
Abstract
Summary: We report the CT, MR imaging, and histologic findings in a patient with an intracranial mass diagnosed as xanthoma disseminatum (XD). The mass demonstrated radiographic findings typical for a glioma. However, histologic examination of brain and dermal lesions showed findings characteristic of XD. XD is a rare dermatologic disorder of unknown cause that may be accompanied by systemic manifestations. In rare cases, it can appear as an intracranial mass.
Xanthoma disseminatum (XD) is a rare dermatologic disorder of unknown cause that may be accompanied by systemic manifestations (1–6). It is a histiocytic disorder of non-Langerhans cell origin characterized by xanthomatous deposits affecting skin and mucosa in the absence of hyperlipidemia (3). Systemic involvement is common in this rare disorder and has been documented in virtually every organ system in the body (1, 3). CNS involvement has been described, but most CNS involvement reported has been extraaxial (2, 3). At least two prior reports of intraparenchymal brain involvement are present in the literature, but none include modern neuroimaging techniques such as MR imaging. We describe the MR imaging and histologic findings in a patient with disseminated XD and an intraparenchymal mass lesion mimicking a cerebral glioma.
Case Report
Clinical History and Physical Examination Findings
A 64-year-old Hispanic female presented to the emergency department (ED) with difficulty swallowing, dysarthria, and blurry vision for 2 weeks; these were accompanied by dizziness, nausea, and vomiting. She had a history of pneumonia 7 months before this ED visit that was successfully treated with antibiotics. Physical examination revealed a facial droop and findings suggestive of cerebral ischemia. Incidentally noted were multiple cutaneous lesions that were sessile and yellow; these were bilaterally present in the axillae.
Radiographic Findings
Because of a clinical suspicion of cerebral ischemia, a nonenhanced head CT scan was obtained in the ED. The CT scan showed findings consistent with an intracranial mass lesion involving both the right cerebral hemisphere and the right cerebellar hemisphere (Fig 1). Brain MR images obtained with intravenously administered contrast material showed a peripherally enhancing mass with associated vasogenic edema (Fig 2). The mass was located in the right cerebral hemispheric white matter, extending through the cerebral peduncle and into the right cerebellar hemisphere. A glioma was suspected, and stereotactic biopsy was performed in the right subinsular region (in the area of the enhancing mass) 2 days later.

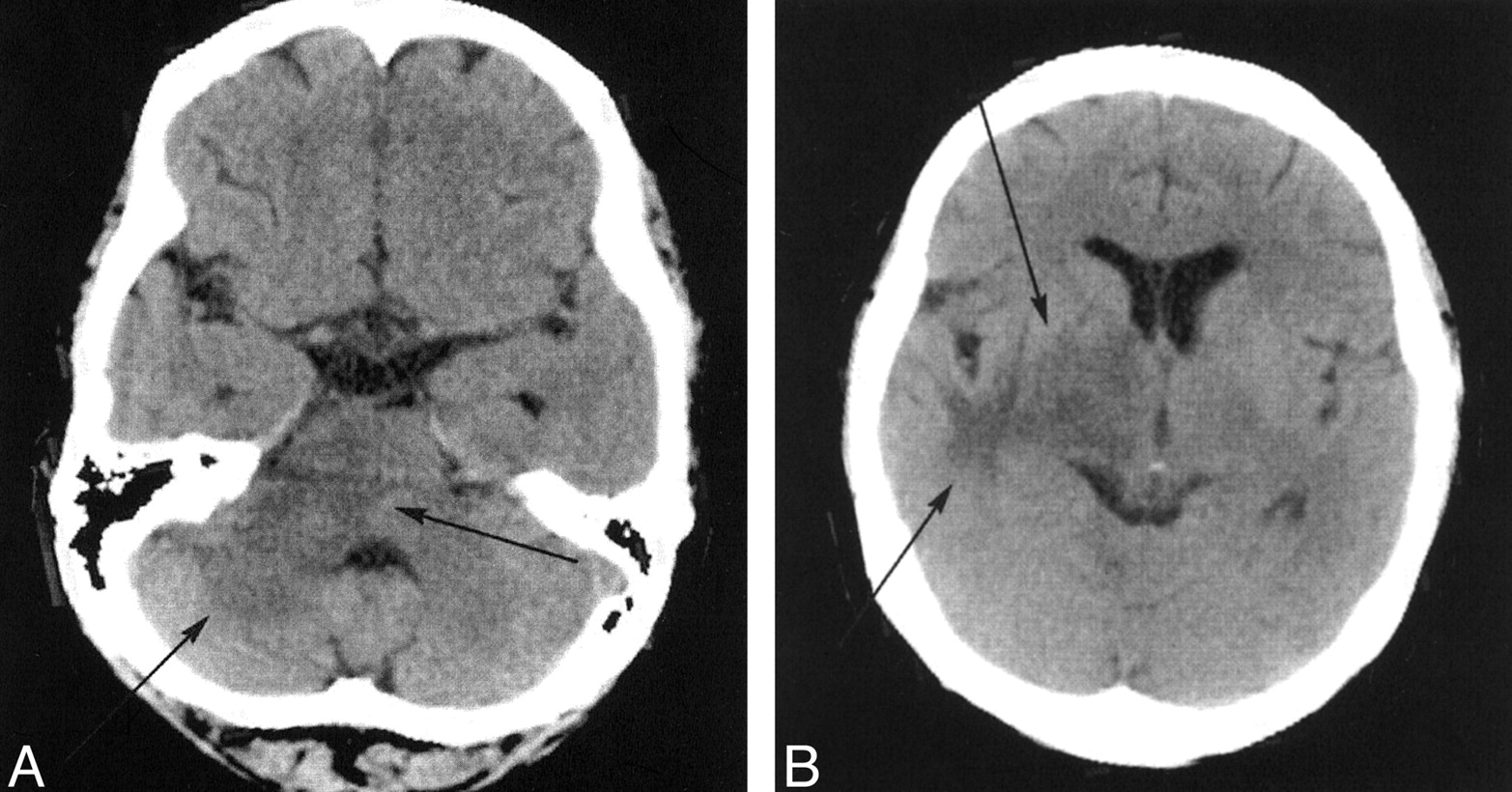
Axial nonenhanced CT scans reveal abnormal hypoattenuation in the right subinsular white matter, basal ganglia, and thalamus and within the middle cerebellar peduncle (arrows).
A, Image at the level of the middle cerebellar peduncle.
B, Image at the level of the insular cortex.
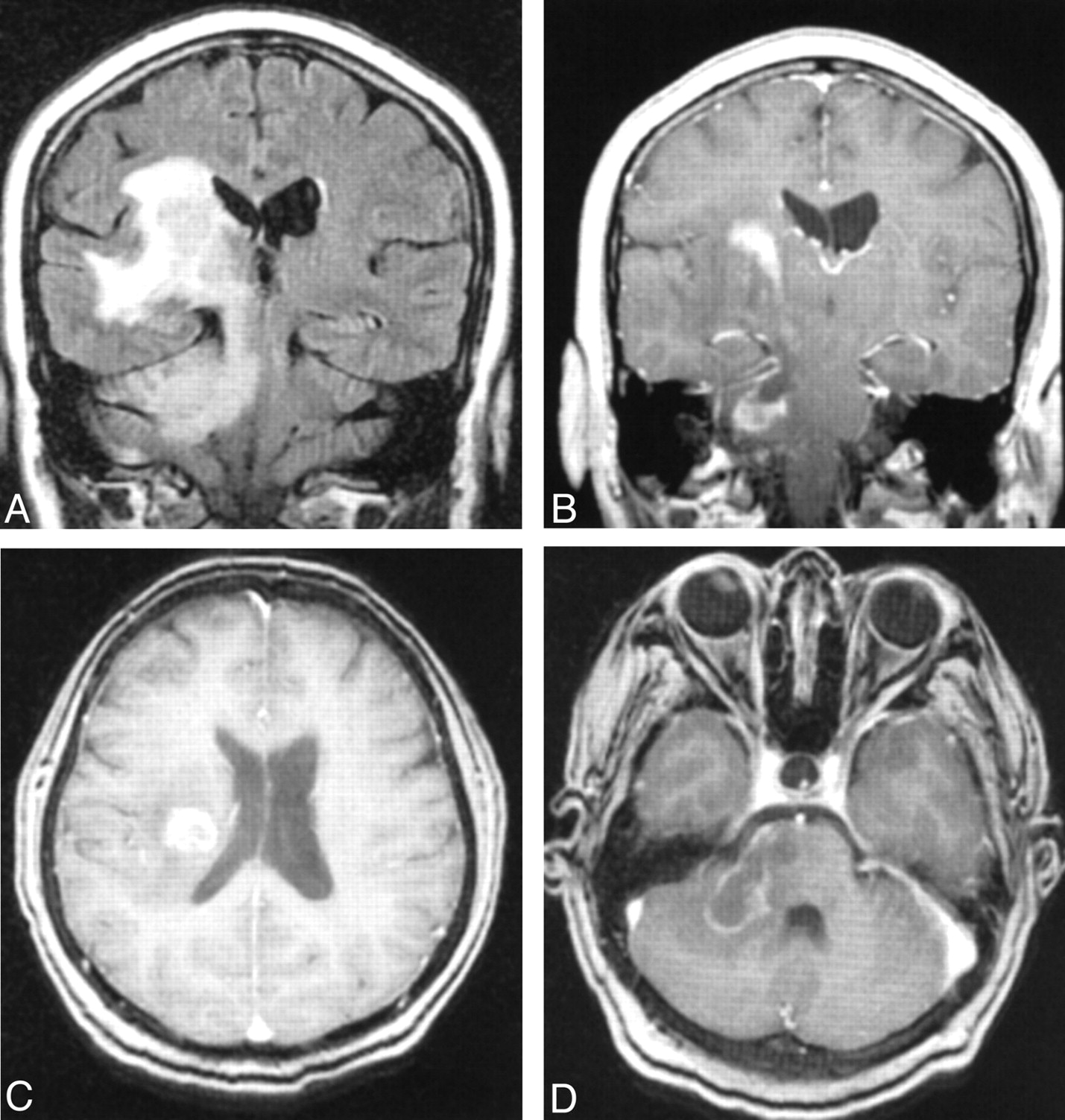
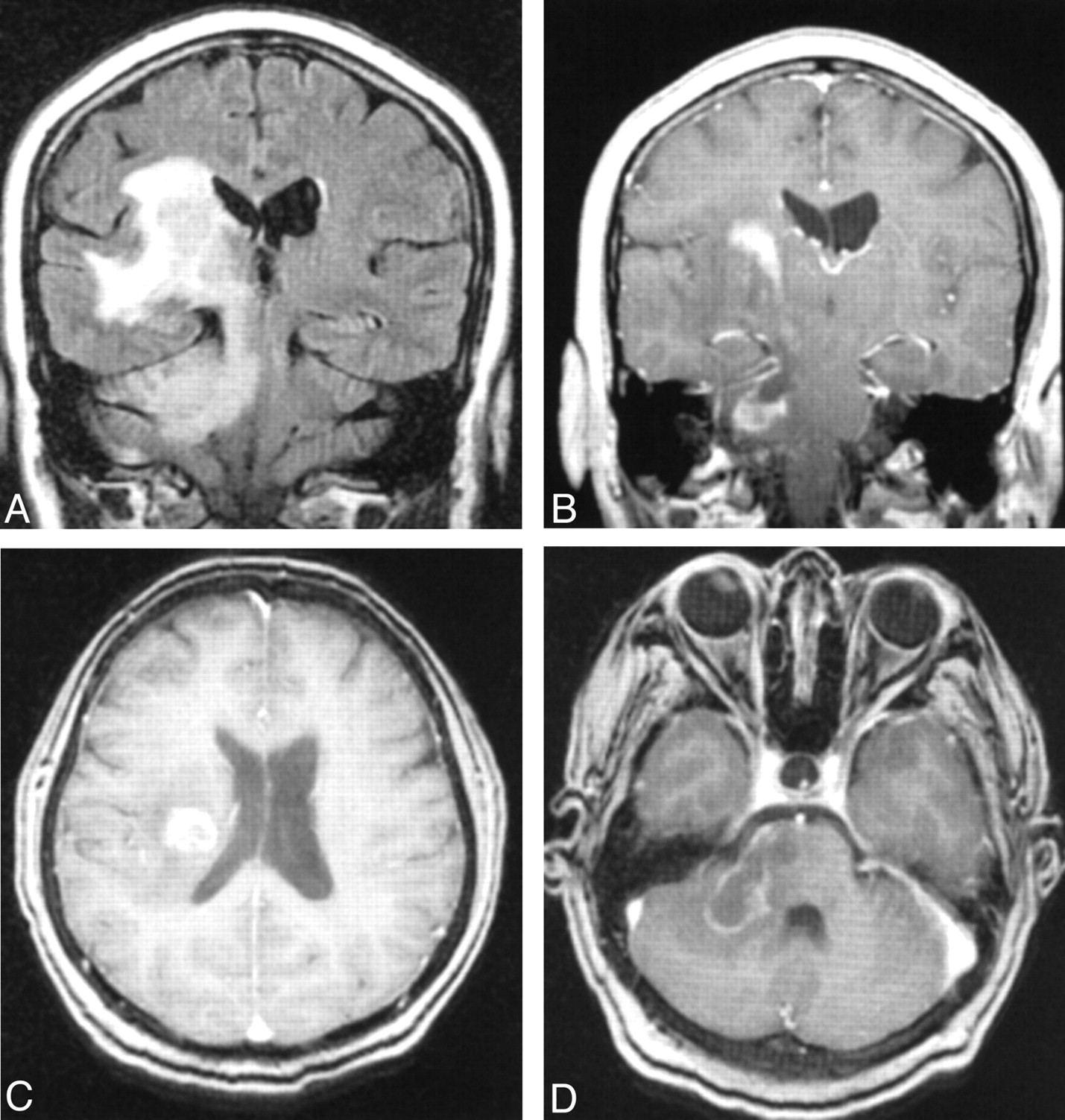
Brain MR images obtained at the time of initial clinical presentation show peripheral enhancement of a mass in the right cerebral white matter that extends through the cerebral peduncle and into the right cerebellar hemisphere via the right middle cerebellar peduncle.
A, Coronal fluid-attenuated inversion recovery (TR/TE/TI, 8000/112/2700) image demonstrates marked adjacent vasogenic edema.
B, Coronal spin-echo gadolinium-enhanced T1-weighted image (TR/TE, 600/15).
C and D, Axial spoiled-gradient postcontrast T1-weighted images (9.2/2.0; flip angle, 20° at the level of the lateral ventricles [C] and middle cerebellar peduncle [D]).
Histologic Findings
Histologic examination with hematoxylin-eosin staining showed a hypercellular lesion with numerous vacuolated or foamy histiocytes (Fig 3A). Focal blood vessels were surrounded by small mature lymphocytes. Immunocytochemical stains revealed that the histiocytes were positive for CD68, a marker for histiocytes (Fig 3B), and negative for gliofibrillary acidic protein (Fig 3C). The cells did not stain with S-100 or HAM-56.

Histopathologic findings.
A, Photomicrograph of a routine paraffin section stained with hematoxylin-eosin (from a stereotactic brain biopsy) shows a hypercellular lesion populated by foamy histiocytes with uniform, benign nuclei (original magnification, ×360).
B, Photomicrograph of the brain biopsy stained with immunocytochemical method for CD68 antigen shows granular cytoplasmic positivity (arrows) (original magnification, ×360).
C, The stain for gliofibrillary acidic protein shows the histiocytes that are negative and a few reactive astrocytes and their processes that are darkly stained (arrows) (original magnification, ×120).
To confirm the diagnosis of XD, a right axillary dermal lesion was examined at biopsy. Histologic analysis revealed diffuse infiltration of the dermis with histiocytes, which exhibited central nuclei and clear, vacuolated cytoplasm. A few lymphocytes were distributed in a perivascular fashion. The histologic findings were equivalent to the histologic findings in the cerebral lesion. The biopsy results were consistent with XD.
Treatment and Follow-up
The patient was treated with oral steroid medications (dexamethasone 2 mg, four times daily) and followed up with repeat brain MR imaging at 2-month intervals until 4 months after the diagnosis. The patient’s facial droop, dysarthria, and nausea and vomiting improved, but she remained weak on the left side of her body. Within the first week after biopsy, notable thrombocytopenia developed; this also improved. After 3 months of steroid therapy, she still had some weakness on the left side of her body, but it was improved. The dexamethasone was slowly tapered over 1 month, to 2 mg/d.
Follow-up brain images obtained 4 months after diagnosis showed a decrease in the size of the mass lesion and the associated edema. Small amounts of residual enhancement and edema were present on the 4-month follow-up image (Fig 4). The patient’s left-sided weakness was much improved, and she was able to ambulate without assistance. Also at that time, the decision was made to wean the patient from steroid therapy. Continued follow-up brain imaging was recommended until the mass stabilizes completely (as documented with MR imaging) or until the enhancement completely abates. At the time of this writing, 9 months have passed since the diagnosis, and the patient has not returned for any acute flare of the disease. She has missed some scheduled follow-up appointments and brain imaging studies, and her clinical course since the 4-month follow-up appointment is unknown.
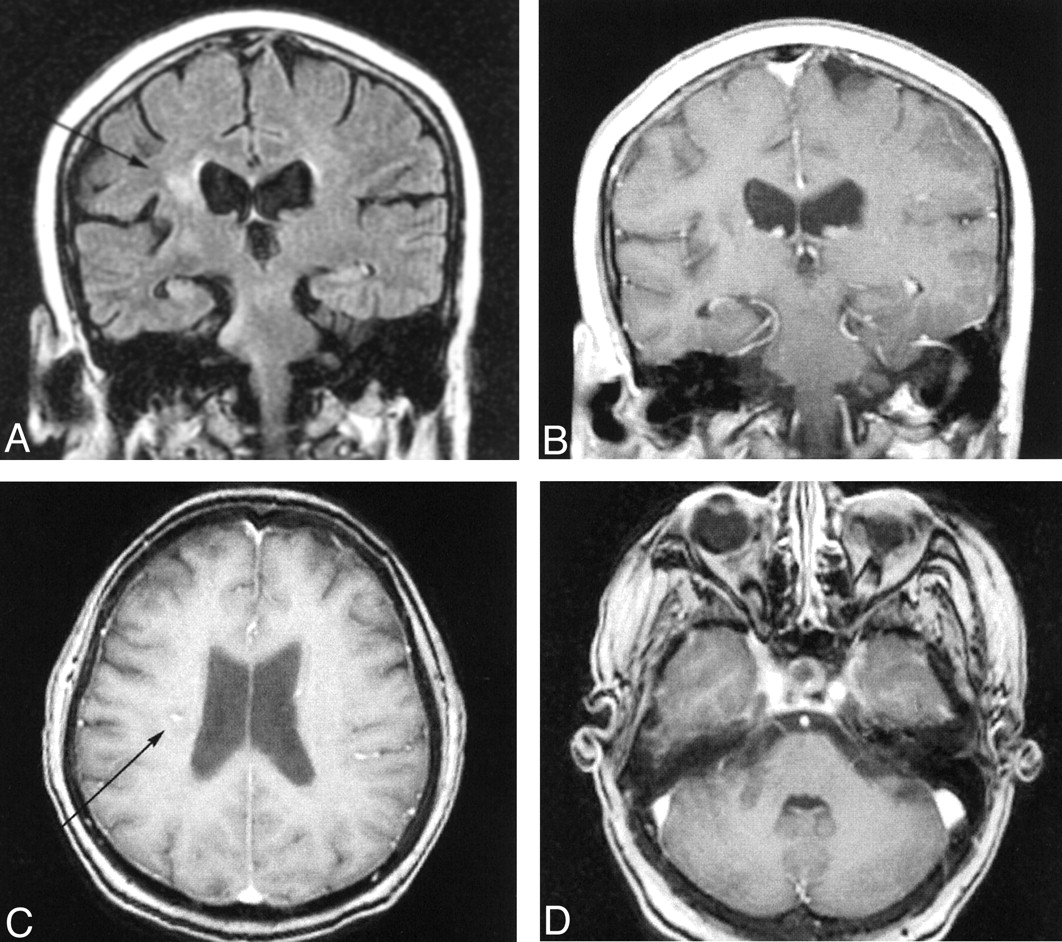
Follow-up brain MR images obtained 4 months post diagnosis, after treatment with steroids. The appearance of the brain is markedly improved compared with the appearance at diagnosis (see Fig 2).
A, Coronal fluid-attenuated inversion recovery (8000/112/2700) shows only small amounts of hyperintense signal.
B, Coronal spin-echo gadolinium-enhanced T1-weighted image (600/15).
C and D, Axial spoiled-gradient postcontrast T1-weighted images (9 .2/2.0; flip angle, 20° at the levels of the lateral ventricles [C] and middle cerebellar peduncle [D]) show small amounts of contrast enhancement (arrows).
Discussion
XD is a rare systemic disorder characterized by xanthomatous deposits throughout the body, particularly in the skin (1–6). Because of the small number of cases reported in the literature, considerable confusion exists regarding its name, its distinction from Langerhans cell histiopathies, its treatment, and its extracutaneous manifestations.
Von Graefe is credited with the first description of XD in 1867. His case was later reviewed by Virchow in 1871, who named it xanthelasma multiplex. (3) Other names for the same condition include xanthosiderohistiocystosis, juvenile xanthogranulomatosis, xanthogranulomatosis, and Montgomery syndrome (1–3). Chiari first reported intraparenchymal CNS disease; a case with pontine involvement was described (3).
XD was originally considered to overlap with other histiocytic conditions such as Hand-Schuller-Christian (H-C-D) disease (3). With the advent of advanced immunochemical staining techniques, XD has been clearly distinguishable from the Langerhans cell histiopathies only in the last 20 years. Specifically, XD histiocytes are S-100 protein negative and lack Birbeck granules; these features differentiate this entity from the Langerhans cell histiopathies such as H-S-C disease. Thus, considerable controversy exists as to how many cases in the premodern literature truly represent XD. To date, approximately 100 cases of intracranial XD have been reported, with only 19 that satisfy current diagnostic standards (3).
XD is included in the differential diagnosis of systemic histiocytic lesions and must be considered in the pathologic approach to histiocytic lesions of the CNS. Its prognosis is good, and spontaneous remissions are occasionally reported (1–3). Some cases, however, have a progressive course and result in considerable morbidity and mortality. This is particularly true of CNS disease, in which the progression to death has been the most frequent outcome in the previous literature (1–3).
The most common initial presentation of CNS involvement with XD is diabetes insipidus (2, 3). The reason for this occurrence has been postulated to be the mass effect from involvement of the sella turcica and infundibulum, although one author has raised the possibility that intrapituitary deposits of histiocytes cause pathologic disruption of the pituitary gland (2). Clinical presentation with strokelike symptoms (as in the current case) is uncommon.
Treatment of XD has been highly variable, with surgical debulking, radiation therapy, and steroid therapy all used with varying degrees of success (1–3). In our case, steroid therapy has nearly completely cured the patient of her intracranial lesion, although cutaneous manifestations persist as of this writing. Further imaging follow-up will be useful to ensure regression of the intracranial lesion (1–6).
Conclusion
The radiographic appearance of XD in our case mimicked that of a cerebral glioma, with peripheral contrast enhancement and associated vasogenic edema. This lesion tracked along white matter fibers through the cerebral peduncle, raising the possibility that it may spread through the brain in a manner similar to that seen with cerebral gliomas. CNS XD is sufficiently rare that routine inclusion in a radiologic differential diagnosis for intracranial mass lesions is unwarranted.
- Received June 3, 2002.
- Accepted after revision July 8, 2002.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.