
Abstract
Summary: We describe radiologic findings of germinoma involving bilateral basal ganglia and cerebral white matter. In the early stage, T1-weighted MR images showed hyperintense areas in the bilateral globi pallidi. Later, T2-weighted images showed hyperintense areas involving bilateral white matter. The MR imaging findings reported here could help facilitate the early diagnosis of germ cell tumors in young patients.
Germinomas represent 0.5–2.1% of all intracranial tumors and usually arise in the pineal or suprasellar region (1). Germinomas arising from the basal ganglia and thalamus are much less frequent and are usually unilateral (1, 2). We describe an unusual case of germinoma involving bilateral basal ganglia and cerebral white matter.
Case Report
A previously healthy and developmentally normal 10-year-old boy developed dystonia with right dominance, weakness in the right leg, and dysarthria. MR examination was carried out on a 0.5T unit. T1-weighted image showed slightly hyperintense areas in the globi pallidi bilaterally, predominating in the left side (Fig 1). T2-weighted images showed small hyperintense areas in the left globus pallidus that were indistinguishable from perivascular space. Contrast-enhanced MR images were not obtained. The patient’s symptoms progressed slowly, and he developed right hemiparesis and mental retardation. Neurodegenerative or metabolic disease was suspected because of the bilateral nature of the findings. However, there was no family history of neurologic disorders, and the laboratory data did not support a diagnosis of metabolic disease. Two years after the onset of symptoms, the patient was admitted to our hospital. Neurologic examination demonstrated a right hemiparesis with hypereflexia, bilateral pyramidal tract signs, right facial nerve palsy, dysarthria, dystonia that was more prominent on the right side of the body, and mild mental retardation. Neuropsychological testing revealed reduced language function, distractibility, and cognitive decline. MR imaging examination was performed on a 1.5T unit. On T1-weighted images, the hyperintense areas in the bilateral globi pallidi had become more heterogeneous than during the previous examination. T2-weighted images showed hypointense areas with small hyperintense foci in the bilateral globi pallidi, diffuse hyperintense areas in the bilateral internal capsule, and surrounding cerebral white matter that was more extensive on the left side (Fig 2A). Postcontrast T1-weighted images showed tiny enhancement scattered in the left globus pallidus (Fig 2B). Postcontrast T1-weighted image in the sagittal plane through the sella-suprasellar region taken on another day showed there was no sella-suprasellar and pineal germinoma (Fig 2C). The MR images also showed marked atrophy of the left cerebral peduncle. Germ cell tumor of the basal ganglia was suspected. Tumor markers (alfa-fetoprotein and human chorionic gonadotropin) in the serum were within the normal range. Stereotactic biopsy of the left basal ganglia was conducted, and histologic examination of the specimen revealed a germinoma (Fig 3). The patient received four cycles of combination chemotherapy consisting of ifosfamide, cisplatin, and etoposide every 4 weeks, followed by radiation therapy for the whole brain (24 Gy/12 fraction). The patient’s neurologic deficits remained unchanged, and follow-up MR images demonstrated no recurrence after 5 years.

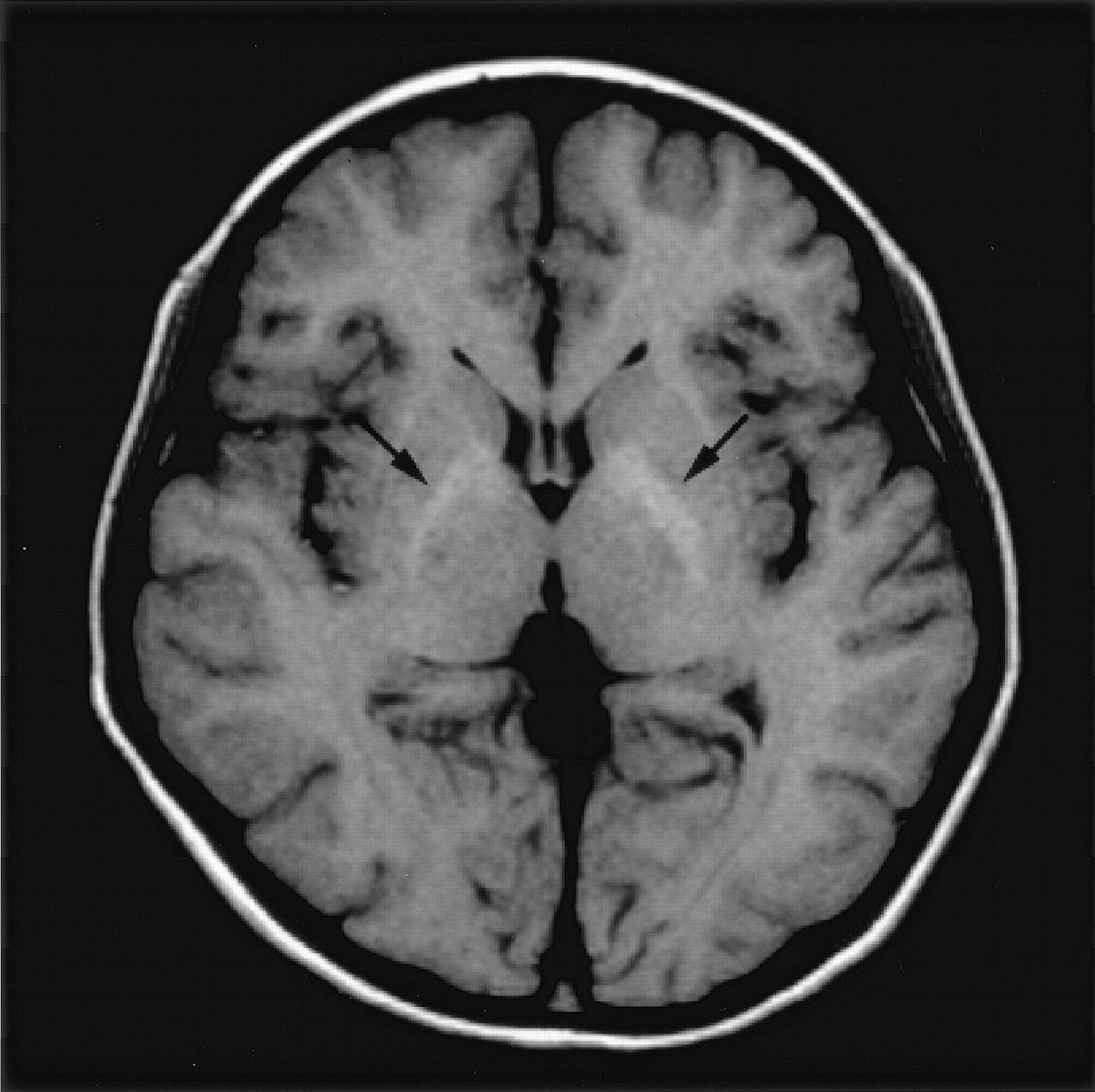
Axial 0.5T MR images obtained at the onset of the disease.
T1-weighted image (spin-echo 662/15 [TR/TE]) shows mild hyperintense areas in the globi pallidi bilaterally (arrows).

Axial and sagittal MR images obtained 2 years after the onset of disease on 1.5T unit.
A, T2-weighted image (spin-echo, 3000/90) shows hypointense areas with small hyperintense foci in the bilateral globi pallidi (arrowheads) and diffuse hyperintense areas in the bilateral internal capsule and surrounding cerebral white matter predominantly in the left side (arrows).
B, Postcontrast T1-weighted image (spin-echo, 600/15) shows tiny enhancement in the left globus pallidus (arrows).
C, Postcontrast T1-weighted image (spin-echo 600/15) in the sagittal plane taken on another day shows no abnormality in the sella/suprasellar and pineal region.

Histopathologic examination of a specimen obtained from left lentiform nucleus by stereotactic biopsy. Hematoxylin and eosin staining shows two different types of cells: large atypical cells containing large, round, vesicular nuclei with irregular and pleomorphic nucleoli (tumor cells), and infiltrating lymphocytes (original magnification, ×200). Placental alkaline phosphatase staining shows positive tumor cells (not shown).
Discussion
Germinomas are the most common of all germ cell tumors, a category that also includes embryonal cell carcinomas, endodermal sinus tumors, choriocarcinomas, teratomas, and mixed germ cell tumors (1). Although intracranial germ cell tumors usually arise from the pineal and suprasellar-sellar regions, as many as 14% of these tumors occur in the basal ganglia or thalamus. Germ cell tumors of the basal ganglia and thalamus are primarily found in patients between 7 and 20 years of age and show a striking (20:1) male predominance (1). Germ cell tumors arising in the basal ganglia or thalamus are usually unilateral. Patients with unilateral germ cell tumors of the basal ganglia or thalamus often present with hemiparesis, mental deterioration such as dementia or character change, precocious puperty, diabetes insipidus, oculomotor palsy, speech disturbance, or hemianopsia. The clinical course is usually slow, with the duration of clinical symptoms ranging from 1 month to 4.5 years (1).
At the time of diagnosis, most basal ganglionic germ cell tumors show an irregular solid area with contrast enhancement and variously sized cysts on CT and MR images (1, 2, 3–8). Mass effect and minimal surrounding edema usually accompany the tumors. Intratumoral hemorrhage is not uncommon on MR images (2, 4, 5). On CT scans, the solid area is usually iso- or hyperattenuated. Intratumoral calcification is frequently observed (1, 3–5, 7). In addition, CT and MR imaging findings of ipsilateral cerebral hemiatrophy or hemiatrophy of the brain stem are highly characteristic of germ cell tumors of the basal ganglia and thalamus. Ipsilateral cerebral hemiatrophy can be found in as many as 33% of these tumors (1, 2, 5, 7, 8). It has been proposed that ipsilateral cerebral hemiatrophy is due to antegrade (Wallerian) and retrograde degeneration of efferent and afferent fibers from the basal ganglia and thalamus caused by destruction and disappearance of ganglia cells and nerve fibers resulting from tumor invasion or due to tumor infiltration into internal capsule fibers with interruption of thalamocortical connections (1, 3, 5, 8).
Diagnosis of basal ganglionic germ cell tumors at an earlier stage has been difficult because of its rarity, nonspecific clinical features, and lack of mass lesions on CT and MR images. Tamaki et al (1) reviewed 40 cases of germ cell tumors of the basal ganglia in the literature together with their own two cases and reported that the duration of clinical symptoms was from 1 month to 4.5 years, with an average period of about 1.5 years. This indicates that the clinical course of this group of tumors usually progresses slowly and that early diagnosis is usually difficult. Because germ cell tumors are thought to arise from a midline streaming of totipotential cells very early in rostral neural tube development (3), they might be of prenatal origin, and their actual onset is probably far earlier than “the age at onset” (9). Such insidious onset before detection of mass lesion with imaging has also been reported in patients with sella-suprasellar germinoma presenting with diabetes insipidus (10). This insidious onset without mass lesion often results in delayed diagnosis.
To make a proper diagnosis earlier, it is mandatory to recognize early imaging findings of basal ganglionic germ cell tumors. In the early stage of basal ganglionic germ cell tumors, CT may not show any abnormality despite the presence of neurologic symptoms (3, 7). The early CT feature of germinomas of the basal ganglia CT has been described as an irregularly defined, homogeneous or inhomogeneous, isoattenuated to slightly hyperattenuated area without mass effect (5–7). Only a few MR imaging studies have been reported in the literature, and the tumors have tended to show no enhancement or only subtle enhancement on postcontrast T1-weighted images in the early stage (2, 5, 6). Okamoto et al (6) stated that high signal intensity on T1-weighted images and a small hyperintense lesion on T2-weighted images were seen in the basal ganglia in their two patients with germinoma and that these findings might be early MR imaging signs of basal ganglionic germinomas. Our T1- and T2-weighted images were similar to theirs. They also stated that the earliest and most characteristic MR imaging feature was atrophy of the basal ganglia, which was recognized before development of hemiparesis (6). By contrast, Kim et al (2) reported that they found low signal intensity on T1-weighted images and high signal intensity on T2-weighted images of the basal ganglia in two patients with small germinoma. Higano et al (5) reported that, in one patient with small basal ganglionic germinoma, T1-weighted images failed to show a definite abnormality and T2-weighted images showed an ill-defined hyperintense area that was difficult to differentiate from ischemic foci on the basis of MR imaging findings. These reports suggest that germ cell tumors of the basal ganglia infiltrate or destroy the brain parenchyma without forming apparent masses in the early stage. We speculate that the various signal intensity patterns result from different cell densities and amounts of tissue destruction among individual lesions.
Bilateral involvement of the basal ganglia by germinoma is extremely rare. We found only four cases of bilateral germ cell tumors of the basal ganglia with or without thalamic involvement in the literature, with the exception of recurrence after treatment (2, 3, 11).
Diagnosis of bilateral germinoma of the basal ganglia at an early stage is even more difficult than that of the unilateral one. Although the clinical course of our patient was nonspecific, it was typical for a germinoma occurring in the unilateral basal ganglia, except for the extrapyramidal signs. This is consistent with the previous case reports of bilateral germ cell tumors of the basal ganglia and thalamus in that the clinical features were bilateral or unilateral extrapyramidal signs, which occurred either simultaneously or sequentially to slowly progressing unilateral pyramidal signs (11). When we retrospectively evaluated the initial MR images of our patient, the subtle hyperintense areas on T1-weighted images in the globi pallidi were suggestive of early MR findings of basal ganglia germ cell tumors as reported by Okamoto et al (6). If it had localized unilaterally in the basal ganglia, it would have been possible to recognize it with MR imaging as early findings of basal ganglionic germ cell tumor. The CT findings of hyperattenuated areas in bilateral globi pallidi also concurred with early CT findings of germ cell tumors of the basal ganglia; however, the subtlety and bilateral nature of the lesion hampered the proper diagnosis in the early stage of the disease. The bilateral nature of the lesion suggested metabolic or neurodegenerative disease rather than neoplasm, although the lesion involvement was not completely symmetrical. The signal intensity patterns disclosed by 0.5T MR imaging and CT were similar to those of Hallervorden-Spatz disease at an early stage. The 1.5T MR imaging findings of hyperintense foci within hypointense globi pallidi on admission to our hospital also mimicked Hallervorden-Spatz disease. At that time, however, bilateral white matter involvement was observed, which did not fit this disease. Moreover, the patient’s clinical symptoms were relatively nonspecific, although his slowly progressing hemiparesis and mental retardation in addition to dystonia are distinct features of idiopathic torsion dystonia. The abnormal enhancement in left globus pallidus and atrophy of the ipsilateral cerebral peduncle suggested a germ cell tumor of the basal ganglia. We do not know exactly what the white matter lesion represents, because biopsy specimens were not obtained from the white matter. We speculate that the white matter lesion reflects tumor infiltration or Wallerian degeneration caused by the tumor, or both (5, 8). The unilateral atrophy of the cerebral peduncle might have been due to tumoral involvement of the internal capsule that was more extensive in the ipsilateral side than in the contralateral side (5).
Although germinomas respond readily to radiation therapy, conventional radiation therapy carries significant risks of neurologic sequelae in young patients. Because the chance of survival of patients with CNS germinoma is excellent, reduction of posttreatment sequelae and the preservation of neurocognitive function are of great concern (12). Early diagnosis is important not only to prevent further neurologic deficit but also, by allowing a reduction in radiation field and/or dose, to obtain a reduction in posttreatment sequelae and preservation of neurocognitive function, while preventing recurrence or progression of the disease. The early CT and MR imaging findings of germinoma reported herein may help facilitate a correct diagnosis of germ cell tumors in young patients, even if they are observed bilaterally.
Conclusion
Although germ cell tumors arising in the basal ganglia are usually unilateral, they can involve bilateral basal ganglia simultaneously. Because early diagnosis may improve patient outcome, it is important to recognize the early MR imaging findings of basal ganglionic germ cell tumors. The findings of a hyperintense area on T1-weighted MR images of the basal ganglia could be crucial for the diagnosis of germ cell tumors. Because the early imaging findings may be subtle and may therefore be misdiagnosed, we must pay special attention to these, especially in young patients with slowly progressive neurologic symptoms.
References
- Received April 24, 2004.
- Accepted after revision July 30, 2004.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.