
Abstract
BACKGROUND AND PURPOSE: The noninvasive identification of plaque types prone to cause symptomatic disease is of great interest to improve the effectiveness of surgical or interventional management. The purpose of the present prospective pilot study was to evaluate the association between the results of imaging—the novel sonography technique B-flow imaging (BFI), B-mode, and color Doppler imaging (CDI)—and histopathologic examination in the characterization of internal carotid artery (ICA) plaques.
METHODS: Twenty-eight consecutive patients with high-grade internal carotid artery stenosis scheduled for carotid endarterectomy were included. BFI, B-mode, and CDI images were used to classify the plaques applying the standardized scores of Beletsky et al and the American Heart Association (AHA), to calculate the gray-scale median (GSM) and to detect potential ulcerations; histopathologic examination results of explanted plaques served as the “gold standard.”
RESULTS: Based on the classification of Beletsky et al, BFI and histopathologic examination results agreed in 21 (75%, κ = 0.61, P < .001) patients, and the corresponding results for B-mode were 19 (68%, κ = 0.52, P < .001) patients, respectively. Corresponding results for the AHA classification revealed inferior agreements for BFI (19 patients/68%, κ = 0.38, P = .003) and B-mode (17 patients/61%, κ = 0.25, P = .045). The median GSM for BFI and B-mode correlated significantly (r = 0.95, P < .001). The sensitivity of BFI for the detection of ulcerated plaques was 100% and the specificity was 95.8%; corresponding values for CDI were 100% and 92.7%, respectively.
CONCLUSION: BFI and the combination of B-mode and CDI exhibit comparable results in the assessment of ICA plaque components and plaque ulceration as well as in the determination of GSM levels.
European (ECST)1 and North American (NASCET)2 carotid surgery trials have proved the benefit of carotid endarterectomy (CEA) in patients with symptomatic internal carotid artery (ICA) stenosis ≥70%. It has also been demonstrated that carotid artery stent (CAS) placement with the use of an emboli protection device is not inferior to CEA.3 However, surgery is needed in approximately 14 patients to prevent 1 ipsilateral carotid territory major ischemic stroke lasting longer than 7 days over the next 5 years.4 In addition, an overall complication rate of 6% and 8% for CAS and CEA, respectively, must be considered.3,5 Therefore, noninvasive identification of plaque types prone to cause symptomatic disease would help to improve the effectiveness of surgical or interventional management, because it is well recognized that many cerebrovascular events are associated with ICA <70%.3,5,6
Several noninvasive techniques have been evaluated for the characterization of the plaque constitution because, with the exception of luminal ulceration, carotid angiography fails to demonstrate plaque morphology.7–11 The predominant imaging technique being investigated for this purpose is ultrasonography.8,10,12,13 Vulnerable and rupture-prone carotid plaques have been subjectively characterized as echolucent and heterogeneous,8 though computer-assisted analysis has shown low gray-scale-median (GSM) values in B-mode imaging.12–14 Color Doppler imaging (CDI) has been used for the evaluation of the plaque’s boundary, but maximizing the color fill-in of vessels almost always results in some overwriting of the vessel walls—the so called “blooming artifact”—which may mask structure details.15 Therefore, B-flow imaging (BFI) has been introduced recently, extending B-mode imaging capabilities to blood flow.15–17 It directly depicts blood echoes in a grayscale presentation and simultaneously depicts surrounding anatomy without the need for overlays. Thus, we speculated that BFI might represent the optimal technique for the assessment of the plaque components as well as its border.
The purpose of the present prospective pilot study was to assess the value of BFI compared with B-mode in combination with CDI in the characterization of ICA plaques by using histopathologic examination of explanted plaques as the “gold standard.” In addition, we analyzed the correlation of GSM values of both sonography techniques and finally assessed the sensitivity and specificity of BFI and CDI in the detection of plaque ulceration.
Methods
Consecutive patients with internal carotid artery stenosis (ICAS) > 70% according to the NASCET criteria,18 either neurologically symptomatic or asymptomatic as assessed by a neurologist and scheduled for CEA, were enrolled in this present prospective pilot trial. All patients underwent B-mode, CDI, and BFI on the day before surgery. Finally, the extracted plaques were analyzed by histopathologic examination after CEA. The trial complied with the principles of the Declaration of Helsinki, and written informed consent was obtained from all patients.
Sonography
The examination was performed on a GE Logiq 9 scanner with 5–14 MHz linear probe (GE Sonography Europe, Solingen, Germany) by an experienced sonographer. The BFI technique has been described in detail previously15; in short, BFI uses digitally encoded ultrasound (US) technology in a digital beam former that provides electronic array focusing. A small number of digitally encoded wideband pulses are transmitted into the body for each scan line. Directly after receiving the reversed pulses, the decoder performs pulse-length compression (a technique that increases the transmission energy by as much as an order of magnitude without compromising transverse resolution) on the acoustic data and then performs clutter suppression filtering. The rest of the processing is essentially the same as in conventional B-mode. Standard imaging parameters were used for B-mode and CDI: B-mode settings were adjusted and standardized using a maximum dynamic range (60 dB) and by setting the gain to ensure an almost noiseless vessel lumen (blood) and an echo-attenuated area of adventitia. For CDI, setting was optimized for color-filling of the vessel (long persistence, adequate velocity setting and color gain) and minimizing wall movement and tissue artifacts. For BFI, we used time-gain compensation fixed in a medium position for all patients, gain adapted for optimized image quality (echo-attenuated area of adventitia), and a dynamic range of 60 dB with linear gray-scale calibration. The background suppression option was not used. Longitudinal and cross-sectional images were obtained and stored digitally on the hard disk drive of the scanner and on a CD-ROM in tagged image file format.
Two observers who were not involved in the image acquisition and were blinded to the results of histopathologic examinations, analyzed the images of each method separately in a random order of patients. Discrepant interpretations were solved by discussion, and a consensus scoring was used for the final analysis. In the first step, we analyzed the plaque composition using the score published by Beletsky.19 In short: 1) soft plaque/organized thrombus, 2) intraplaque hemorrhage/fatty deposition, and 3) fibrosis/densely calcified plaques. Plaques classified by sonography in group 1 exhibited a lower attenuation (<2 times the blood attenuation) than group 2, which in turn had a lower attenuation than group 3 (as attenuated as the surrounding connective tissue with or without additional acoustic shadowing).19 In addition, we used an adapted version of the AHA classification,20 modified for the usage with sonography imaging: I) atheroma/fibroatheroma (= extracellular lipid pool, with or without a cap rich in fibrosis), II) calcified plaque, III) fibrotic plaque (= fibrous connective tissue, no lipid core), and IV) wide hemorrhage or thrombosis. Plaques classified by sonography in group IV had a low attenuation (<2 times the blood attenuation), an intermediate (between the attenuation of the blood and the surrounding connective tissue) attenuation for group I, a high attenuation (as attenuated as the surrounding connective tissue) with acoustic shadowing in some planes for group II, and a high attenuation without shadowing for group III. We then assessed the GSM of the plaque for BFI and B-mode as described recently.14 In short, images were analyzed on a personal computer using Adobe Photoshop 7.0 (Adobe Systems, San Jose, Calif). We adjusted the linear scale of the “curves” facility of the software to achieve gray values of the blood between 0 and 5 (for B-mode) and of the adventitia between 185 and 195 (for both techniques). In such standardized images, plaques were outlined with the cursor and measurements of the GSM were obtained from the histogram. Then, GSM values were correlated with the histologic classification of Beletsky et al19 and the American Heart Association (AHA).20 We also analyzed the sensitivity and specificity of GSM ≤25 in the detection of symptomatic patients.14
Finally, we analyzed the plaque border for potential ulcerations, which were defined as recesses in the contour of the lesion at least 2 mm in depth, with a well-defined back wall at the base showing flow vortices without frequency aliasing within the recess.21
Plaque Morphology and Analysis of Histopathologic Specimens
The atherosclerotic plaque of the ICA was excised en bloc at CEA. Particular care was taken not to disturb the plaque surface by irrigation or suctioning. The fresh specimens were rinsed briefly in normal saline solution to remove the surface blood and were immersed in 10% formalin fixative and subsequently in a decalcifying solution (formic acid). Then the specimens were sectioned with a disposable microtome knife, and the blocks were numbered in sequence starting at the proximal end. Each block was processed through paraffin, sectioned at 5 μm, and then stained in sequence with hematoxylin-cosin, Martius Scarlet blue, and Perls solution. An experienced vascular histopathologist—blinded to the results of sonography and the patient’s symptoms—examined all specimens for the presence of a fibrous cap, focal calcification, necrotic core, media, surface thrombus, intraplaque hemorrhage, and intraplaque fatty deposition and finally classified the specimens according to the scores of Beletsky et al19 and the AHA.20 In addition, he decided about the presence of plaque ulcerations, which was recorded where there was clear break in the fibrous cap, usually at a point of thinning and inflammation, and where the break in the cap did not seem to have been created during surgery.9
Statistical Analysis
For statistical analysis, we used SPSS 11.5 statistical software (SPSS, Chicago, Ill). All numeric data are stated as the median with the interquartile range (IQR); categorical data are stated as frequency analysis. Cross-table procedures were used for the correlation analyses of categorized data as well as the assessment of the sensitivity and specificity. Correlation analyses of the results of the plaque classifications between imaging modalities and histopathology use κ statistics; agreement was interpreted according to the scale of Landis and Koch: very good, κ > 0.81; good, κ = 0.8–0.61; moderate, κ = 0.6–0.41; poor, κ = 0.4–0.21; and bad, κ < 0.21. Spearman correlation coefficient (r) was used for numeric correlation analysis. A P value < .05 was defined as significant.
Results
Thirty-two patients were screened for participation. One patient refused to participate, leaving 31 patients who underwent sonography. In 3 (10%) of them, surgery was cancelled because of poor medical condition (2 patients) and a previously radiated neck (1 patient). Therefore, 28 (88%) patients were included for final analysis. Ten patients (36%) were female, and 18 patients (64%) were male; the mean age was 71 ± 9 years. Thirteen patients (46%) were judged as symptomatic by the neurologist; symptoms included brachiofacial transient ischemic attack in 5 patients (38%), retinal symptoms in 4 patients (31%), transient aphasia in 3 patients (23%), and acute stroke in 1 patient (8%).
All specimens as well as all stored images of the included patients were classified. Based on the classification of Beletsky et al, BFI and histopathologic examination results agreed in 21 (75%, κ = 0.61, P < .001) patients; the corresponding results for B-mode were 19 (68%, κ = 0.52, P < .001) patients. Corresponding results for the AHA classification revealed inferior agreements for BFI (19 patients/68%, κ = 0.38, P = .003) and B-mode (17 patients/61%, κ = 0.25, P = .045). Further details are provided by Tables 1 and 2. Figure 1 demonstrates a perfect correlation of BFI (Fig. 1A) and CDI (Fig. 1B) with histopathologic examination (Fig. 1C).

Magnified (A) BFI and (B) CDI images and (C) histologic specimen of a 78-year-old asymptomatic patient (Beletsky III, AHA II); ultrasonography was in almost perfect accordance with histologic examination results, which demonstrates a plaque with fibrous intimal cap, debris, foam cells, and cholesterol deposition. * indicates the plaque.
Results of B-Flow Imaging and B-Mode Using the Classification of Beletsky et al19 as Well as Corresponding Median Gray-Scale-Median of All Investigated Patients; Histopathologic Examination Serves as the ‘Gold Standard’
Results of B-Flow Imaging and B-Mode Using the Classification of the AHA20 as Well as Corresponding Median Gray-Scale-Median of All Investigated Patients; Histopathologic Examination Serves as the ‘Gold Standard’
The median GSM for BFI and B-mode were 33 and 27 (IQR 40 and 52), respectively; values correlated significantly (r = 0.95, P < .001). The median BFI-GSM of symptomatic patients was 24 (IQR 52) and 40 (IQR 51) for asymptomatic patients. A GSM cutoff value ≤25, as proposed by Biasi et al,14 resulted in a sensitivity of 54% (7/13) and a specificity of 67% (10/15) for the detection of symptomatic disease.
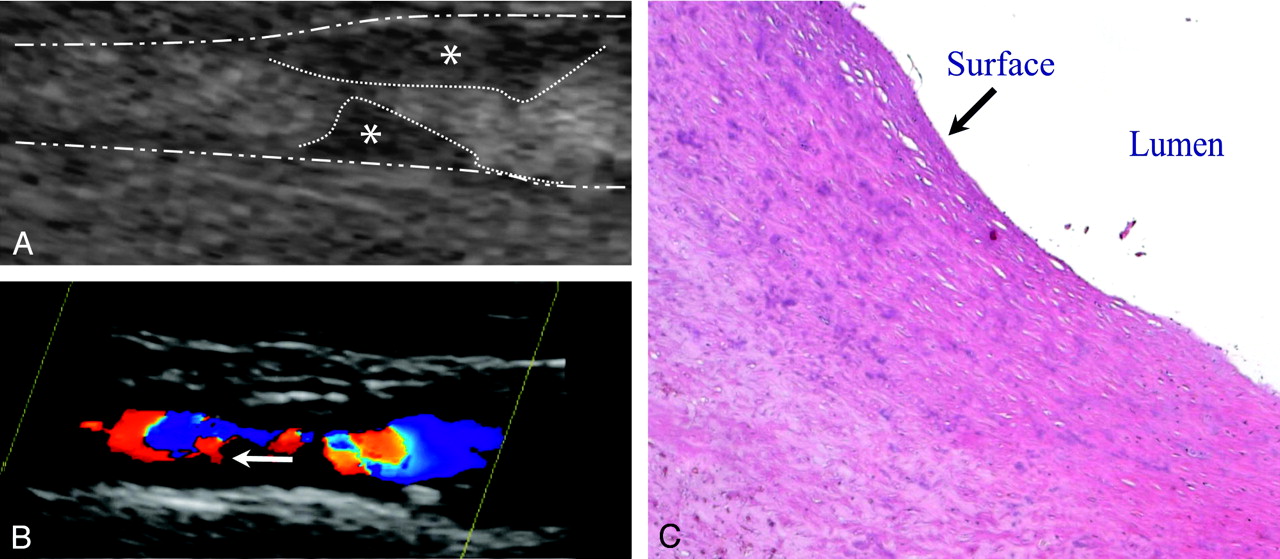
Using histopathologic examination as the “gold standard,” BFI exhibits a sensitivity for the detection of ulcerated plaques of 100% (4/4) and a specificity of 95.8% (23/24); corresponding values for CDI were 100% (4/4) and 92.7% (22/24). Three of 4 (75%) patients with ulcerated plaques verified on histologic examination were symptomatic. Figure 2 demonstrates a patient with suspected ulceration by CDI (Fig. 2B), but regular surface shown by BFI (Fig. 2A) and histopathology (2C). Fig 3 demonstrates a case with an ulcerated plaque.

Magnified (A) BFI and (B) CDI images of a 51-year-old asymptomatic patient (Beletsky III, AHA III) indicating the regular surface on BFI and a suspected ulceration on CDI. Histopathologic examination results demonstrate the continuous integrity of the luminal surface of the plaque (C). · · · outlines the plaque, − ·· − outlines the adventitia, * indicates the plaque; arrow demonstrates the false-positive ulceration on the CDI image.
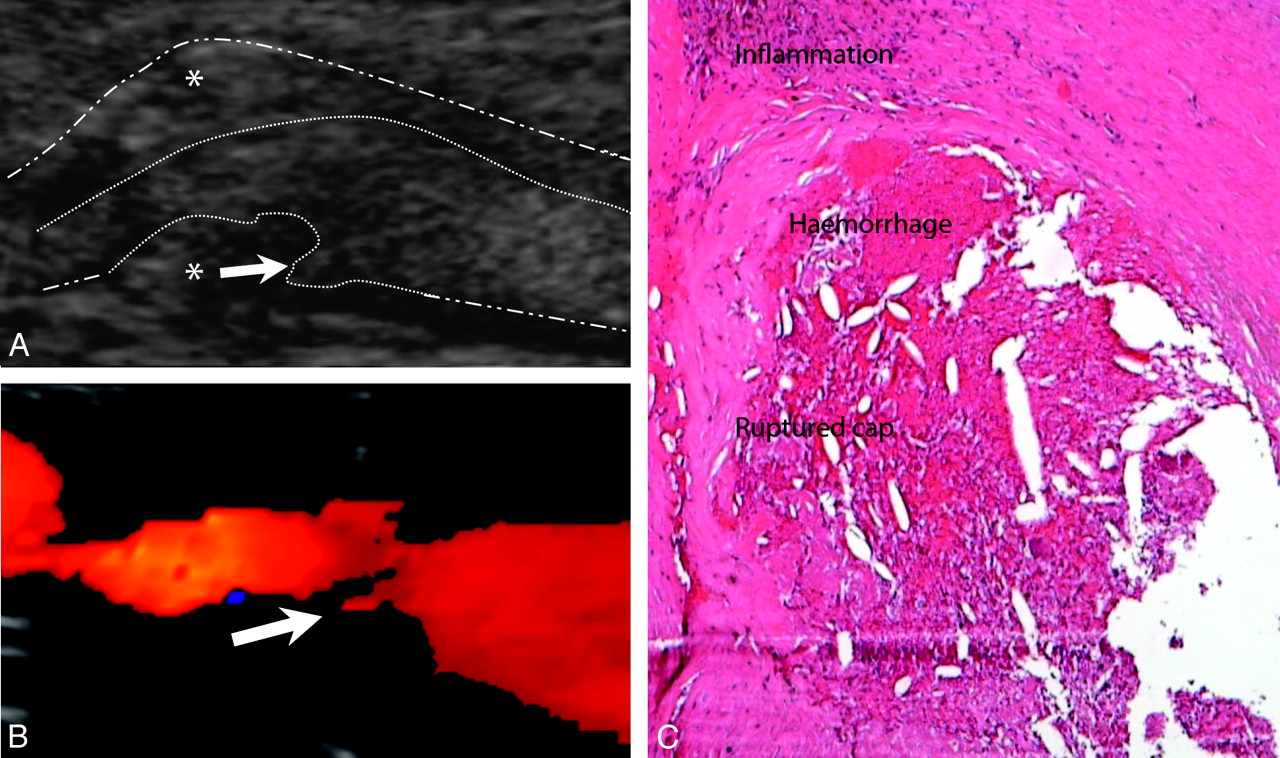
Magnified (A) BFI and (B) CDI images and (C) histologic specimen of a 76-year-old symptomatic patient (cerebral insult 4 weeks before imaging; Beletsky II, AHA I); imaging and histology clearly demonstrate the irregular luminal surface and the ulceration of the plaque with hemorrhage and concomitant inflammation. ··· outlines the plaque, − ·· − outlines the adventitia, * indicates the plaque; arrows demonstrate the ulcerations on BFI and CDI images.
Discussion
The sonographic characteristics of carotid plaques have been the subject of intense research in the last few years. It has been recognized that the surface of the plaque and its morphology are related to clinical symptoms.8,13,22,23 However, previous data demonstrated that, on the one hand, subjective sonography characterization is associated with low levels of reproducibility24 and, on the other hand, that objectively determined GSM levels exhibit a very low level of agreement with results of histopathologic examination.25 In addition, computerized analysis of echo attenuation is dependent on postimaging processing on a personal computer and is presently not available in commercially used duplex sonography systems.
The present trial is the first direct correlation between the results of BFI and histopathologic examination in the evaluation of atherosclerotic plaques. We demonstrated a good agreement of BFI and histopathologic examination by using the 3-category classification proposed by Beletsky et al,19 whereas B-mode demonstrated comparable but slightly inferior results. Both imaging modalities achieved inferior correlations concerning the 4-category AHA classification.20 The histopathologic basis of the AHA classification, including various detailed plaque characteristics, seems to us to be a potential explanation for these latter results. In detail, most discordant classifications had been observed in AHA grade I (atheroma/fibroatheroma), which especially exhibits an inhomogeneous plaque composition. In addition, it has been observed that the correlation of imaging and histopathologic examination decreases with an increasing number of subclassifications, which has even been reported for MR imaging20 and spiral CT.26 Finally, sonography cannot demonstrate the total plaque volume on a 2-dimensional single image, and different angulated views are needed to overcome potential shadowing artifacts caused by heavily calcified plaques.
We demonstrated that GSM values measured on BFI images correlated well with those assessed by B-mode images (r = 0.95), though only the adventitia could be standardized on BFI images because of the blood echoes in a gray-scale presentation. The missing standardization of the blood lumen had no significant influence on GSM levels; thus, GSM testing can also be accurately performed by BFI. In accordance with the literature, we detected lower GSM values (24 versus 40) in symptomatic patients compared with asymptomatic patients.12,13,27 However, based on the small sample size, we did not evaluate a potential statistical significance. The proposed cutoff level of ≤25, which has been reported to increase the risk of stroke in CAS,14 did not reveal an acceptable sensitivity and specificity for symptomatic disease. Further trials with appropriate design and a sufficient statistical power are therefore needed to clarify the role of GSM analysis in the detection of symptomatic cerebrovascular disease.
As a further goal, we focused on the detection of plaque ulceration, which has been related to neurologic events in ICAS.6,23 We demonstrated an excellent sensitivity and specificity of BFI and CDI for the detection of ulceration. Our data analyzing CDI correspond well to the results of Furst et al,28 who demonstrated a sensitivity of 95% and a specificity of 94%. However, these findings were challenged by Sitzer et al,29 who failed to reliably identify plaque ulceration by CDI. In the interpretation of the negative result of their study, the fact that most ulcers detected by pathologic examination were flat with a surface defect of approximately 1 mm in width has to be considered.29 However, we could not confirm the hypothesis of an improved assessment of plaque ulceration of BFI compared with CDI. One explanation might be the small sample size, which is of course a limitation of the present study. However, in times of constraints on resources, detailed histologic work-up of plaques is costly and time-consuming, thus explaining the necessity of conducting a pilot trial. A further potential explanation for the low rate of ulcerated plaques is that imaging was closely related to the time of surgery to achieve a reliable comparison to histologic examination results. Therefore, some of the patients were imaged several weeks after the date the symptoms started and we cannot completely exclude the possibility that some ulcerations had been healed in the meantime.
Conclusion
The present trial is the first to compare BFI, which extends B-mode imaging capabilities to blood flow, and histopathologic examination using standardized scores. BFI and the combination of B-mode and CDI exhibit comparable results in the assessment of ICA plaque components and the detection of plaque ulceration, using histopathologic examination as the “gold standard.” In addition, BFI provides an excellent correlation with B-mode imaging concerning the determination of GSM levels.
References
- Received January 26, 2006.
- Accepted after revision April 24, 2006.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.