
Abstract
Summary: We describe a case of cerebral vasculitis seen on angiography in a patient with a history of non-Hodgkin lymphoma and graft-versus-host disease (GVHD) 2 years after match-related bone-marrow transplant. The vasculitis was ascribed to GVHD as other causes were excluded by laboratory tests. Other recent reports of GVHD-related vasculitis have been published, but none with angiographic changes.
After bone-marrow transplant patients are at known risk for multiple systemic and neurologic complications, primarily due to the immunosuppression, including opportunistic infections, drug toxicity, and immune-related processes such as graft-versus-host disease (GVHD) and lymphoma. CNS infections, neurotoxicity from cyclosporine, and stroke are not uncommon, particularly in the acute posttransplant period. As more patients are surviving longer following bone-marrow transplant, other complications are being recognized. We present a case of cerebral vasculitis demonstrated on angiography in a patient with several relapses of chronic GVHD, which we believe to be the cause of the vasculitis. Other authors have reported cases of cerebral vasculitis secondary to chronic GVHD, but none demonstrated vasculitis on angiography (1–3).
Case Report
A 55-year-old female patient with a history of non-Hodgkin lymphoma presented to an outside hospital with onset of headache, dizziness, and progressive ataxia. Cranial CT performed at that time showed an acute intraparenchymal hemorrhage in the left cerebellum. Cerebral angiography was performed, showing an aneurysm of the left posterior inferior cerebellar artery (PICA) that was thought to be the source of hemorrhage.
The patient was transferred to our institution, where 23 months prior she had undergone a match-related allogeneic bone-marrow transplant for recurrent lymphoma. Her posttransplant course was complicated by acute GVHD of the skin, gastrointestinal tract (biopsy proven), and liver, which was treated with cyclosporine and prednisone for approximately 1 year. Immunosuppressants were tapered over the year, with episodes of diarrhea and recurrence of the skin rash. Eighteen months after transplant, the patient developed dyspnea, wheezing, and a persistent cough. Bronchoscopy showed inflammatory cells in the bronchial washings, and GVHD of the lungs was suspected but not confirmed. Six weeks before the cerebellar hemorrhage, she developed vasculitis of the digits presenting as blue fingertips. Complete workup at that time for infectious causes including cytomegalovirus, toxoplasma, and cryptococcus were negative. Further, the sedimentation rate, C-reactive protein, and thrombophilia screen were also normal or negative.
A repeat angiogram was performed 3 weeks after the initial hemorrhage and showed an aneurysm of the left PICA with hemorrhage in the left cerebellum (Fig 1). Also, there were multiple segments of abnormally dilated branches of the arteries of the posterior fossa, as well as the left posterior cerebral artery, which suggests the diagnosis of vasculitis. Vasospasm was not thought to be the likely etiology because the segments of vessels appeared distended beyond their expected normal caliber. Furthermore, these findings had been evident in a less-prominent degree on the initial angiogram 3 weeks earlier. MR imaging of the brain showed the left cerebellar hemorrhage with mildly increased T2 signal intensity in the periventricular white matter (Fig 2).

Anteroposterior (A) and lateral (B) images of left vertebral artery injection show small aneurysm off the left PICA and multiple abnormally dilated segments consistent with vasculitis.
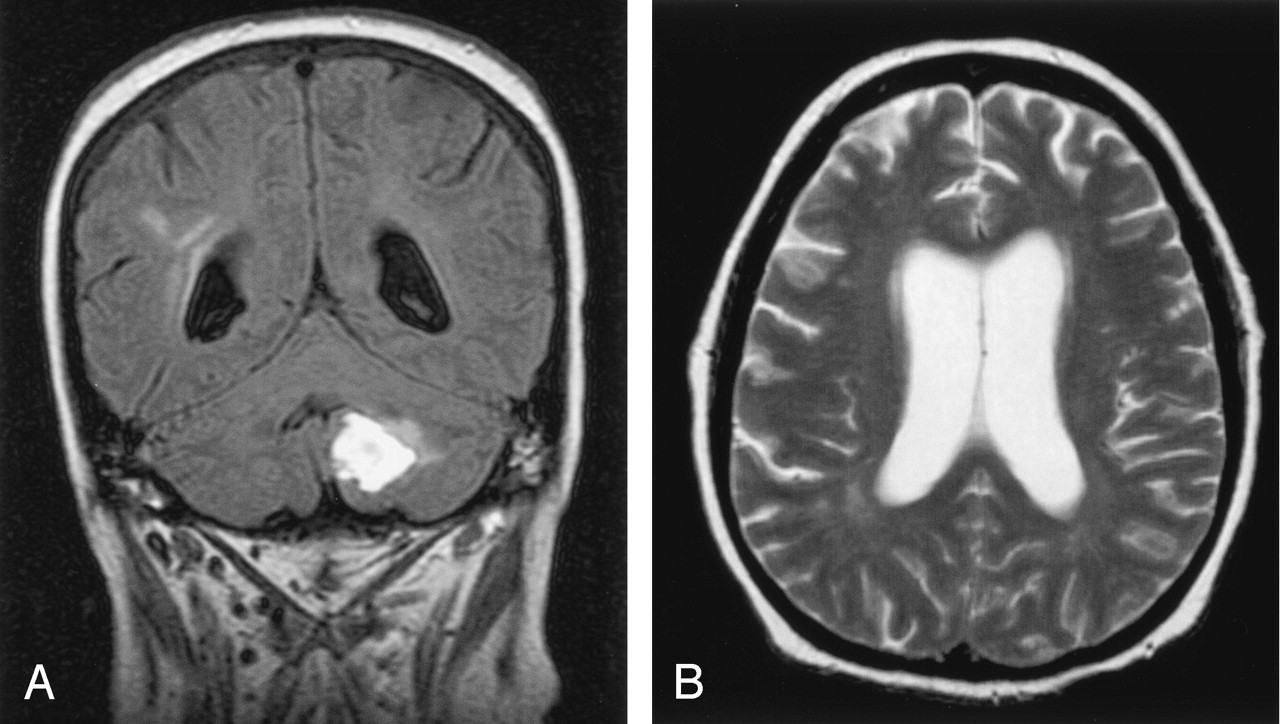
A, Coronal fluid-attenuated inversion recovery image shows the left cerebellar parenchymal hemorrhage and mild increased signal intensity in the periventricular white matter. B, Axial T2-weighted image also showing areas of increased T2 signal intensity in the white matter, especially near the posterior horns of the lateral ventricles.
GVHD was the presumed cause of the vasculitis of the cerebral arteries and fingers, and the patient began immunosuppressive therapy. Tacrolimus was chosen for its ability to cross the blood-brain barrier. Neurosurgical consultation recommended conservative management of the hemorrhage and left PICA aneurysm. After several days of treatment with tacrolimus, her gait disturbance decreased, her headaches declined, and she was discharged home.
Discussion
Following bone-marrow transplant, patients are known to be at risk for developing multiple neurologic complications, including metabolic encephalopathy, CNS infections, stroke, neurotoxicity to immunosuppressant drugs such as cyclosporine, and seizures (4, 5). These complications are more typically seen in the early period following transplant. Over the past decade, bone-marrow transplant patients have demonstrated increased survival time, leading to some chronic conditions such as GVHD.
Chronic GVHD occurs in 30–50% of transplant patients from related donors and at least 60–70% from unrelated donors (6). Clinical manifestations most commonly involve the skin, gastrointestinal tract, and liver, but all organ systems are at risk (7). Neurologic manifestations typically involve peripheral neuropathy and myasthenia gravis (4, 8). More recent reports in the literature have described patients developing an angiitis-like syndrome of the CNS as a manifestation of chronic GVHD (1–3).
Our patient initially developed the typical manifestations of GVHD with involvement of the skin, gastrointestinal tract, and liver. Approximately 2 years after her transplant, she developed a left cerebellar parenchymal hemorrhage. MR imaging of the brain showed the parenchymal bleed, some mild atrophy, and nonspecific increased T2 signal intensity in the periventricular white matter (Fig 2). Cerebral angiography showed a 3-mm aneurysm arising from the left PICA, the likely source of hemorrhage. Furthermore, there were classic manifestations (Fig 1) of cerebral vasculitis with dilated and narrowed segments in branches of the posterior circulation (9). A case report by Padovan et al (2) described two of five patients with chronic GVHD and a suspected or confirmed cerebral angiitis who developed parenchymal hemorrhages. All developed some abnormally increased T2 signal intensity in the white matter. One had autopsy-proved vasculitis, but none demonstrated classic appearance of vasculitis on angiogram, although there was a complete occlusion of the middle cerebral artery in one patient.
The precise cause for this patient’s vasculitis and aneurysm is not known. We suspect that the most likely cause is chronic GVHD, particularly in light of the development of telangiectasia of the finger tips just weeks before presenting with the cerebellar hemorrhage, as well as the history of GVHD following bone-marrow transplant. There are many known causes of cerebral vasculitis, including bacterial, viral, granulomatous, and other infections; collagen vascular diseases such as lupus and scleroderma; other auto immune processes; neoplasms, including intravascular lymphomatosis (also known as neoplastic angioendotheliosis, among other names). Most infectious causes of vasculitis were excluded in this patient by blood and CSF cultures. The patient did not have any other manifestations of granulomatous or collagen vascular disease. Intravascular neoplasms would have a rapidly progressive course, whereas this patient showed some slow steady improvement with the change in immunosuppressant therapy.
Several cases have now been published with high suspicion or confirmation of cerebral angiitis following bone-marrow transplant, but none with classic angiographic findings. Because patients survive longer after bone-marrow transplant, the possibility of vasculitis from chronic GVHD seems more possible and this diagnosis must be added to the list of potential neurologic complications.
References
- Received March 31, 2004.
- Accepted after revision June 15, 2004.
- Copyright © American Society of Neuroradiology








{kind=link}
{kind=link}