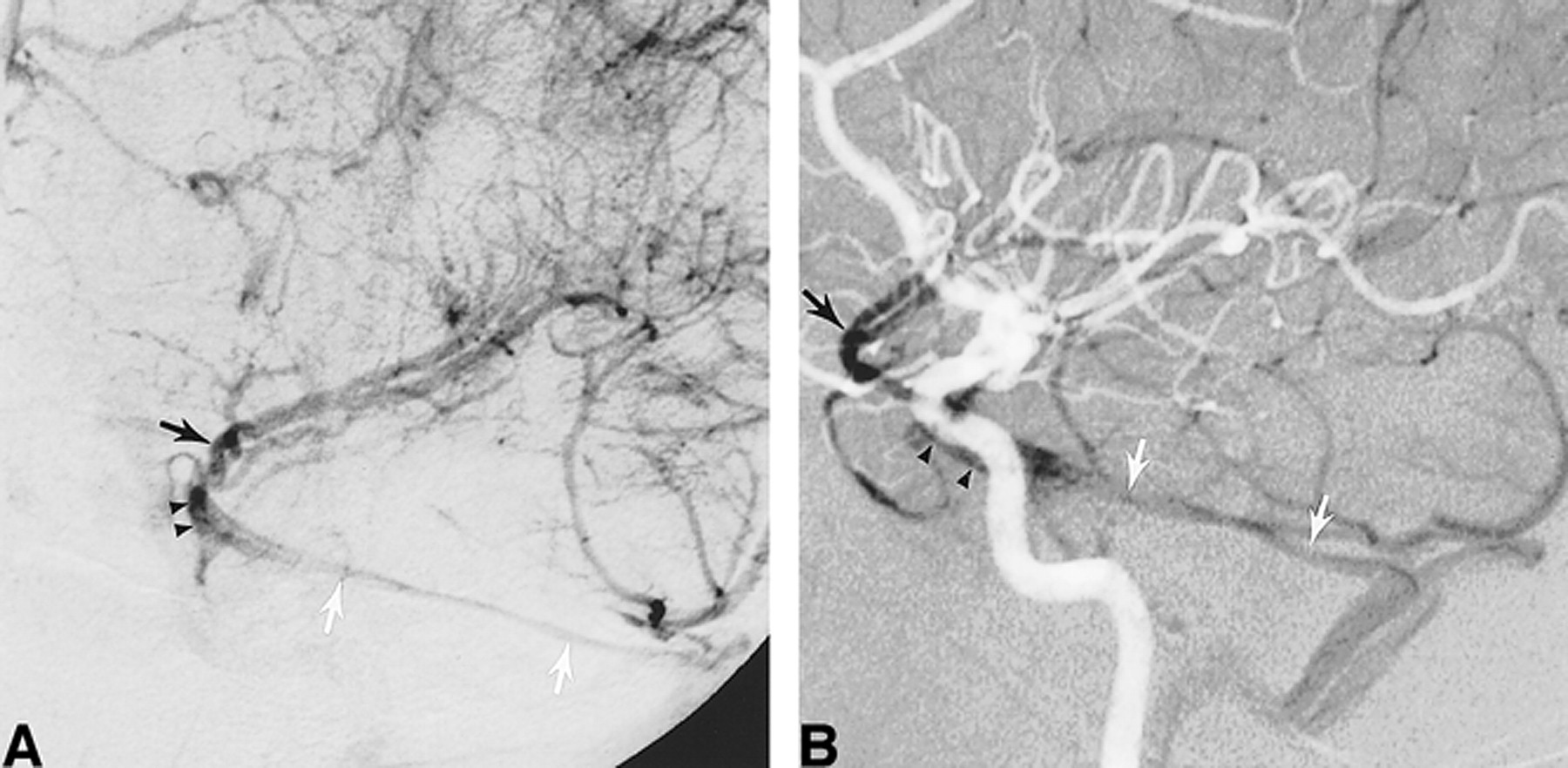
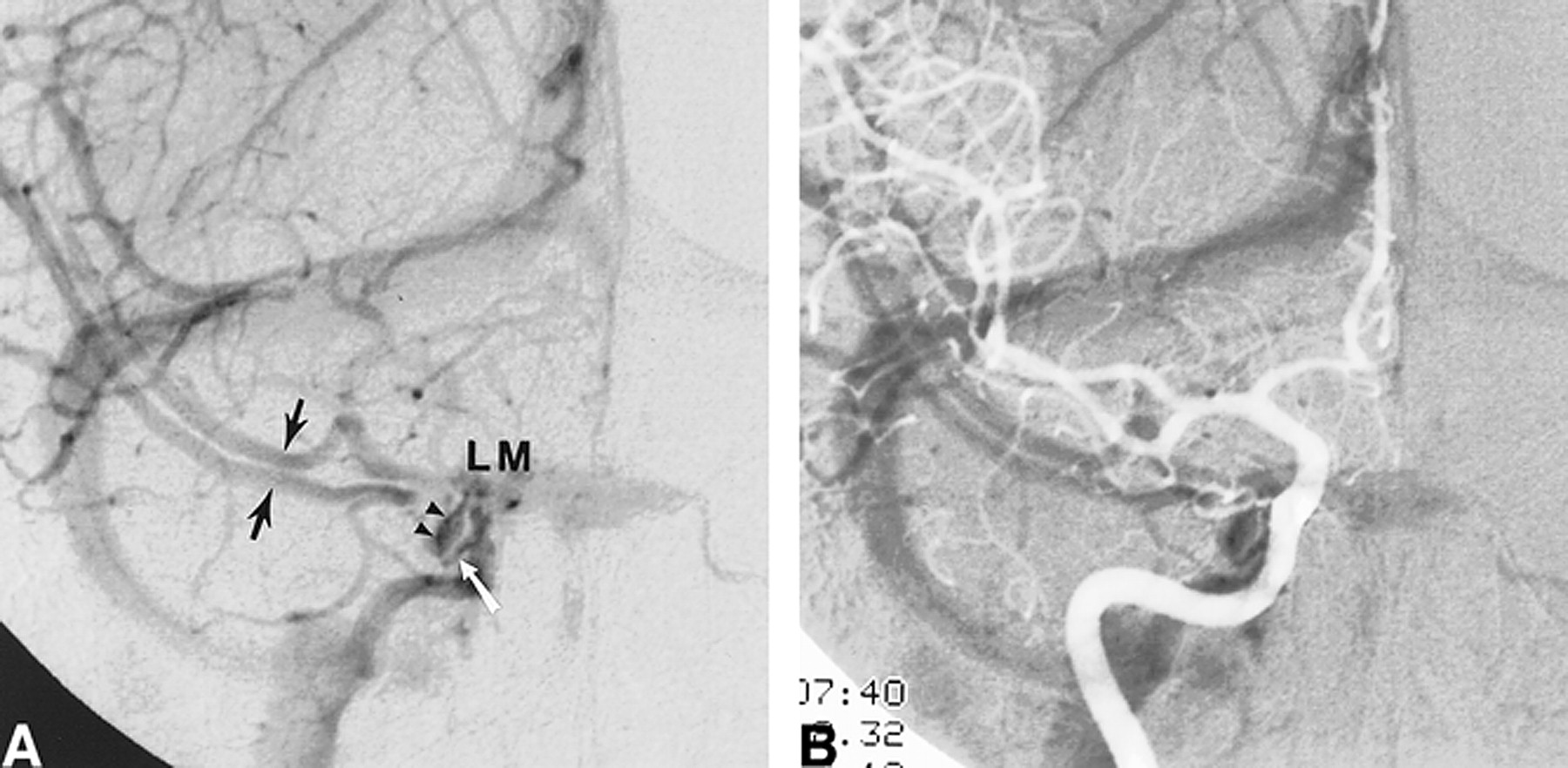
DSA, venous phase, in a 38-year-old man examined for subarachnoid hemorrhage.
A, Left ICA injection, left anterior oblique view. The left SMCV (black arrow) courses medially toward the CS region but continues posteriorly as an LCS (arrowheads) and then as an SPS (white arrows), ending in the left transverse sinus. There is no connection with the CS, which is not opacified.
B, Left ICA injection, lateral view, sequential subtraction technique. The arterial (light) and venous (dark) phases are displayed simultaneously, enabling visualization of their topographic relationship. The LCS (arrowheads) is seen overlying the cavernous segment of the left ICA. Posteriorly, it continues as the left SPS (white arrows) coursing over the petrous ridge before reaching the left transverse sinus. Black arrow indicates the left SMCV.
Connections between an LCS and the CS may take two different forms (4): the LCS may terminate into the posterior aspect of the CS (Fig 4), or the LCS may present one or several secondary anastomoses with the CS along its course, established either via small apertures in the inner layer of the CS lateral wall or via small anastomotic channels at the skull base (Fig 7). Both types of connections were observed more frequently on the angiographic studies than in the anatomic series. In particular, termination into the posterior aspect of the CS appears as a frequent outflow route for the LCS, found in 32% of angiographic cases, compared with 13.8% reported in the anatomic study (4).

DSA, venous phase, in a 37-year-old woman undergoing a presurgical epilepsy workup (Wada test).
A, Right internal carotid injection, AP view. The right SMCV (arrow) drains toward the right transverse sinus via an LCS. A small anastomotic channel (arrowhead) joins the LCS to the posterior aspect of the CS at the skull base.
B, Right internal carotid injection, lateral view. The simultaneous opacification of the LCS and the CS (medial and lateral compartments) makes it impossible to differentiate them on the lateral view.
C, Left internal carotid injection, AP view. The left SMCV (arrow) drains toward the left pterygoid plexus (PP) via an LCS (arrowheads). There is an “en passant” connection between the LCS and the lateral compartment (L) of the CS.
Although simultaneous opacification of the LCS and CS may be observed, the LCS most often opacifies before the medial and lateral compartments of the ipsilateral CS (Fig 8). Three anatomic situations must be considered to understand these different patterns of opacification: 1) simultaneous opacification occurs when the LCS and the CS communicate via large anastomotic channels (Fig 7B) or when the LCS terminates into the posterior aspect of the CS (Fig 4); 2) when the LCS and CS are completely separated (Fig 5), the CS essentially drains blood from the high-resistance arterial beds of the ophthalmic and external carotid territories via the superior ophthalmic vein, while the LCS drains blood from the low-resistance cerebral arterial bed via the SMCV (the low resistance of the intracranial bed is coupled with a shorter circulation time, resulting in earlier opacification of the LCS); and 3) delayed opacification of the CS may also be observed when small anastomoses connect the LCS to the CS (Fig 7A) and allow for slow filling of the latter with blood of cortical origin. Delayed opacification of the CS thus occurs when the CS and the LCS are either totally separated (situation 2) or connected via small anastomoses (situation 3). In both cases, a transcavernous endovascular approach to the LCS would prove difficult or impossible for purely anatomic reasons. On the other hand, simultaneous opacification of the CS and LCS, indicating the presence of large connections (situation 1), would favor a transcavernous route to the LCS. A CS opacifying before an LCS was observed in one instance only, in a patient with viral nasal inflammation. In that case, early appearance of the nasal mucosa led to rapid contrast filling of the superior ophthalmic vein and CS, preceding the opacification of the LCS.
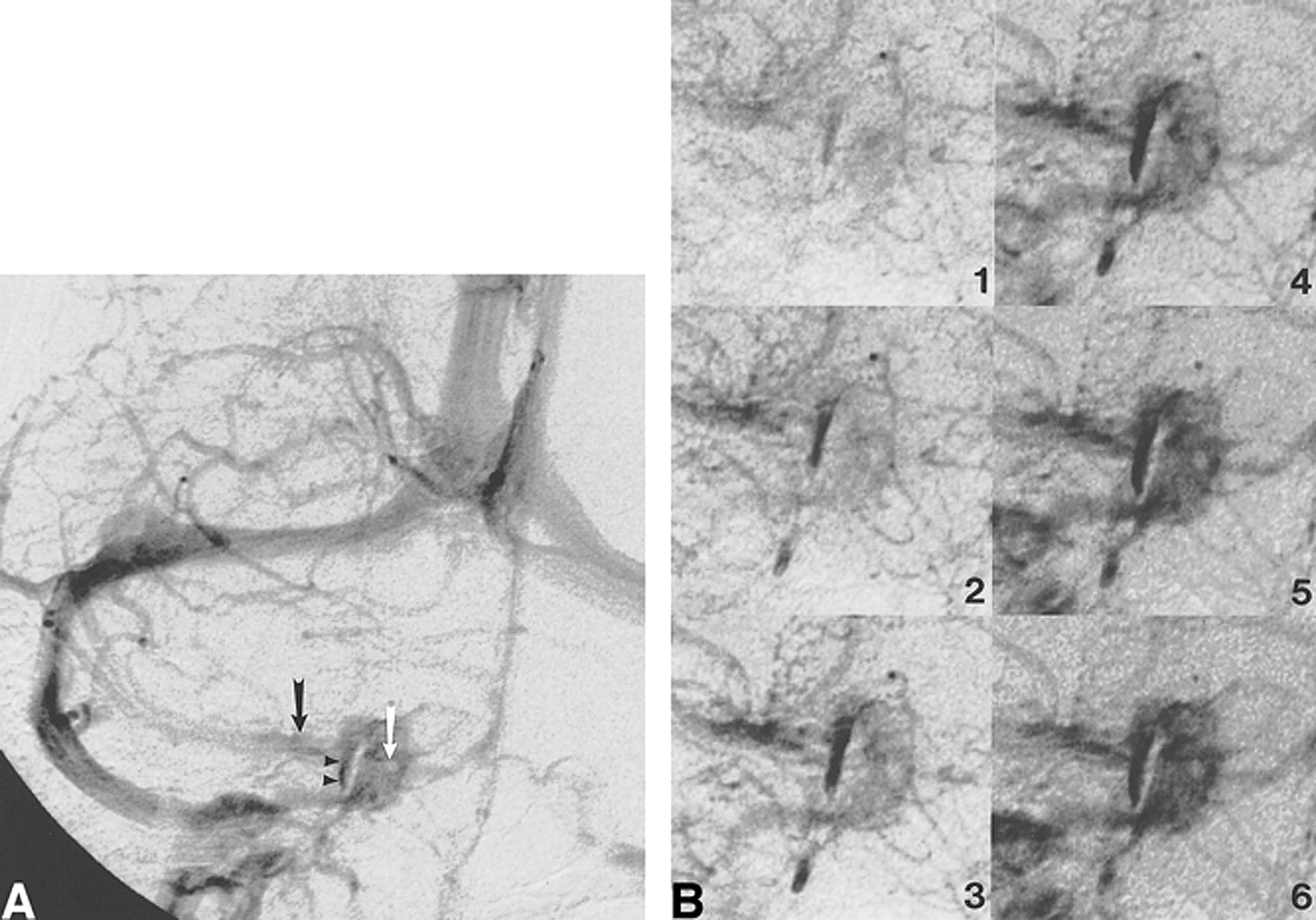
DSA, venous phase, in a 68-year-old man examined for carotid bifurcation atheromatous disease.
A, Right common carotid injection, AP view. The left SMCV (black arrow) drains into a right LCS (arrowheads). The right CS is opacified as well, although no significant connections are observed. Note the linear opacification defect of the inner layer of the CS lateral wall, separating the LCS from the lateral compartment of the CS. A second, round opacification defect is visible within the CS itself, corresponding to the cavernous segment of the right ICA (white arrow). This anatomic landmark enables one to discern the medial and lateral compartments of the CS.
B, Magnified view of the right laterosellar venous spaces. This dynamic sequence (1 to 6) was acquired at the rate of one image per second. Note that the LCS appears early in the sequence while the medial and lateral compartments of the CS show homogeneous opacification after a delay of approximately 5 seconds. This is consistent with the findings of Bonneville et al (2), who observed, during dynamic CT of the laterosellar venous spaces, a delay of 5 seconds between the visualization of distinct laterosellar veins and a homogeneous opacification of the CS. Note on the last image of the sequence the particularly well delineated inner layer of the CS lateral wall.
Embryologic Hypothesis
According to Padget (8), connections between the CS and the SMCV are usually not established before birth. During fetal life, the CS only receives blood from the superior ophthalmic vein, while cortical blood from the SMCV drains directly into the transverse sinus via the primitive tentorial sinus. Secondary anastomoses between these two embryologically distinct systems will eventually allow cortical venous drainage toward the CS. However, it now seems that connections occur earlier in the fetal period, at the time of formation of the lateral wall of the CS. Hakuba et al (9) have shown that the lateral wall of the CS is formed around the 8th week of gestation by a combination of an outer layer, the dura propria of the temporal lobe, and an inner layer, the dural sheaths of the third, fourth, and fifth cranial nerves. Expansion of the temporal lobe is thought to be responsible for the medial bulging of its dural covering, which comes to overlie and fuse with the preexisting dural layer of the third, fourth, and fifth cranial nerves, thus forming the lateral wall of the CS. It is conceivable that the same process produces a medial migration of the primitive tentorial sinus as well, bringing it close to the CS. The early formation of anastomoses between the superficial middle cerebral venous system and the CS was confirmed in the study by Knosp and coworkers (10). In their investigation of human fetuses between the 17th and 40th weeks of gestation, these authors observed connections between the SMCV and the CS in 20% of cases. These connections resulted either from a direct termination of the SMCV into the CS or from connections between a primitive tentorial sinus and the CS. It thus seems that the SMCV drainage pattern reaches its adult configuration during the fetal period, although further modifications, such as secondary anastomoses to the CS, may occur after birth.
In summary, we think that the primitive tentorial sinus, which drains cortical blood coming from the SMCV, migrates medially toward the CS region at the time of formation of the lateral wall of the CS, during the 8th week of gestation. Depending on the extent of migration and subsequent formation of anastomoses between the tentorial sinus and the CS, three adult SMCV drainage patterns may result: 1) persistence of a primitive tentorial sinus, coursing laterally in the temporal fossa and taking the name of paracavernous sinus in the adult; 2) presence of an LCS within the lateral wall of the CS, with or without secondary connections with the CS itself; or 3) direct termination of the SMCV into the CS, the classically described but anatomically and angiographically less often observed pattern.
Conclusion
The angiographic findings reported here are consistent with the concept that the laterosellar blood spaces should be divided into two embryologically, morphologically, and functionally independent systems with potential secondary connections (4, 8, 10): a medial system made up of the superior ophthalmic vein, the CS, and the inferior petrosal sinus; and a lateral system draining the cortical blood of the cerebral convexity through the SMCV toward the pterygoid plexus and/or the transversesinus. The latter pathway may take the form of a paracavernous sinus, an LCS, or a classic termination of the SMCV into the anterosuperior aspect of the CS, in decreasing order of frequency. Although the LCS is sometimes difficult to identify on DSA studies, owing to its close topographic relationship with the CS, it is an independent anatomic entity with characteristic angiographic features. Better knowledge of its course and connection patterns should enable more frequent recognition of the LCS on angiographic studies and improved evaluation of its potential clinical implications.
Footnotes
↵1 Presented in part at the annual meeting of the American Society of Neuroradiology, Philadelphia, May 1998.
- Received February 24, 2000.
- Copyright © American Society of Neuroradiology
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cerebral venous anatomy: implications for the neurointerventionalist
- Cerebral venous anatomy: implications for the neurointerventionalist
- Republished: Embolization of a cavernous carotid fistula through the vein of Labbe: a new alternative transvenous access route
- Embolization of a cavernous carotid fistula through the vein of Labbe: a new alternative transvenous access route
- New Concept in Cavernous Sinus Dural Arteriovenous Fistula: Correlation With Presenting Symptom and Venous Drainage Patterns
- The Sphenoparietal Sinus of Breschet: Does It Exist? An Anatomic Study