
Abstract
Summary: A 6-year-old girl was admitted for transoral penetrating injury by a half-split chopstick. Subsequent CT imaging examinations showed that the chopstick had passed between the basion and the dens and reached the subarachnoid space just at the medulla oblongata. A sagittal reconstructed CT scan was useful for the evaluation of the injury. Imaging findings and their clinical relevance are discussed.
Craniocerebral penetrating injury by a half-split chopstick sometimes occurs in Japan (1–6), especially in children (1–5). We describe a patient with transoral penetrating injury by a half-split chopstick, passing between the basion and the dens. To our knowledge, this type of penetrating injury had not been reported in the literature.
Case Report
While eating cotton candy, the patient, a 6-year-old girl, fell with a half-split chopstick in her mouth. On admission to the emergency department of our hospital, she had no neurologic deficits. The half-split chopstick was fixed tightly, penetrating the soft palate. We performed CT immediately without sedation. CT scans were obtained at a voltage of 120 kV, a tube current of 300 mA, 0.5 s per rotation, a detector row beam collimation of 1 mm, helical pitch of 3.5, and a field of view of 21.75 cm by using a multidetector helical CT scanner (Aquilion Multi; Toshiba Medical, Tokyo, Japan). The chopstick was fixed with a string, to prevent migration. The CT scan setting with the bone window demonstrated the chopstick as a low-attenuation area in the nasopharyngeal wall and, moreover, in front of the medulla oblongata (Fig 1). Obvious intracranial hemorrhage was not observed.
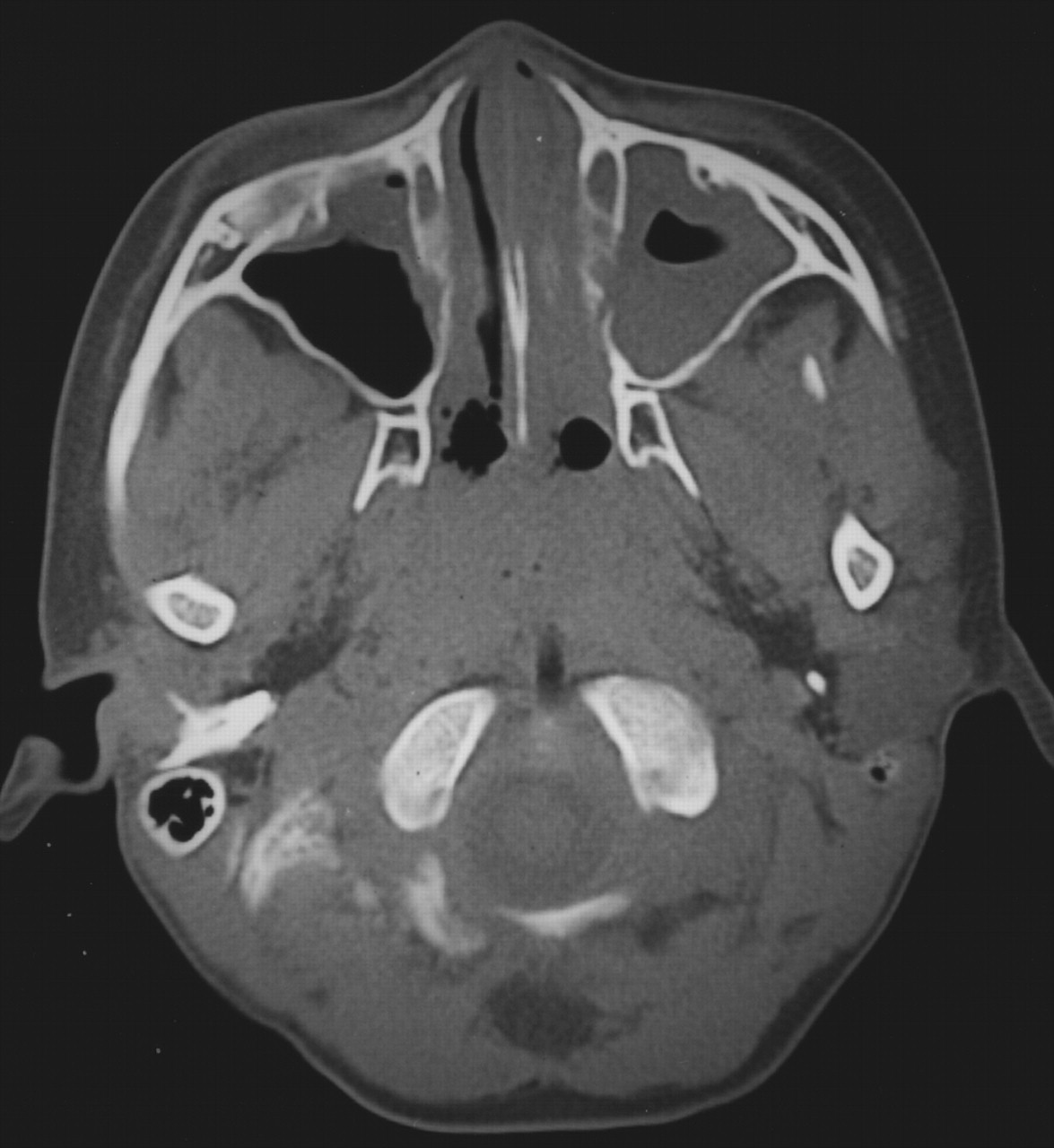
CT scan with the bone window setting demonstrating the chopstick as a low-attenuation area in the nasopharyngeal wall and in front of the medulla oblongata.
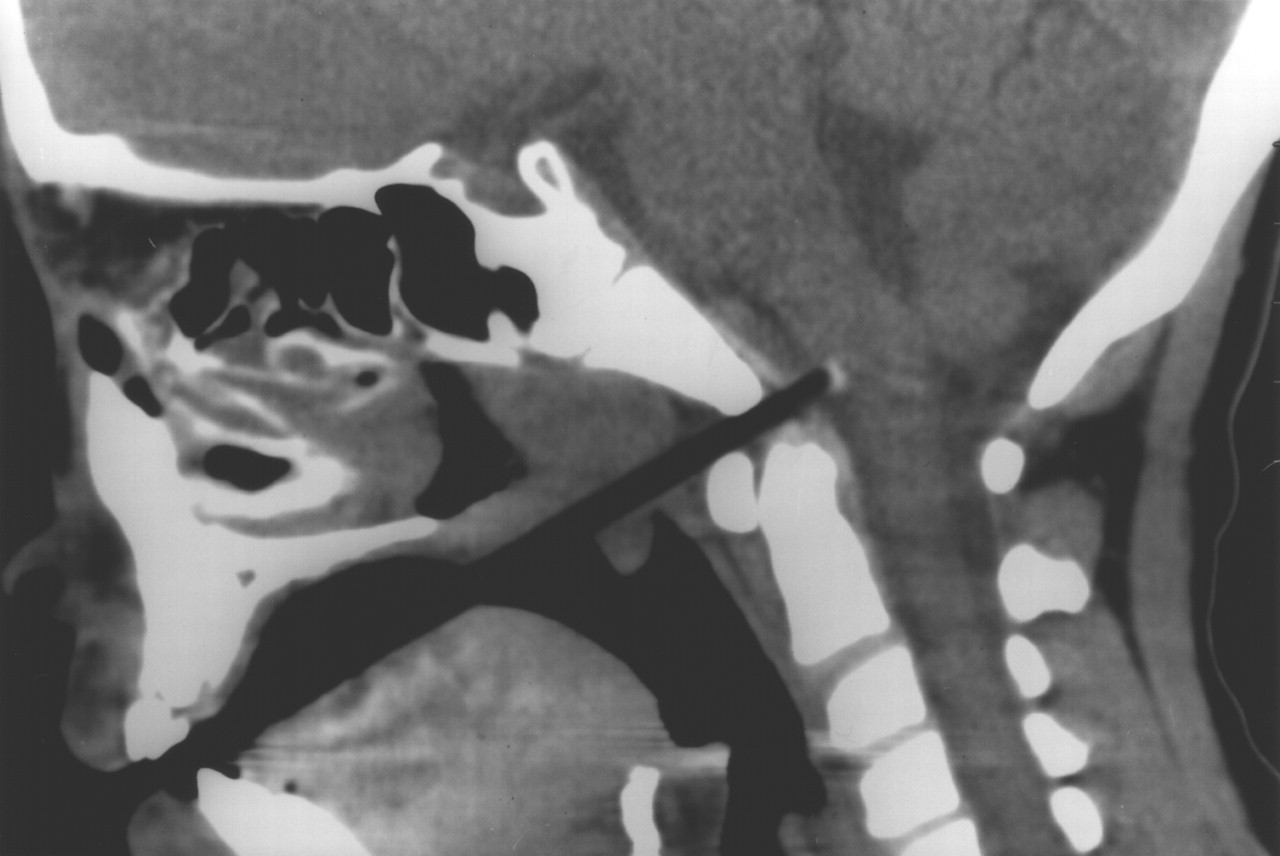
Reconstructed sagittal CT images revealed the accurate localization of the chopstick (Fig 2). The half-split chopstick penetrated into the soft palate just above the uvula to the nasopharyngeal space and tore the upper pharyngeal wall between the basion and the dens and then reached the subarachnoid space at the medulla oblongata. After CT was performed, the patient began to cry and move her head and mouth. We then decided to remove the chopstick without further examinations, because of the risk of injury to the brain stem.

Reconstructed CT scan revealing a clear image of the half-split chopstick as low-attenuation line, which penetrated into the soft palate just above the uvula, through the nasopharyngeal space, into the upper pharyngeal wall between the basion and the dens, and then reached the subarachnoid space at the medulla oblongata.
Emergent surgery was performed via a transoral approach under general anesthesia. Preoperatively, we did not evaluate vascular injury. Because the top of a half-split chopstick was blunt (ie, 5 mm × 5 mm) and no hemorrhaging was apparent around the tip of the chopstick, it was unlikely that penetration would result in direct vascular injury. Moreover, there could be no major artery at the midline of the lower part of the medulla oblongata, where the top of chopstick reached. If it had been necessary, however, microscopic surgical intervention would have been performed.
During the operation, the half-split chopstick was fixed firmly, and strong force was needed to remove it manually. CSF and a small amount of blood were noted after its removal, but their leakage stopped with compression alone. The posterior pharyngeal mucous membrane was then closed with two stitches of absorbable suture. Intravenous antibiotic therapy was administered to prevent postoperative bacterial meningitis. A subsequent lumbar puncture demonstrated mild bacterial meningitis, but the patient was discharged 3 weeks after her injury free of infection or CSF leakage. On discharge, she wore a soft neck collar for immobilization. Her neck was stable, with dynamic study demonstrating no abnormal movement of the dens.
Discussion
In the literature, craniocerebral penetrating injury in childhood consisted of stab wounds, encountered as accidental injuries by pencils (7), screwdrivers (5), sewing needles (5, 8), chopsticks (1–5), knives (9), scissors (10), and so on. Whenever children hold objects in their mouths, oral injury is likely. In our case, an unusual transoral penetration between the basion and the dens occurred. To the best of our knowledge, the literature contains no reports of this type of injury.
Because of the porosity of the wood, a dry chopstick contains a considerable amount of air. As such, a CT scan shows it as a low-attenuation structure. Once water is absorbed from surrounding tissues, its attenuation could be changed (1–3), resulting in misdiagnosis. If small foreign bodies migrate into soft tissues, still greater attention is needed. In such a case, MR imaging should be performed. In the case of our patient, the reconstructed sagittal image provided us with a clear picture as the low-attenuation line, which demonstrated accurate localization of the half-split chopstick that penetrated the dura in front of the medulla oblongata.
Preoperatively, we supposed that major vascular injury had not occurred. First, the top of a half-split chopstick was obtuse and blunt, so direct injury to the vessel was unlikely. Second, there could not be basilar artery at the medulla oblongata at the position of the chopstick. Third, the patient had no neurologic deficits, which indicated that major vessels were not damaged. In fact, intraoperatively, a small amount of blood was observed after its removal, but further bleeding did not occur. Postoperatively, she recovered well without major complications.
In this case, the reconstructed sagittal CT image gave us a great deal of useful information about the accurate location of the chopstick and, consequently, aided in treatment.
- Received May 21, 2003.
- Accepted after revision August 23, 2003.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.