
Article Figures & Data
Figures
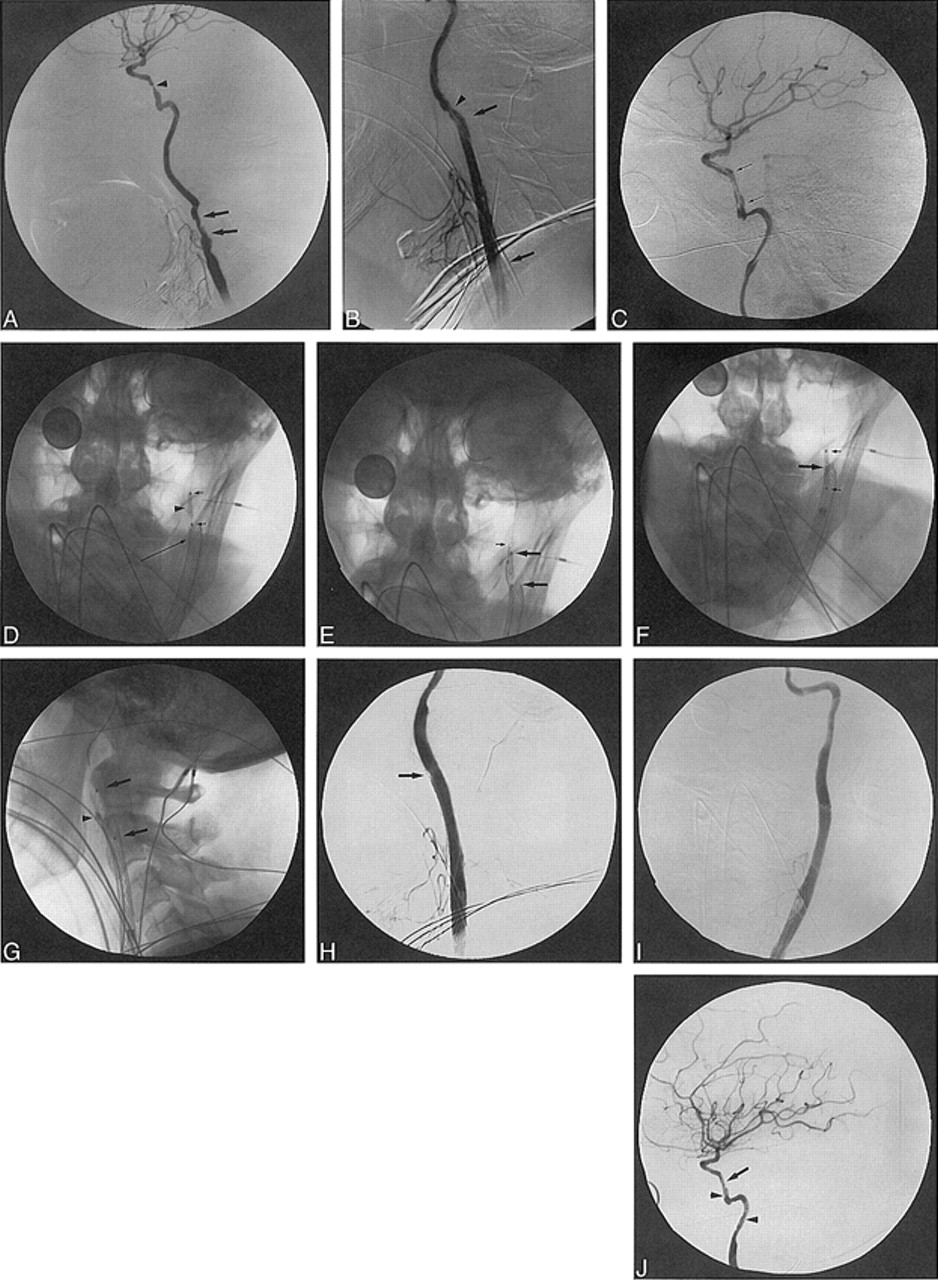
- fig 1.
63-year-old woman (with a Hunt and Hess grade of 4) who had subarachnoid hemorrhage from ruptured aneurysms of the left posterior carotid wall.
A, Lateral view from left ICA angiogram shows two large posterior carotid wall aneurysms (arrows), one of which is bilobate.
B, Lateral fluoroscopic image shows multiple GDCs within the superior aneurysm as well as a long, linear strand of coil (arrows) extending proximally into the cavernous and petrous portions of the ICA. A RapidTransit microcatheter is within the aneurysm and a dime (18 mm) is present for measuring purposes.
C, Lateral view from a left CCA angiogram through the guiding catheter shows near occlusion of the two aneurysms by a GDC, a linear strand of coil within the cavernous and petrous segments of the ICA, as well as a tangled mesh of unraveled coil (arrows) more proximally within the cervical segment.
D, Lateral fluoroscopic image from the angiogram in C better shows the coil mass in the cervical ICA (arrows) as well as the coil fragment (arrowhead) connecting this mass to the coils within the posterior carotid wall aneurysm. The RapidTransit microcatheter and dime are again visible.
E, Anteroposterior fluoroscopic image of the carotid bifurcation shows a Wallstent endoprosthesis pinning the migrated coil fragments (arrows) against the wall of the proximal cervical segment of the ICA.
F, Anteroposterior left CCA angiogram shows patency of the ICA and ECA in the region of the Wallstent. The stent crosses the bifurcation.
G, Six-month follow-up anteroposterior CCA angiogram shows mild intimal hyperplasia within the stent (arrows), without significant stenosis. There is continued patency of the ICA and ECA at the level of the stent.
H, Anteroposterior fluoroscopic image from the angiogram in G shows the coil mass (arrows) pinned to the wall of the ICA with the Wallstent.
I, Lateral fluoroscopic image shows multiple GDCs within the two aneurysms and a small linear coil fragment (arrows) extending from the aneurysms inferiorly into the cavernous and petrous segments of the ICA.
- fig 2.
Patient 2. A–C, Angiography: ECA occlusion distal to small superior thyroidal and lingual branches, irregular narrowing in cervical ICA (arrows) and severe stenosis in vertical petrous ICA (A); Wallstent across carotid bifurcation (arrows) with ECA branches patent, improved CCA contour/caliber after deployment, but mild ICA spasm distal to stent (B); inflated AVE stent delivery balloon (arrows) shows reduced petrous ICA stenosis while stent is unattached to uninflated balloon (C). D–G, Fluoroscopy: AVE stent (arrowhead) with delivery balloon (short arrows) withdrawn over ACS guidewire into cervical ICA (D); 2-mm microsnare (small arrow) around ACS guidewire before AVE stent stabilization for balloon catheter (large arrows) removal (18-mm dime for measurement) (E); microsnare around AVE stent (large arrow) beside undeployed Palmaz-Schatz stent mounted on Courier balloon catheter (small arrows) (F); Palmaz-Schatz stent (arrows) deployed in distal ICA with crushed AVE stent (arrowhead) against distal cervical ICA and microsnare attached (G). H–J, Angiography: adequate ICA lumen adjacent to crushed, pinned AVE stent (arrow) after Palmaz stent deployment (H); AP view confirms adequate ICA lumen (I); minimal residual petrous ICA stenosis (arrow) and normal filling of MCA and ACA at procedure's end but irregular distal cervical and petrous ICA (arrowheads) shows residual spasm/dissection (J).
- fig 3.
65-year-old man with recurrent squamous cell carcinoma of the neck surrounding the ECA branches who presented with significant oropharyngeal bleeding.
A, Lateral view from late arterial-phase right CCA angiogram shows vascular tumor blush (arrows) corresponding to recurrent neck tumor.
B, Lateral view from early arterial phase right CCA angiogram shows tiny branch (arrows) off proximal ECA supplying the tumor. Additional supply originates from the facial and lingual arteries (arrowhead).
C, Lateral view from a CCA angiogram shows an Envoy guiding catheter in the CCA, a coaxially placed RapidTransit microcatheter in the proximal ECA, and multiple GDCs within the proximal ECA. More distally positioned Flower coils are also seen in the ECA. There is continued filling of a small proximal tumor feeder (arrow).
D, Lateral view from a postembolization CCA angiogram shows near occlusion of the ECA with no further tumor blush or significant filling of the previously noted proximal feeding vessel.
E, Lateral fluoroscopic image of the carotid bifurcation shows the Wallstent providing support for GDC sacrifice of the ECA.











{kind=link}
{kind=link}
{kind=link}