Abstract
BACKGROUND AND PURPOSE: Benign and malignant fractures of the spine may have similar signal intensity characteristics on conventional MR imaging sequences. This study assesses whether in-phase/opposed-phase imaging of the spine can differentiate these 2 entities.
METHODS: Twenty-five consecutive patients who were evaluated for suspected malignancy (lymphoma [4 patients], breast cancer [3], multiple myeloma [2], melanoma [2], prostate [2], and renal cell carcinoma [1]) or for trauma to the thoracic or lumbar spine were entered into this study. An 18-month clinical follow-up was performed. Patients underwent standard MR imaging with an additional sagittal in-phase (repetition time [TR], 90–185; echo time [TE], 2.4 or 6.5; flip angle, 90°) and opposed-phase gradient recalled-echo sequence (TR, 90–185, TE, 4.6–4.7, flip angle, 90°). Areas that were of abnormal signal intensity on the T1 and T2 sequences were identified on the in-phase/opposed-phase sequences. An elliptical region of interest measurement of the signal intensity was made on the abnormal region on the in-phase as well as on the opposed-phase images. A computation of the signal intensity ratio (SIR) in the abnormal marrow on the opposed-phase to signal intensity measured on the in-phase images was made.
RESULTS: Twenty-one patients had 49 vertebral lesions, consisting of 20 malignant and 29 benign fractures. There was a significant difference (P < .001, Student t test) in the mean SIR for the benign lesions (mean, 0.58; SD, 0.02) compared with the malignant lesions (mean, 0.98; SD, 0.095). If a SIR of 0.80 as a cutoff is chosen, with >0.8 defined as malignant and <0.8 defined as a benign result, in-phase/opposed-phase imaging correctly identified 19 of 20 malignant lesions and 26 of 29 benign lesions (sensitivity, 0.95; specificity, 0.89).
CONCLUSION: There is significant difference in signal intensity between benign compression fractures and malignancy on in-phase/opposed-phase MR imaging.
Abnormal signal intensity in benign compression fractures on conventional MR imaging can be similar to that seen in vertebrae with underlying malignancy. In an effort to differentiate between benign and malignant disease, morphologic criteria as well as diffusion imaging has been used. Because benign vertebral fractures should contain fatty marrow and malignant processes replace normal marrow,1 differentiation of these 2 processes should be possible with in-phase/opposed-phase imaging. This technique has been used extensively in separating benign from malignant adrenal lesions as well as differentiating fatty infiltration of the liver from neoplastic disease. We hypothesize that in-phase/opposed-phase imaging of the spine should be a sensitive and specific way to differentiate benign from malignant signal intensity abnormalities in the spine.
Methods
From January 2003 through June 2003, 25 consecutive patients with a history of suspected acute vertebral compression fracture or known primary malignancy with suspected spinal metastasis and who were referred for MR imaging were entered in this study. Two patients were examined twice. An 18-month clinical follow-up was performed from June 3, 2003 through mid-December 2004.
Of the 14 patients with malignancy, 2 had x-ray therapy (XRT) more than 2 years before their examinations. Two patients received XRT after their first examinations but before the second study. The remaining patients had no radiation therapy. Chemotherapy was administered to patients as clinically appropriate to the disease. All patients underwent standard imaging of the spine on a 1.5T super-conducting magnet. This consisted of T1, proton attenuation, and fat-suppressed T2-weighted fast spin-echo images in the sagittal plane, as well as T1- and T2-weighted fast spin-echo images in the axial plane. In imaging the thoracic spine, the proton attenuation images were not performed. In addition to the routine sequences, sagittal in-phase (repetition time [TR], 90–185; echo time [TE], 2.4 or 6.5; flip angle, 90°) and opposed-phase gradient recalled-echo sequences (repetition time [TR], 90–185; echo time [TE], 4.6–4.7; flip angle, 90°) were acquired. The duration of the extra sequence was 32 seconds. Patients with a history of malignancy received gadolinium as part of the routine protocol if this was believed to be necessary at the time of examination. Patients with a history of trauma did not. The patients were followed for 18 months after the completion of the study; the final clinical diagnosis was used as the “gold standard” to classify the vertebral lesions as benign or malignant.
All images were then sent to a PACS workstation, and areas that were of abnormal signal intensity on the T1 and T2 sequences were identified on the in-phase/opposed-phase sequences. When this was unclear on visual inspection of the in-phase/opposed-phase images, a spatial mapping function was used to precisely locate the abnormal area on the routine images, and this area was cross-referenced to the in-phase/opposed-phase images. An elliptical region of interest cursor was placed over the abnormal area on the in-phase as well as on the opposed-phase images. Three measurements of the signal intensity were made and the average recorded (Fig 1). A computation of the signal intensity ratio (SIR) of the marrow on the opposed phase to signal intensity measured on the in-phase images was made.
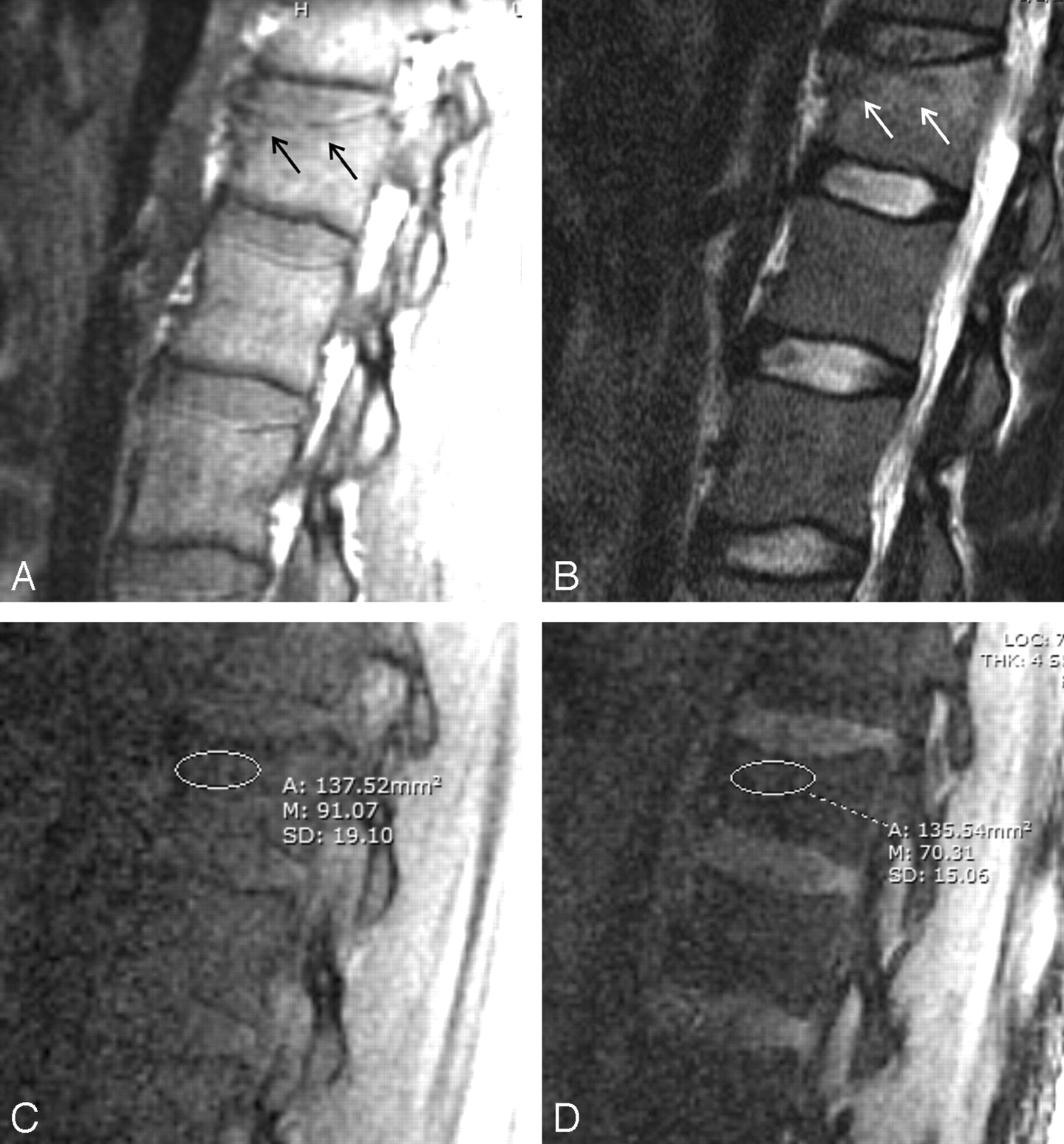
Motor vehicle crash involving 31-year-old man. Images demonstrate signal intensity–to-noise measurement technique used in assessing the abnormal signal intensity in the acute T12 compression fracture (arrows).
A, T1-weighted image.
B, T2-weighted image.
C, In-phase image.
D, Opposed-phase image. Region of interest cursor is on the region of abnormal signal intensity on the T1- and T2-weighted images. SIR is 0.76, indicating the presence of fat or benign marrow. Note the suppression of signal intensity from the normal fatty marrow in the adjacent vertebra.
Student t test and receiver operating characteristic analyses were performed.
Results
One patient had to be eliminated from the study because of motion artifact. Three patients who had no evidence of either compression fracture or malignancy on the standard sequences were also eliminated. The remaining 21 patients had 49 vertebral body lesions, either a benign compression fracture or metastatic deposit. No patient with metastatic disease had a single lesion, and only 2 patients with a benign fracture had metastatic disease. These patients had follow-up MRIs that included the fracture site and documented normal marrow at the fractured level. Two patients were examined twice. There were 29 benign compression fractures and 20 regions of malignant infiltration identified in the 23 examinations.
Of the 29 benign lesions, 26 had relatively decreased signal intensity on the T1-weighted images, and increased signal intensity on the T2-weighted images compared with normal marrow. Three patients had lesions that were isointense to normal marrow on both the T1- and T2-weighted sequences but were included in the study group because of the clinical diagnosis of acute fracture. The SIR of these 3 lesions was 0.79, 0.31, and 0.70.
Of the 20 malignant lesions, 18 had decreased signal intensity compared with normal marrow on the T1-weighted images. Two melanoma metastases were isointense to normal marrow on the T1 sequences. On the T2-weighted sequences, 4 lesions (1 each of myeloma, lymphoma, breast cancer, and melanoma) were isointense to normal marrow; the remaining 16 lesions had increased signal intensity. One of the melanoma lesions was isointense to marrow on both the T1- and T2-weighted images, but metastatic disease was confirmed on an enhanced fat-suppressed T1 sequence after gadolinium administration.
When the SIR is calculated, there is a significant difference (P < .001, Student t test) in the mean SIR for the benign lesions (mean, 0.58; SD, 0.02) compared with the malignant lesions (mean, 0.98; SD, 0.095). Of the 2 papients who had a remote history of prior XRT, both patients had malignant-appearing lesions on their examinations that were positive by in-phase/opposed-phase imaging.
Two patients had 3 lesions treated by XRT between their 2 studies. Two of these remained malignant by SIR and 1 reverted to a benign SIR, though the T1- and T2-weighted images remained abnormal. If a SIR of 0.80 as a cutoff is chosen, with >0.8 indicating no suppression of signal intensity (and therefore no fat) defined as a malignant result and <0.8 defined as a benign result, in-phase/opposed-phase imaging correctly identified 19 of 20 malignant lesions and 26 of 29 benign lesions (sensitivity, 0.95; specificity, 0.89) (Fig 2). The sole malignant lesion that was classified as benign was in a patient who had been treated with XRT for lymphoma. The initial evaluation of the affected level was correctly identified as malignant. On the follow-up study, the SIR changed from malignant to benign, though the T1- and T2-weighted sequences remained abnormal.

Plot of SIR of the data points with triangle indicating the benign fractures and circle denoting the malignant marrow infiltration. While there is variation in the SIR of the benign lesion, malignant infiltration does not suppress.
Discussion
Despite the common usage of in-phase/opposed-phase imaging of the adrenal glands and liver, relatively few studies assess the utility of this technique in the spine.1,2 In clinical practice, the differentiation between a chronic benign fracture and malignancy is usually not difficult. Morphologic criteria, though not perfect, may accurately predict benign from malignant fractures of the spine in up to 94% of cases.3 The important clinical question is whether there is an underlying marrow-replacing process when areas of abnormal signal intensity are observed on conventional imaging. This can be particularly vexing in patients with a history of malignancy and no evidence of osseous metastases elsewhere. Although patterns of signal intensity abnormality on conventional images can suggest one cause or another, there are still cases in which the diagnosis is uncertain. Diffusion imaging has provided some promise in this regard.4–7
In-phase/opposed-phase imaging to assess for the presence of fat and water in a voxel of tissue has been used extensively in imaging of the liver and adrenal glands. The technique takes advantage of different precession frequencies of water and fat protons due to the differences in their molecular environment. Because they precess at slightly different frequencies, at 1.5T, water and fat protons are in phase with one another at a TE of 4.6 ms, and 180° opposed at a TE of 2.4 msec. This phenomenon is not usually evident on spin-echo sequences. Without a refocusing pulse, when there are both fat and water protons in a given voxel, there will be some signal intensity loss on images that are obtained when the protons are in their opposed phase (TE = 2.4 ms) (Fig 3). More signal intensity suppression occurs when the volume of fat and water is roughly equal. There have been a few previous reports that have described in-phase/opposed-phase imaging of the spine and marrow.1,2,8,9

Illustration of the physical principles of in-phase/opposed-phase imaging.
A, At echo time (TE) of 4.6 ms, both the fat and water protons are in phase, and signal intensity is received from voxels containing both tissue types.
B, At TE of 2.4 ms, the protons on water and fat molecules are 180° opposed, and the signal intensity from one cancels the signal intensity from the other. Voxels that contain both tissue types have a reduction in signal intensity.
We hypothesized that in-phase/opposed-phase imaging of the spine should be a sensitive and specific method for differentiating pathologic from benign compression fractures. The presence of both fat and water in normal marrow results in suppression of signal intensity on the opposed-phase images.10 In benign compression fractures, although the signal intensity on conventional spin-echo sequences is abnormal, no marrow-replacing process has occurred. The existence of normal marrow fat should result in suppression of signal intensity on the opposed-phase images. In pathologic fractures, normal fat-containing marrow is replaced with tumor, which should result in lack of suppression on the opposed phase images (Fig 4).

Metastatic melanoma in a 56-year-old man.
A and B, Routine T1- and T2-weighted images of metastatic melanoma with pathologic fracture of L2 (arrows). Metastatic lesions of L1 and L3 are difficult to see on the routine sequences.
C, In-phase image (TE = 4.6 ms).
D, Opposed-phase image (echo time [TE] = 2.4 ms). Marrow replaced by tumor does not suppress (arrows), whereas the normal fatty marrow appears dark on these images (asterisks).
E, In-phase image with region of interest cursor in place. Signal intensity ratio of L2 is 0.90, indicating the absence of fat and a malignant result.
F, Opposed-phase image with region of interest cursor in place. Signal intensity ratio of L2 is 0.90, indicating the absence of fat and a malignant result.
One of the false-negative examinations (Fig 5) was in a patient who had been treated with XRT between the initial and follow-up studies. Even though the marrow signal intensity remained abnormal on the standard sequences, the marrow signal intensity returned to normal on the in-phase/opposed-phase. Although we have no proof other than the known efficacy of XRT in the treatment of metastases, one wonders whether the normalizing signal-to-noise ratio in these 2 cases is an indication of response to therapy. The false-positive examinations may have been because for maximum opposed-phase suppression, relatively equal amounts of fat and water are necessary. These lesions may have undergone some healing with resultant new bone growth or scar tissue formation. Research regarding the time course of marrow healing and signal intensity changes on in-phase/opposed-phase imaging may be of interest.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lymphoma in a 33-year-old man. False-negative for malignancy.
A and B, T1- and T2-weighted images, respectively, done in February 2003 show abnormal decreased signal intensity (arrows) on the T1-weighted sequence and increased signal intensity (arrows) on the T2-weighted sequence compared with normal marrow. These findings were considered to be due to lymphomatous marrow infiltration.
C and D, In-phase image and opposed-phase image, respectively, done in February 2003. Signal intensity measurement is 202 on the in-phase sequence and 215 on the opposed phase, a ratio of 1.1 or a malignant result.
E–H, T1-weighted, T2-weighted, in-phase, and opposed-phase images 3 months later. Patient has received prior radiation therapy. T1- and T2-weighted images continue to show abnormal signal intensity relative to the normal marrow (arrows), though the signal intensity changes have evolved since the initial examination. Signal intensity on the in-phase image is 90 and 46 on the opposed-phase, a SIR of 0.51, a benign result in a lesion that was still considered malignant on the routine sequences.
The findings in this study are similar to those of previous studies in the literature. One study2 found a significant difference in SIR between benign and malignant fractures, but noted that some of the benign fractures did not suppress on the opposed-phase images. The sensitivity and specificity of their data were not provided. A second study found the opposed-phase imaging to be 89% sensitive and 80% specific1 in the detection of malignancy. However, the latter study design differed from the current study design in that the SIR was computed relative to the marrow signal intensity on T1-weighted imaging, and in-phase imaging was not performed.
Three of the patients with a clinical diagnosis of acute compression fracture did not have evidence of an acute fracture on MR imaging. However, the mean SIR of these 3 vertebrae was higher than the mean SIR for benign lesions in general, and inclusion of these lesions in this study does not affect the outcome.
A problem with the design of this study is the lack of pathologic proof of the presumed malignant lesions and lack of follow-up imaging in the case of the benign lesions; however, in 18 months of clinical follow-up, there have been no cases in which the presumed benign lesions proved to be malignant. Although there is potential for misdiagnosis of any of the lesions, we believe that MR imaging in combination with the clinical data makes this sufficiently unlikely as to not alter the results of this study. A second problem is that the lesions selected for inclusion in the study were not problematic from an imaging standpoint. If this technique were to be used in clinical practice, it would only have utility in those lesions in which the diagnosis is in question. These lesions were not specifically included.
Of interest is the return to benign SIR of a malignant lesion that was treated with XRT, whereas the standard spin-echo sequences remained abnormal. In-phase/opposed-phase imaging may prove to be an early marker for response to treatment of osseous metastatic disease.
It is easy to imagine a situation in which a pathologic compression fracture contains some fat because the volume of fractured bone exceeds the volume of tumor. In those cases, one might observe suppression of signal intensity on the opposed-phase images and a false-negative result might be obtained. Conversely, based on the current data, it is clear that some benign fractures do not contain sufficient fat to suppress on the opposed-phase sequences. The evolution of the signal intensity changes in benign compression fractures over time with this technique is not known. It may be that the number of false-positives for malignancy of this technique may be reduced when used within a specified time period after the occurrence of a fracture.
Both diffusion imaging and this technique rely on the replacement of the fat in the marrow to generate image contrast. DWI relies on the diffusion of many different cell types to be sufficiently different from fat to generate consistent contrast differences. In-phase/opposed-phase imaging relies only on the absence of fat, rather than similarities in different neoplastic cell lines to produce image contrast. This may make this technique more specific in identifying benign lesion of the spine than diffusion-weighted imaging (DWI) or be a useful supplement to DWI in assessing problematic vertebral body lesions.
Conclusion
In-phase/opposed-phase imaging may be useful in differentiating acute benign compression fractures from malignant infiltration and pathologic fractures. Furthermore, it may be an early indicator of response to treatment after radiation therapy to the spine and additional research could be performed. At our institution, this technique is used to help differentiate benign from malignant compression fractures of the spine when this is a clinical or radiologic concern.
References
- Received August 23, 2005.
- Accepted after revision October 13, 2005.
- Copyright © American Society of Neuroradiology