
Abstract
Summary: Intra-arterial Doppler sonography may complement arteriography by providing immediate physiological evidence of hemodynamic adequacy and by obviating unnecessary angioplastic dilation. We used a Doppler-tipped guidewire in 16 patients and obtained velocity measurements at the site of stenosis immediately before and after carotid artery stenting (CAS) in 10 patients. Intra-arterial Doppler sonography confirmed hemodynamic improvement immediately after stent placement and correlated well with post-CAS duplex Doppler sonography results. Thus, intra-arterial Doppler sonography can be feasibly incorporated into CAS procedures for hemodynamic evaluation and can provide anatomic information that complements information provided by angiography.
Although intra-arterial Doppler-tipped guidewires have been found to be accurate in measuring intra-arterial blood flow velocities in extra- and intracranial arteries and veins, the clinical application of Doppler guidewires in neuroradiology has been limited to only a few studies (1–4).
Carotid artery stenting (CAS) requires arteriography for immediate anatomic evaluation of the adequacy of dilation obtained after stenting but does not provide physiological measures of the resultant improvement in blood flow velocities (5). Reliance on an anatomic measure alone of CAS adequacy may result in dilation without adequate improvement in cerebral hemodynamics. Prolonged or excessive balloon inflation has been associated with cerebral hypoperfusion from luminal compromise, plaque dislodgment, and intimal dissection (6).
Use of a Doppler-tipped guidewire as a means of evaluating blood flow velocities during the stent placement procedure may obviate unnecessary angioplastic dilation or provide physiological evidence of hemodynamic adequacy. Our goal was to determine whether the Doppler-tipped guidewire can safely be used for immediate evaluation of CAS and to evaluate the relationship between blood flow velocities as measured with intra-arterial and duplex Doppler sonography and the degree of stenosis estimated on the basis of angiographic studies.
Methods
The intra-arterial system used consists of a 0.014-inchDoppler-tipped guidewire (Flowire; Cardiometrics, Mountain View, CA) with a piezoelectric transducer operating at 12 MHz mounted at its distal end. The proximal end of the wire is connected to a spectral wave analyzer that displays the pulsed Doppler signal.
Sixteen patients (nine men and seven women) with symptomatic carotid stenosis shown by an external duplex color Doppler device were examined. When the symptomatic stenotic vessel was entered by using the regular femoral approach, an angiographic study was performed, and the Flowire was navigated in the catheter to the site of the stenosis. Blood flow velocities were recorded proximal to, distal to, and at the level of stenosis. After angioplasty and stent placement, the Flowire was reinserted to obtain flow measurements at the level of stenosis. Patients underwent color and spectral Doppler sonography 24 hours, 1 month, 3 months, 6 months, and 1 year after the stent placement procedure.
Percentage of pre- and post-stent stenosis as seen on the angiograms were estimated during the procedure and confirmed by using the North American Symptomatic Carotid Endarterectomy Trial method after the procedure (6, 14), specifically by using the following equation: % = [1 − (dstenosis / dnormal)] × 100, where dstenosis = diameter of the internal carotid artery at the site of the most severe stenosis and dnormal = diameter of the proximal normal common artery. The same approach was used for post-stent measurements, for which the numerator was the diameter of the stent at the internal carotid artery that was judged to be the smallest. The measurements were obtained 90 degrees to the arterial wall. Measurements were obtained on three separate occasions by using three separate images of the same vessels. The average of the three results was calculated. All measurements were made by the primary author (N.G.).
Results
Full data are presented in tabulated form (Table). For four of 16 patients, it was not possible to advance the Doppler-tipped guidewire past the level of the stenosis, and velocity measurements could not be obtained with that system. In one patient, the angioplasty procedure was not performed because of induction of a severe vasovagal response. In the remaining patient, the immediate pre- and post-stent peak systolic velocities were recorded by using the intra-arterial Doppler-tipped guidewire system.
Pre- and post-stent angiography, intra-arterial Doppler ultrasonography, and duplex Doppler ultrasonography data
The pre-stent peak systolic velocities obtained by using the intra-arterial Doppler-tipped guidewire system were markedly greater compared with the peak systolic velocities obtained after stent placement, with an average difference of approximately 120 cm/s. This difference suggests that the stent placement procedure resulted in significant relief of stenosis and recuperation of blood flow. Similarly, pre-stent measurement of peak systolic velocities were recorded by using conventional duplex Doppler sonography on the same day of the procedure in eight patients; in 14 patients, same-day post-stent duplex Doppler peak systolic velocities were recorded. As with the intra-arterial Doppler-tipped guidewire system, the pre-stent velocities recorded by using duplex Doppler sonography were significantly greater than those recorded after the stent placement procedure (average pre-stent/post-stent difference of 204 cm/s). When comparing the intra-arterial Doppler-tipped guidewire system and duplex Doppler sonography results, good correlation was observed between peak systolic velocity measurements obtained after stent placement (r = 0.70; P < = .01). Both methods show resolution of peak systolic velocities to “normal” values in nine patients (56%) after stent placement (Table, Fig 2).

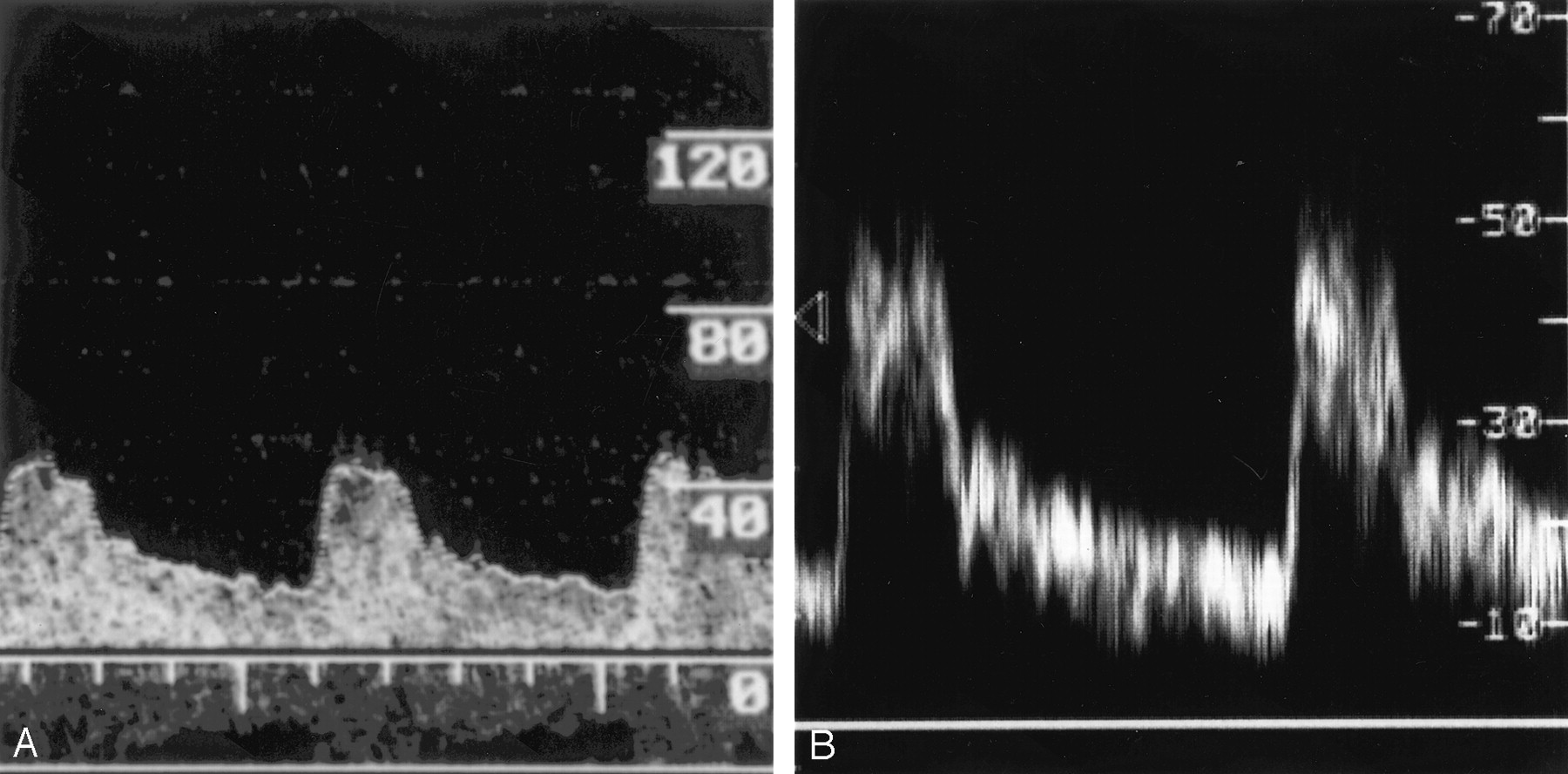
Examples of Doppler spectra. Velocities are measured in cm/s.
A, Intra-arterial Doppler-tipped guidewire spectra obtained immediately before the stent placement procedure.
B, Duplex color Doppler sonography spectra obtained 2 hours before stent placement.

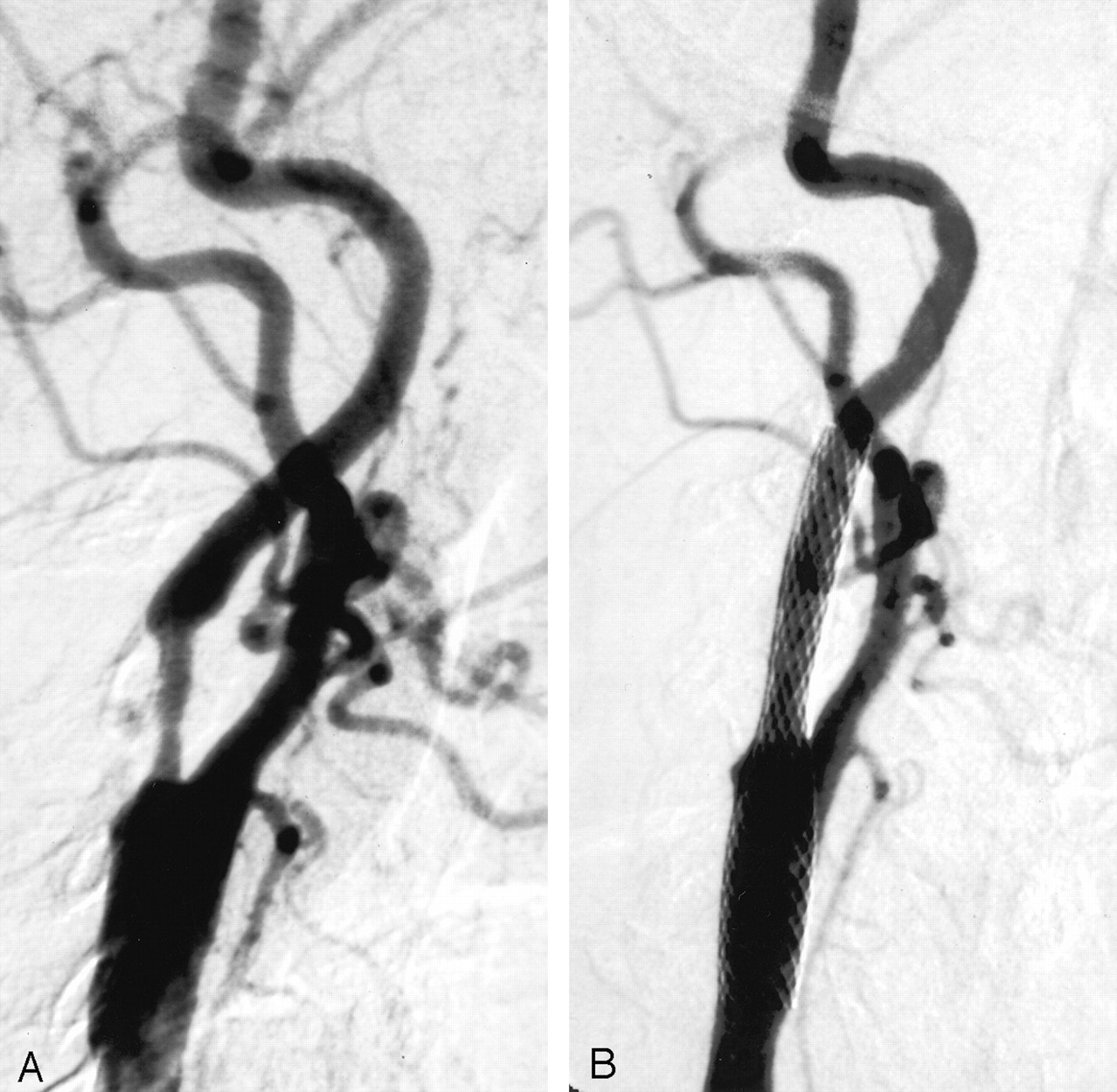
Angiograms of the patient whose spectra are shown in Figure 1.
A, Before angioplasty of >80% stenosis of the right carotid artery.
B, After the procedure, successful angioplasty and stent placement can be seen.
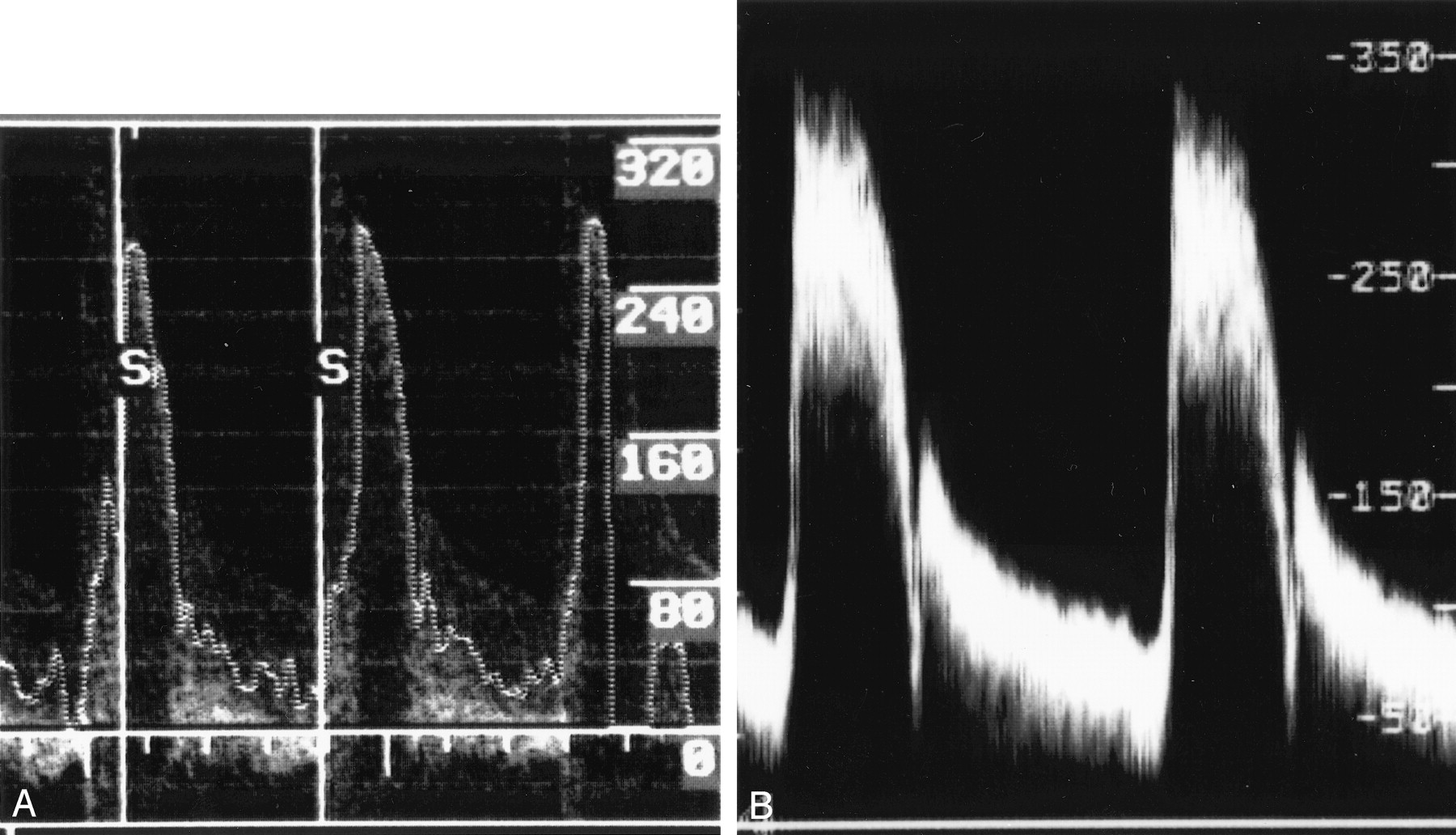
Examples of Doppler spectra. Velocities are measured in cm/s.
A, Intra-arterial Doppler-tipped guidewire spectra obtained immediately after the stent placement procedure.
B, Duplex color Doppler sonography spectra obtained 2 hours after stent placement.
Angiograms of the patient whose spectra are shown in Figure 3.
A, Before angioplasty of >80% stenosis of the right carotid artery.
B, After the procedure, successful angioplasty and stent placement can be seen.
For the 10 CAS procedures for which intra-arterial Doppler peak systolic velocity measurements were obtained, several angiographic studies were conducted both immediately before and immediately after the CAS procedures (Table, Patients 1, 3, 5, 8, 10, 11, 13, 14, 15, and 16). In all 10 cases, the post-stent angiographic results indicated resolution of stenosis to moderate (30–69%) or low (<30%) grade levels after the angioplasty and stent placement procedure. [However, below approximately 54% stenosis achieved after stent placement, peak systolic velocities achieved by using the intra-arterial Doppler-tipped guidewire system and duplex Doppler sonography did not improve considerably.] For example, the intra-arterial Doppler-tipped guidewire system peak systolic velocity values for patients 3, 4, 5, 6, 8, 11, and 16 were all between 60 and 80 cm/s, even though post-CAS stenosis values were 54%, 33%, 27%, 54%, 20%, 43%, and 53%, respectively. Furthermore, peak systolic velocities remained above 100 cm/s in patients 1, 13, and 15 even though measured percent stenosis achieved in these patients was below 54%. This observation suggests that dilation of the stent above a certain point does not result in any significant increase in blood flow. No neurologic complications occurred during the procedures.
Discussion
Patients with unstable angina and those with contralateral carotid artery occlusion, restenosis, or radiation-induced stenosis represent specific patient populations for whom CAS offers a potential alternative to carotid endarterectomy (11, 12). Doppler guidewire-measured intravascular blood flow velocities after CAS have been shown to closely correspond with velocities obtained by using external duplex Doppler sonography in both animal models (1, 2) and preliminary studies of patients undergoing endovascular carotid angioplasty (3). The intra-arterial Doppler-tipped guidewire system offers the advantage of intraprocedural physiological measurements, and therefore the opportunity to make any hemodynamically based adjustments during the procedure. In addition, the system is less affected by inaccuracies introduced as a result of interference of sonographic penetration by endovascular prostheses such as stents (13).
Our results show that the intra-arterial Doppler-tipped guidewire system can be used for immediate evaluation of angioplasty and stent placement of stenotic carotid arteries. Pre-stent peak systolic velocity measurements at the tightest stenosis could be obtained in all except four patients for whom the extent of stenosis precluded the advancement of the Doppler-tipped guidewire past the stenosis. As expected, peak systolic velocities at the tightest level of stenosis decreased significantly with angioplasty and stent placement in all patients. The system thus provided real-time physiological confirmation of recuperation of blood flow after stent placement.
As assessed by the intra-arterial Doppler-tipped guidewire system, 10 patients attained velocities within normal ranges for adequate blood flow. Among these same patients, however, the degree of post-stent dilation achieved as assessed by using post-stent angiography resulted in stenoses ranging from 20% (low grade) to 54% (moderate grade). These results indicate that below a certain level of stenosis, no clinically significant improvement occurs in blood flow. Thus, below approximately 50% stenosis, it may be unnecessary to dilate as long as peak systolic velocity has decreased to normal levels. Despite the wide range of angiographic results for these patients, no difference in the rates of neurologic complications occurred after stent placement. These results provided some insight into the observation that no benefit has been shown of procedures such as carotid endarterectomy for patients with stenosis of <50% (12). That is, below this level of stenosis, blood flow is sufficient to avoid neurologic sequelae.
Ringer et al (11) and Yoshida et al (13) showed that the use of carotid duplex Doppler sonography for follow-up of carotid arteries may be less reliable after stent placement than before stent placement. Altered arterial wall compliance or stent interference with Doppler signaling may reduce the accuracy of Doppler sonography after stent placement, resulting in a significant number of falsely positive stenoses (11). The intra-arterial Doppler-tipped guidewire system may be less subject to the effects of signal interference caused by stent placement, because the Doppler-tipped guidewire is in direct contact with blood. This may be reflected in the generally lower post-stent peak systolic velocity values obtained by using the system (Table) and may indicate a way of reducing false-positive results after stent placement.
Further studies need to be conducted on a greater sample size to accurately assess the validity of the intra-arterial Doppler-tipped guidewire system for evaluation of CAS success. Importantly, it must be established whether a threshold peak systolic velocity range exists as measured by the system, below which one can reliably predict no further benefit from dilation at the level of stenosis. The importance of improvement in blood flow velocities before and after stent placement compared with absolute blood flow velocities also must be determined. If improvement is more important, the use of the intra-arterial Doppler-tipped guidewire system may be limited to cases in which the degree of pre-stent stenosis does not preclude advancement of the Doppler-tipped guidewire.
Conclusion
On the basis of our preliminary results, we find that the intra-arterial Doppler-tipped guidewire system is a feasible method of evaluating the immediate results of CAS. Except when near-occlusive stenosis precludes the advancement of the Doppler-tipped guidewire, the technique is easily incorporated during the CAS procedure and adds minimal time and no complications. Although more experience is needed, a reasonable correlation seems to exist between post-stent peak systolic velocity levels as measured by the intra-arterial Doppler-tipped guidewire system and those measured by duplex Doppler sonography. The intra-arterial Doppler-tipped guidewire system can therefore be useful in showing the adequacy blood flow velocities achieved by the stent placement procedure. The system may in turn help circumvent unnecessary, potentially harmful over-dilation during the CAS procedure. The generally lower peak systolic velocities shown by the intra-arterial Doppler-tipped guidewire system, as compared with duplex Doppler sonography, may indicate that the system is less subject to sonographic interference produced by the stent. The intra-arterial Doppler-tipped guidewire system is limited in that it may be difficult to advance the Doppler-tipped guidewire past levels of tight stenosis. This may have important implications if relative improvement in peak systolic velocities is more indicative of successful CAS than the final post-stent peak systolic velocity value. More research is needed to determine the prognostic importance of physiological measurements obtained by using the system versus the anatomic measurements obtained by using post-procedural angiography.
References
- Received August 11, 2003.
- Accepted after revision January 5, 2004.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.