
Abstract
BACKGROUND AND PURPOSE: Prolonged T2 relaxation time of denervated muscle has been described in several clinical and experimental studies. The purpose of this study was to evaluate the utility of MR imaging in the diagnosis of neurogenic muscle disorders compared with that of clinical and electrophysiologic examination.
METHODS: In a prospective study, 40 consecutive patients clinically presenting with a foot drop were included. MR imaging of the lower leg included axial T1-weighted and axial turbo inversion recovery magnitude (TIRM) sequences. Two readers blinded to clinical data evaluated T1-weighted images for anatomic localization of affected muscles and TIRM images for patterns of signal intensity increase. After MR imaging, a detailed neurophysiologic examination was performed. Cause of foot drop was independently determined on the basis of MR and electrophysiologic data.
RESULTS: Clinical examination and electromyography (EMG) disclosed 20 peroneal nerve lesions, nine cases of L5 radiculopathy, and 11 nerve lesions extending beyond neural structures. MR imaging revealed three distinct patterns of signal intensity increase on TIRM images: peroneal nerve pattern, L5 pattern, and unspecific pattern. MR imaging and EMG findings were in agreement in 37 (92%) of 40 patients. In three patients, MR imaging revealed a more widespread involvement than did EMG. In one of these patients, denervation in the corresponding muscle was validated by follow-up EMG. No false-negative diagnoses were made by use of MR imaging as compared with use of EMG.
CONCLUSION: MR imaging improves accuracy in the differential diagnosis of peripheral nerve lesions compared with that of EMG and can supplement EMG in the diagnosis of denervated muscles.
As a supplement to clinical examination, electromyography (EMG) is considered the reference standard in the evaluation of denervated muscle. Nevertheless, the diagnosis of an underlying nerve lesion in affected muscles made on the basis of EMG findings is not always unequivocal. MR imaging has been introduced in the diagnosis of denervated muscles. MR alterations are characterized by a prolongation of T1 and T2 relaxation times (1). The feasibility of MR imaging to reveal denervated muscles has been shown in several experimental and clinical studies (2–4). Nonetheless, whether MR imaging is a scientifically interesting but otherwise unnecessary investigative tool in neuromuscular disorders or whether it has the potential to improve the differential diagnosis of peripheral nerve lesions remains a question. In the present study, we compared MR and EMG findings in the evaluation of neurogenic foot drop as an example of a frequently encountered problem in the clinical and routine electrophysiologic examination to assess the clinical utility of MR imaging in neurogenic muscle disorders.
Methods
A prospective study comprised 40 consecutive patients (mean age, 41 years; age range, 17–81 years; nine female patients, 31 male patients [Table]) who clinically presented with a foot drop (muscle strength, ≤3/5 [Medical Research Council scale]) to the clinical neurophysiology laboratory of the department of neurology. These patients were referred by neurologists or neurosurgeons or were seen as part of the neuromuscular consultation service of the university hospital. The study was approved by the local ethics committee, and informed consent was obtained from every patient. After neurologic examination, patients underwent MR imaging of the proximal lower legs on a clinical 1.5-T system (Vision; Siemens, Erlangen, Germany) with a round surface coil covering an area from the knee joint to 20 cm below. The MR protocol consisted of a turbo inversion recovery magnitude (TIRM) sequence (TR/TE/TI, 6250/60/150; field of view [FOV], 300 mm2) and a T1-weighted spin-echo sequence (TR/TE, 460 ms/14 ms; FOV, 300 mm2). All MR sections were obtained in the axial plane with a section thickness of 6 mm. The electrophysiologic examination was performed within 1 week after MR imaging to avoid possible artifacts arising from multiple needle insertions. The examination was performed by staff of the electrophysiology laboratory and included nerve conduction studies and EMG of muscles, depending on the clinical presentation of the patient. On MR images, denervated muscles were readily distinguished from unaffected muscles by a signal intensity increase on TIRM images. The anatomic localization of the affected muscles was determined on T1-weighted images. The films were independently evaluated by two investigators (M.B., A.J.B.) blinded to each other’s results and the results of the clinical and electrophysiologic examination.
Comparison of MR and EMG findings
Results
Three Distinct Lesion Patterns: MR Findings
Peroneal nerve pattern.—
Peroneal nerve lesions (Fig 1) were characterized by a restricted involvement of the anterior tibial and extensor digitorum muscle (if the deep ramus of the nerve was affected), the long peroneal muscle (if the superficial branch was damaged), or a combination of both branches. Lesions outside these three muscles precluded the diagnosis of an isolated peroneal nerve lesion. Electrophysiologic studies typically demonstrated conduction failure or conduction slowing of the peroneal nerve at the fibular head and acute or chronic neurogenic changes in the corresponding muscles (Fig 1C and D).

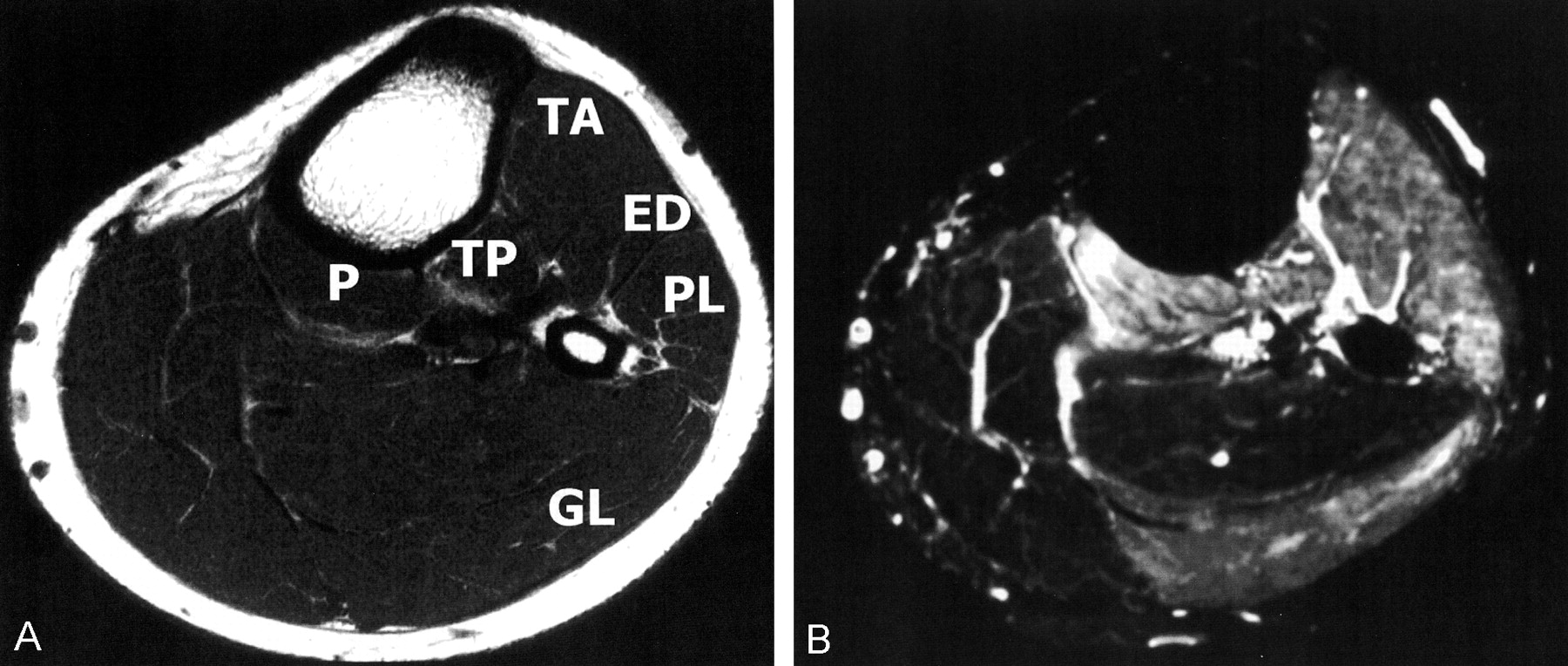
Electrophysiologic and MR changes in common peroneal nerve palsy.
A, Axial T1-weighted image localizes affected muscles. TA indicates the anterior tibial muscles; ED, the extensor digitorum; and PL, the long peroneal muscle. No abnormalities are shown.
B, Axial TIRM image depicts increased signal intensity in the TA, ED, and PL muscles, a pattern compatible with a common peroneal nerve lesion.
C, EMG recording shows spontaneous activity in the TA and PL muscle; in the posterior tibial (TP), there is normal insertional activity.
D, On stimulation of the distal peroneal nerve, no compound muscle action potential (CMAP) can be recorded in the extensor digitorum brevis muscle of the foot.
L5 radicular pattern.—
In L5 nerve root radiculopathy (Fig 2), increased signal intensity was present in the posterior tibial and popliteus muscle in addition to the three muscles involved in common peroneal nerve lesions. Typically, conduction studies of the peroneal nerve would not show conduction failure at the fibular head, but a significant reduction of the amplitude of the compound muscle action potential and acute or chronic neurogenic changes in the anterior and posterior tibial, extensor digitorum, long peroneal, and popliteus muscle (Fig 2C and D) could exist.

Electrophysiologic and MR changes in L5 nerve root lesion.
A, Axial T1-weighted image localizes affected muscles. No abnormalities are evident.
B,Axial TIRM image reveals a signal intensity increase in the TA, ED, PL, TP, and popliteus (P) muscles. This pattern was consistent with an L5 nerve root lesion.
C, EMG shows spontaneous activity in the TA, extensor hallucis longus (EHL), and TP muscles; as with MR results, these findings are consistent with a lesion of the L5 root.
D, Nerve conduction studies of the peroneal nerve show normal CMAP after stimulation of the peroneal nerve, at the level of the ankle, distal and proximal to the fibular head (amplitude, 9 mV; nerve conduction velocity, 50 m/s). In this patient, a lumbar disk herniation was confirmed at surgery.
Unspecific pattern.—
A third pattern (Fig 3) represented a more widespread lesion that included at least one of the muscles innervated by L5 or the peroneal nerve and portions of the gastrocnemius or soleus muscle. Electrophysiologic investigations typically showed neurogenic changes in these muscles, and nerve conduction studies revealed abnormalities in the sural or tibial neurography that were unaffected in both L5 radiculopathies and isolated peroneal nerve lesions.

MR images obtained in a patient who had partial sciatic nerve damage of nonspecific pattern after a motorcycle accident.
A, Axial T1-weighted localizes affected muscles.
B, Axial TIRM image shows high signal intensity in the TA, ED, and medial head of the gastrocnemius (GM) muscles.
Electrophysiologic Evaluation
Electrophysiologic examination revealed 20 lesions of the peroneal nerve, nine L5 radiculopathies, and 11 nonspecific lesions extending the sole innervation of the peroneal nerve or the L5 nerve root. Of the nonspecific lesions, eight had a partial or complete lesion of the sciatic nerve, and in one patient each a lesion of the lumbosacral plexus, the cauda equina, and the L5 and S1 nerve root in combination was diagnosed.
Correlation between MR and Electrophysiologic Results
MR findings were compared with those of electrophysiologic studies and clinical evaluation. MR findings were in agreement with those of electrophysiologic study in 92% (37/40) of patients. There was disagreement in two (10%) of the 20 cases of isolated peroneal nerve palsies and in one (11%) of the nine cases of L5 radiculopathies, whereas no discrepancies were found for the diagnosis of the 11 cases involving a more extensive lesion. No disagreement in MR findings existed between the two independent neuroradiologists. Two of the three patients in whom a discrepancy between neurophysiologic and MR diagnosis occurred are discussed in detail below; the third patient revealed a similar underestimation of the extent of denervated muscles on EMG recordings as compared with extent revealed by MR imaging. These examples show that the addition of MR imaging to the diagnostic procedure improved the accuracy of the diagnosis.
Case 1.—
A 35-year-old male patient presented with a 2-month history of left-sided sciatica. Two weeks before presentation, he had noticed a sudden onset of foot drop and hypoesthesia on the dorsum of the foot. On examination, he showed weakness of foot extension (3/5), extension of the great toe (4/5), and supination (4/5). The ankle jerk was reduced on the left, and there was hypoesthesia corresponding to L5 dermatome and pain radiating into the L5 and S1 dermatomes. CT of the lumbar spine revealed a large left mediolateral disk prolapse affecting the L5 nerve root and a caudally sequestered disk herniation compressing the left S1 nerve root. EMG showed the typical signs of acute muscle denervation, such as positive sharp waves, fibrillation potentials, and reduced interference pattern in the extensor hallucis muscle, but the vastus medialis muscle and the medial head of the gastrocnemius muscle appeared unaffected. MR findings were normal on T1-weighted images (Fig 4A), but increased signal intensity was present on the TIRM image in the anterior and posterior tibial muscle, the extensor digitorum muscle, the peroneal muscle, and the lateral but not the medial head of the gastrocnemius muscle (Fig 4B). Thus, although EMG and MR imaging showed congruent results of the examined muscles, MR imaging revealed a more extensive denervation than did EMG. Intraoperatively, large disk herniation compressing both the left L5 and S1 root was verified, and symptoms remitted postoperatively. In this patient, there was clear involvement of an S1-innervated muscle that had not been detected by the EMG recording because only one of the two heads of the gastrocnemius muscle had been studied.
MR images obtained in a 35-year-old male patient who presented with a 2-month history of left-sided sciatica due to lumbar disk herniation. MR imaging revealed a more widespread involvement of muscles of nonspecific pattern than did routine EMG (not shown).
A, Axial T1-weighted image localizes affected muscles.
B, Axial TIRM image not only shows signal intensity increase in the TA, ED, PL, P, and TP muscles (L5 radicular pattern), but also in the lateral head of the gastrocnemius (GL) muscle.
EMG studied only the medial head of the GL; no neurogenic changes were found, and the diagnosis of an L5 nerve root compression was made. CT of the lumbar spine revealed a large disk herniation compressing both the L5 and S1 nerve root (not shown) that were subsequently confirmed at surgery.
Case 2.—
A 42-year-old female patient presented with a 5-month history of a left foot drop and hypoesthesia on the dorsum of the foot. She had worn a splint that was fixed around the proximal third of the lower leg for several days. On examination, she revealed a palsy of the large toe, toe, and foot weakness extension and pronation (3/5). Hypoesthesia corresponded to innervation territory of the common peroneal nerve. Nerve conduction studies showed an absent response of the extensor digitorum muscle after stimulation of the deep branch of the peroneal nerve at the ankle and a reduced amplitude of the anterior tibial muscle after stimulation of the common peroneal nerve above (6.9 mV) and below the fibular head without evidence for a conduction block at a normal conduction velocity (45 m/s). Needle EMG of the proximal lower leg did not reveal active denervation in the anterior tibial muscle. MR imaging of the proximal lower leg was normal (Fig 5A and B), but further distally, the TIRM sequence revealed an increased signal intensity in all muscles of the anterior compartment (Fig 5C and D). Additional follow-up EMG confirmed absence of positive sharp waves and fibrillation potentials in the proximal portions of the anterior tibial and long peroneal muscle, which were nonetheless present further distally. Thus, in this case MR imaging helped detect denervation in a part of the anterior tibial muscle that had escaped from routine EMG diagnosis and perfectly pointed to the actual lesion (peroneal nerve damage by fixation of the splint).

MR images obtained in a 42-year-old female patient who presented with a foot drop after splint fixation around the proximal lower leg. This case exemplifies that MR imaging is capable of demonstrating the entire muscle, whereas EMG can only study parts of a muscle.
A, Axial T1-weighted image obtained just below knee level localizes affected muscles.
B, Axial TIRM image obtained at the level of A does not show signal intensity abnormality.
C, Axial T1-weighted image obtained approximately 4 cm below knee level localizes affected muscles.
D, Axial TIRM image obtained approximately 4 cm below knee level shows marked signal intensity increase in the TA, ED, and PL, findings consistent with a peroneal nerve lesion.
Initial needle EMG (not shown) obtained just below the knee level did not reveal denervation; however, follow-up examination further distally showed marked denervation in the TA, ED, and PL muscles.
Discussion
MR signal intensity changes in denervated muscle were first decribed in 1986 by Polak et al (1), who reported a prolongation of both T1 and T2 relaxation times in denervated muscle after transection of the sciatic nerve. Both a widening of the extracellular space (1) and increased blood perfusion (5) in denervated muscles have been suggested as the underlying pathomechanism. By now, several clinical reports exist on the application of MR imaging of denervated muscle (2–4, 6). Most of these reports describe the feasibility of MR imaging to depict denervated muscle (2–4). More recently, a correlation between the signal intensity increase on T2-weighted images and the extent of denervation revealed by EMG has been reported (6). Apart from a scientific point of interest, however, MR imaging is not yet used to diagnose the pattern of muscle denervation.
Electrophysiologic examination remains the reference standard in the diagnosis of neuromuscular disorders because, until now, no data were available on the value of MR imaging compared with that of clinical and electrophysiologic examination. In the present study, distinct patterns of affected muscles on MR images were applied to discover the affected nerve. Independently, EMG and MR imaging revealed an overall agreement rate of 92% (37/40 patients) in the diagnosis of an acute foot drop. The three patients with discordant findings exhibited a more extensive involvement of muscles on MR images than on EMG recordings. In two patients, follow-up EMG was not performed. Although intraoperative findings during lumbar spine surgery supported the MR diagnosis in both cases, this was not verified by the reference standard of needle EMG; therefore, these cases could conceivably represent false-positive findings. In one patient, involvement of the distal part of the anterior tibial muscle on MR images was validated by follow-up EMG examination.
In this patient series, no false-negative diagnoses were made on the basis of MR findings as compared with EMG findings. There were, however, no cases of chronic denervation, which may not reveal high signal intensity on TIRM images and thus may lead to false-negative diagnoses. These results suggest that in selected patients with acute and subacute denervation, MR imaging may be more accurate in the differential diagnosis of peripheral nerve lesions as compared with EMG. Beyond that, MR imaging has several additional advantages. First, it is noninvasive, which is especially valuable in the examination of children or patients with coagulation disorders in whom needle EMG is either difficult to perform or would require alteration of medical treatment. Second, the entire cross-section of the leg or arm can be visualized in contrast to the interpretation of EMG data being restricted to the number of muscles under study. Figure 4 clearly demonstrates that, if denervation is present in muscles that are clinically not affected, these muscles probably will not be part of the EMG examination. Figure 5 also shows that denervation may be present only in parts of one muscle and that needle EMG examination in one or two locations of the muscle may not be representative of the whole muscle. Third, the electrophysiologic examination is a challenging technique that is observer-dependent and of limited reproducibility, whereas MR imaging does not have these disadvantages. Fourth, apart from demonstrating denervation, MR imaging can show altered muscle tissue (ie, atrophy, fatty replacement of muscle fibers [7], hypertrophy). In this study, we did not look for the nerve lesion site on MR images, because the study focused on pattern recognition of denervated muscle groups; however, MR imaging may also depict the nerve lesion (8–10). By demonstrating both the nerve lesion and the subsequently denervated muscle, MR imaging is a promising additional diagnostic tool for peripheral nerve disorders (11). Finally, experimental data indicate that MR imaging can show denervated muscle as early as 24 hours after the nerve lesion forms (12, 13). In a similar experimental setting, needle EMG depicts spontaneous activity after 3 days, at the earliest (14). In a clinical setting, spontaneous activity is found by use of needle EMG as early as 7 to 14 days after the denervation. Thus, MR imaging may narrow this diagnostic gap between occurrence of a nerve lesion and the earliest detection of denervated muscle.
Conclusion
MR imaging is an accurate tool in the differential diagnosis of peripheral nerve lesions by pattern recognition of denervated muscles. It may be a valuable additional test to EMG in the differential diagnosis of peripheral nerve lesions.
Footnotes
Present address of M.K.: Institute of Child Health and Institute of Neurology, University College London, England.
References
- Received December 4, 2002.
- Accepted after revision March 3, 2003.
- Copyright © American Society of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}