
Abstract
Summary: Cranial fasciitis is a benign fibroblastic tumor of the skull found almost exclusively in young children. It is histologically identical to nodular fasciitis. We present the clinical, radiologic, and pathologic findings of a 7-month-old male infant with cranial fasciitis of the skull. Herein, we include the first description of this entity’s diffusion-weighted imaging appearance. Although rare, cranial fasciitis can mimic more aggressive processes both clinically and radiographically.
Cranial fasciitis is a rare benign tumor of the skull that occurs almost exclusively in children younger than 6 years (1). Clinically, it typically presents as a single palpable, painless scalp mass, and it rarely produces neurologic symptoms. Radiographically, the lesion usually presents as a single lytic defect in the calvaria with an associated soft tissue mass. In this report, we discuss the salient clinical, radiographic, and pathologic findings of a case of cranial fasciitis in a 7-month-old male infant.
Case Report
A seven-month-old male infant presented with a palpable scalp mass of the parietotemporal region that his mother first noticed 2 months before presentation. The mother stated that it had grown rapidly since that time, but it did not appear to cause the child any pain or discomfort. There was no history of trauma, seizure, fever, proptosis, vomiting, rash, or ear infections.
Physical examination revealed a painless mass over the right parietotemporal region that measured approximately 2.0 cm in diameter. There was no discoloration of the overlying skin and no fluctuance. No focal neurologic findings were noted, and the remainder of the examination was unremarkable.
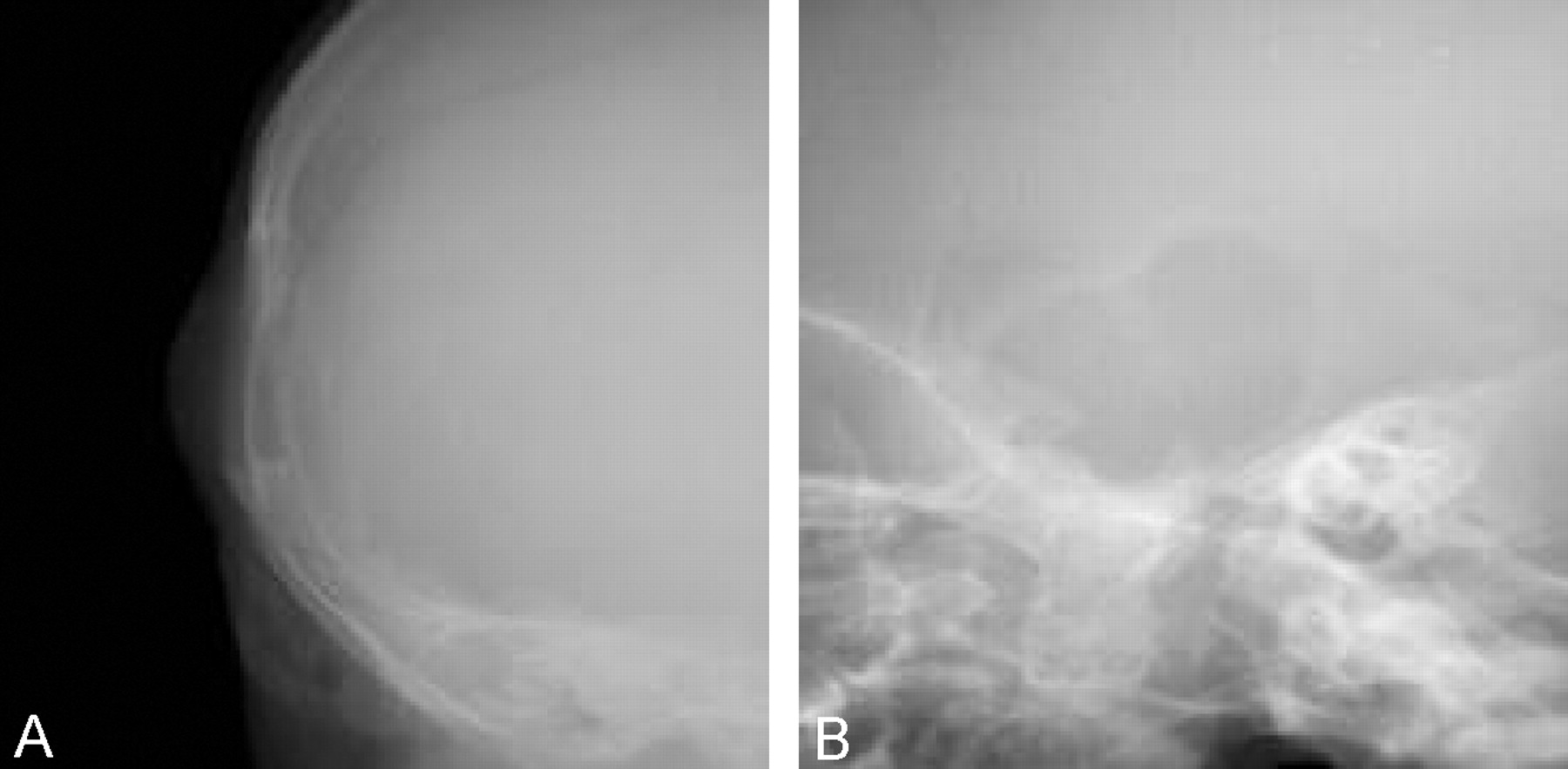
A plain radiographic skeletal survey was performed because of clinical suspicion of eosinophilic granuloma. This showed a 2.5-cm, well-circumscribed oval lytic defect in the right calvaria with an associated soft tissue mass of the scalp (Fig 1A and B). No other lesions were identified in the axial or appendicular skeleton.
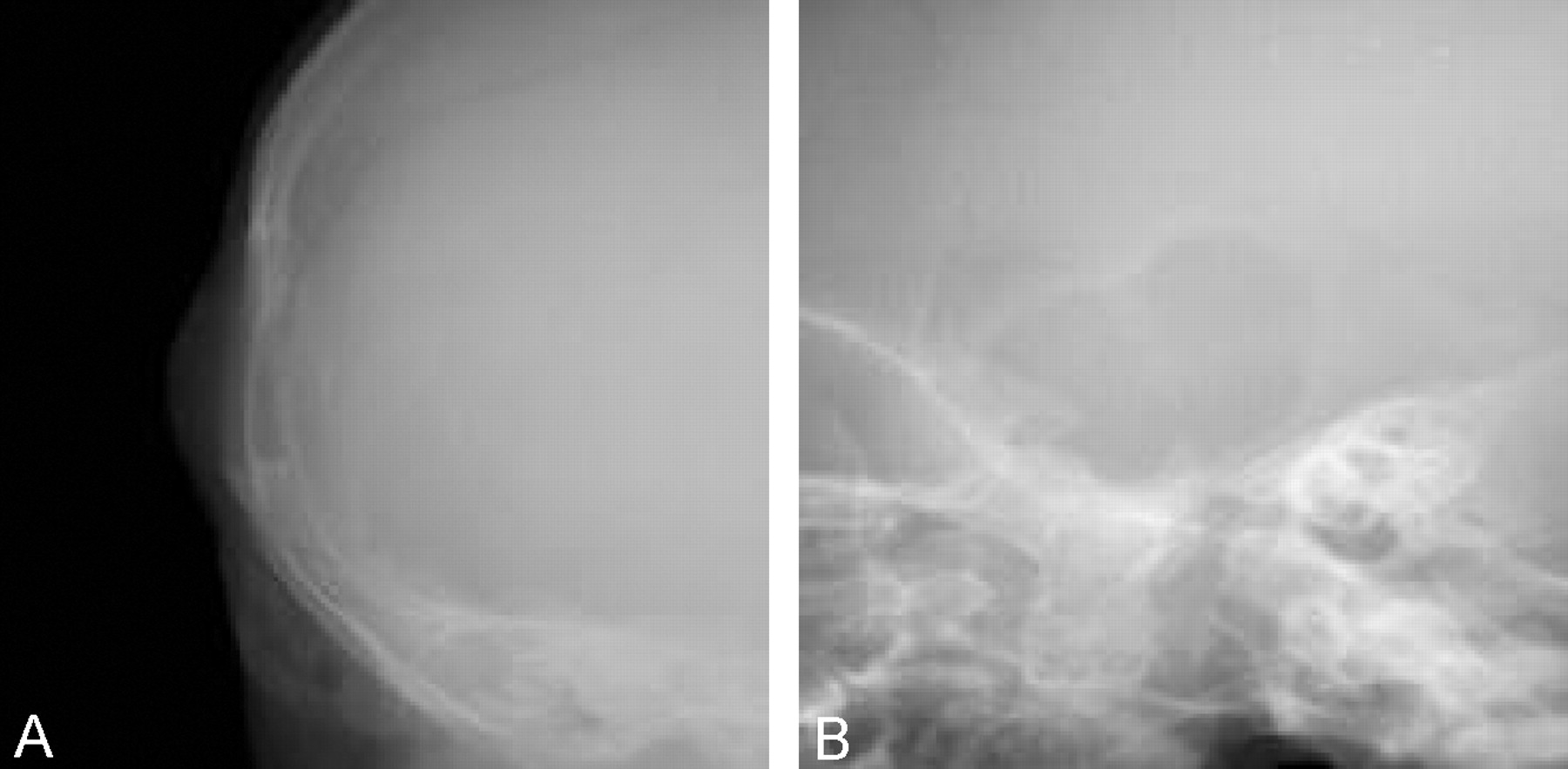
Frontal (A) and lateral (B) conventional radiographs of the skull, demonstrating cranial fasciitis of the skull as a single lytic defect in the temporal region with associated soft tissue swelling of the overlying scalp. The lesion has a narrow zone of transition, and there is no periosteal new bone formation. There are no other bony lesions in the remainder of the axial or appendicular skeleton.
Axial CT examination of the brain was then performed. This revealed a single 1.5 × 2.5-cm lesion in the right parietotemporal skull, which was centered in the intradiploic space and extradural in location (Fig 2A and B). No significant mass effect was demonstrated. The lesion enhanced after administration of intravenous contrast material.

Axial CT images (A and B) of the head, demonstrating cranial fasciitis of the skull as a soft tissue mass centered in the calvarium. There is destruction of the inner and outer tables of the skull. The mass is extraaxial.
A subsequent MR image showed that the lesion destroyed both the inner and outer tables of the skull, was well defined, and demonstrated homogeneous contrast enhancement. The lesion was heterogeneous in signal intensity on T2-weighted images (Fig 3A). It showed no diffusion restriction on diffusion-weighted images, and it was isointense to gray matter on T1-weighted images (Fig 3B and C). There was also associated dural thickening and enhancement (Fig 3D). The remainder of the examination was unremarkable.

Axial T2-weighted (4780/100 [TR/TE]) (A), diffusion-weighted (b value = 1000, 5100/137 [TR/TE]) (B), and pre- (C), and postcontrast (D) T1-weighted (500/12 [TR/TE]) MR images of the brain, demonstrating cranial fasciitis of the skull as a solitary, homogeneously enhancing, extraaxial soft tissue mass centered in the calvarium. The lesion demonstrates heterogeneous T2 signal intensity, no restriction of diffusion on diffusion-weighted image, and signal intensity that is isointense to gray matter on the precontrast T1-weighted image. The postcontrast image shows enhancement of the underlying dura. There is no involvement of the underlying brain.
A neurosurgical consult was obtained. At surgical resection, the lesion was noted to be intracalvarial, confirming imaging findings. It was purplish in color and soft, and it bled vigorously when incised. It was easily dissected from the calvaria and dura and was removed in a piecemeal fashion in toto.
At histologic analysis, the mass was found to be composed of proliferations of loose to compact fibroblasts and myofibroblasts. These were arranged in fascicles and storiform patterns in a variably collagenized to myxoid stroma. Osseous metaplasia was noted, and there were osteoclastlike giant cells present as well as hemorrhagic elements. These findings were most compatible with a diagnosis of nodular fasciitis or cranial fasciitis.
Discussion
Cranial fasciitis is a benign fibroblastic proliferation of the scalp that was first described as a subset of nodular fasciitis in a study of nine cases in 1980 by Lauer and Enzinger (1). Features distinguishing cranial fasciitis from nodular fasciitis include the usual age of incidence of the tumor and its location. It is an extremely rare tumor, with fewer than 40 cases reported in the literature. It occurs almost exclusively in children under the age of 6 years but has been reported in at least one adult (2). The median age of presentation is approximately 21 months, and at least one case occurring in a neonate has been described (3). Male patients are affected twice as frequently as female patients (1). No definite predisposing factors have been identified; however, many reports cite prior trauma to the affected area as playing a possible role in later development of cranial fasciitis (1, 4–7). A familial predisposition has also been suggested, although this has not been proved (7).
The lesions are characteristically rapidly growing with a median size at presentation of approximately 2.5 cm, although they may attain a size as large as 15 cm (8). In most cases, the lesion arises from the deep fascia of the scalp and erodes into the underlying calvaria; however, a single case of purely intracranial cranial fasciitis has been reported (6). The lesions are usually single, although one case of two synchronous tumors has been reported (7). The parietotemporal regions are most commonly affected (1).
Clinically, patients usually present with a history of a rapidly growing scalp mass that is firm and nontender. When present, other symptoms are usually secondary to mass effect and have included proptosis, diplopia, facial nerve palsies, deafness, and hemiparesis (3, 6, 9, 10, 11). Surgical excision is the definitive therapy for these lesions. Reports have shown that, even after incomplete surgical excision, the lesions tend to regress over time and do not recur (7, 11).
Imaging features usually include a single lytic skull lesion, which is well defined with an accompanying enhancing soft tissue mass seen on CT or MR images. The lytic calvarial defect may have a thin sclerotic margin, although aggressive-appearing periosteal new bone formation can be seen as well. Calcification within the soft tissue mass can be seen. Erosion of the outer table of the skull is most common, although extension through the inner table and involvement of the dura has been seen in approximately one third of reported cases. The soft tissue mass seen on CT or MR images is usually mildly inhomogeneous and demonstrates marked enhancement. On CT images, it can appear slightly hyperattenuated relative to gray matter. On MR images, the lesion can appear isointense relative to gray matter on both T1- and T2-weighted images. Our single case demonstrated no evidence of restricted diffusion on diffusion-weighted images.
The radiologic differential diagnosis for a lytic skull lesion includes multiple pathologic entities such as eosinophilic granuloma, juvenile fibromatosis, juvenile fibrosarcoma, primary bone neoplasms, hemangioma, epidermoid cyst, metastasis, syphilis, sarcoidosis, tuberculosis, and leptomeningeal cysts. Cross-sectional imaging with CT or MR may help distinguish between many of these entities and cranial fasciitis; however, the diagnosis of cranial fasciitis is primarily a histologic one. Microscopy will demonstrate loose proliferations of fibroblasts or myofibroblasts that may be arranged in loosely bound fascicles in a collagenous or myxoid matrix (12).
Conclusion
Our case typifies the usual clinical and radiologic presentation of cranial fasciitis: a male infant presented with a 2-month history of a painless but rapidly expanding parietotemporal scalp mass, which CT and MR imaging demonstrated to be an enhancing soft tissue mass that eroded through the skull and involved the dura. Surgical excision was curative.
The significance of cranial fasciitis to a radiologist is that it can mimic the appearance of more aggressive entities such as eosinophilic granuloma and malignant neoplasms. Although cranial fasciitis is quite rare, it should be considered in the differential diagnosis for lytic skull lesions in patients whose age and clinical presentation suggest this possibility.
References
- Received November 8, 2002.
- Accepted after revision December 18, 2002.
- Copyright © American Society of Neuroradiology









{kind=link}
{kind=link}
{kind=link}