
Abstract
BACKGROUND AND PURPOSE: A controversial discussion concerning treatment of aneurysms in elderly patients exists. The aim of this study was to analyze clinical outcome in patients older than 65 years harboring intracranial aneurysms after endovascular treatment.
MATERIALS AND METHODS: A total of 108 patients aged 65 years or older (mean age, 72 years, range, 65–87 years) were selected for endovascular treatment between 1997 and 2005. A total of 85 (78.7%) patients had an acute subarachnoid hemorrhage (SAH). SAH was classified according to Hunt and Hess (HH) grade: I (n = 16), II (n = 11), III (n = 33), IV (n = 19), and V (n = 6). There were 69 aneurysms that were small; 46, medium; 8, large; and 5, giant. Occlusion rate was categorized as complete (100%), subtotal (95% to 99%), and incomplete (<95%) obliteration according to the Raymond scale.
RESULTS: Endovascular treatment was technically feasible in 108 of 113 aneurysms. Complete occlusion could be achieved in 80 patients; basal remnant was seen in 26 patients and a dog ear in 2 patients. Procedural complications included thrombotic vessel occlusion (n = 9), aneurysmal rupture (n = 4), and stenosis of the parent vessel (n = 2). The Glasgow Outcome Scale (GOS) for the patients with SAH after 6 months was good recovery (n = 43), moderate disability (n = 12), severe disability (n = 28), persistent vegetative state (n = 5), and death (n = 18). Outcome for the patients with unruptured aneurysms was good recovery in all 23 patients. On follow-up digital subtraction angiography (DSA) in 69 patients, complete aneurysmal occlusion was confirmed in 81% after 6 months. Five patients with recanalization were re-treated with coiling.
CONCLUSION: Endovascular treatment of ruptured and unruptured intracranial aneurysms in this subgroup was safe and effective.
The incidence of subarachnoid hemorrhage (SAH) increases with age: at the third decade of life, the incidence is approximately 1.5 to 2.5 per 100,000 per year, at the eighth decade, it is approximately 40 to 78 per 100,000 per year.1,2 Conservative treatment of ruptured aneurysms in elderly patients is known to be associated with a poor outcome.3 Some studies reveal a slightly better outcome after surgery,4 but these results are not consistent.5
There are some findings that the outcome in elderly patients is not associated by age but by the clinical grade of the aneurysm.6 First, results concerning endovascular treatment revealed a benefit in outcome for this patient group.7 However, because of a higher incidence of atherosclerotic diseases and tortuous vessels, the procedural complications in respect to thromboembolic events and therapy failure may increase. Furthermore, the individual life expectancy and the risk for aneurysmal rupture have to be estimated before a decision is made about therapy.8 Some studies on the use of endovascular therapies in elderly patients did reveal a higher risk for this subgroup of patients (eg, the SPACE study reported a higher risk for patients older than 70 years).9 Therefore, the question arises of whether endovascular therapy should be performed according to an age-related category.
Materials and Methods
Subjects
A total of 108 consecutive patients aged 65 years or older (mean age, 72 years; age range, 65–87 years) harboring 128 aneurysms were seen at our hospital between March 1997 and March 2005. All patients had been selected for endovascular treatment. A total of 85 (78.7%) patients had an acute SAH. The treatment was performed between 6 and 72 hours after symptom onset. SAH was classified according to Hunt and Hess (HH) grade: I (n = 16 [15%]), II (n = 11 [10%]), III (n = 33 [31%]), IV (n = 19 [17%]), and V (n = 6 [5%]).
Location of Aneurysms
The 108 patients harbored 128 aneurysms in total. The aneurysms were located either in the anterior (n = 95) or posterior (n = 33) circulation. The size of the aneurysm ranged from 2 to 30 mm. There were 69 aneurysms that were small (0–5 mm); 46, medium (6–10 mm); 8, large (11–25 mm); and 5, giant (>25 mm). Of the 95 aneurysms in the anterior circulation, 31 were at the internal carotid artery (ICA), 10 at the medial cerebral artery (MCA), and 54 at the anterior cerebral artery (ACA). Of the 33 aneurysms at the posterior circulation, 3 were at the vertebral artery (VA); 23, at the tip of the basilar artery (BA); 2, at the superior cerebellar artery (SCA); and 5, at the posterior inferior cerebellar artery (PICA).
Endovascular Procedure
All subjects were treated under general anesthesia. Treatment was performed as soon as possible after admission. In patients admitted with an acute SAH, treatment was performed within 3 days after SAH. A femoral approach was used in all patients. A 6F guiding catheter (FasGuide; Boston Scientific, Fremont, Calif or Envoy; Cordis Neurovascular, Miami Lakes, Fla) was used. A Tracker Excel-14 microcatheter and a Transend EX or platinum 14-guidewire (Boston Scientific) were used for selective catheterization of the aneurysm. For aneurysmal embolization, detachable coils were used: either a Guglielmi detachable coil (Boston Scientific) or MicroPlex (MicroVention; Terumo, Columbia, Calif). Coil thicknesses were 0.010 and 0.018 inches. We used a balloon-remodelling technique in 6 patients, and 3 patients were treated with a Neuroform stent (Boston Scientific).
Anticoagulation and antiplatelet therapy: Since 2004, in patients with an unruptured aneurysm, 250 to 500 mg of aspirin has been given intravenously before the procedure. In ruptured aneurysms, aspirin was given after the second or third coil. Before 2000, heparin (5000 IU) was given after the first coil in unruptured aneurysms and after the second or third coil in ruptured aneurysms.
All patients were transferred to the neurosurgical intensive care unit after the intervention. In cases of SAH, the patients were treated according to the German Guidelines for Treatment of SAH.10 Asymptomatic patients stayed in intensive care for at least 1 day. After acute bleeding, patients stayed in the intensive care unit according to their clinical follow-up. Aspirin (100 mg/day, orally) was given in 89 patients. At the time of treatment, 4 patients had severe vasospasm, which was treated with nimodipine administered intra-arterially through the guiding catheter to allow catheterization of the aneurysm.
The extent of aneurysmal occlusion was analyzed directly after treatment and at 6 months of follow-up with digital subtraction angiography (DSA) by a neuroradiologist experienced in aneurysm therapy. The rate of occlusion was categorized as complete (100%), subtotal (95% to 99%), and incomplete (<95%) obliteration. All patients underwent MR imaging within 3 days after the coiling procedure, including diffusion-weighted imaging (DWI). Follow-up MRA after 6 months was achieved in 103 patients and DSA in 69 patients. Clinical outcome was assessed according to the Glasgow Outcome Scale (GOS) on the day of discharge and at 6 months in 107 patients.
Statistics
Possible confounding effects of age or HH grade on outcome grading was tested by the Mann-Whitney U test. The threshold was set with P < .05.
Results
Endovascular treatment was technically feasible in 108 of 113 aneurysms. There were 15 incidental aneurysms in another location that were not intended to be treated in those patients with more than 1 aneurysm. In 4 (3.5%) patients, coiling could not be performed because of extreme elongated supra-aortal arteries. In 1 patient, the first coil occluded an important vessel coming out of the base of the aneurysm and was therefore withdrawn, resulting in a total of 4.4% of patients who could not be treated with endovascular therapy.
Complete occlusion could be achieved in 80 (74%) aneurysms. Subtotal occlusion was achieved in 27 (25%) aneurysms; only 1 (1%) aneurysm was occluded incompletely. According to the classification of aneurysm occlusion rates of Raymond et al,11 this group included 26 aneurysms with a neck remnant and 2 aneurysms with a dog ear. In 5 patients with vasospasms, nimodipine or papaverine was administered intra-arterially before coiling. After treatment of vasospasms, coiling was carried out with use of standard techniques.
In 1 patient with a large aneurysm and 2 patients with giant aneurysms, occlusion of the parent vessel was chosen as the therapeutic procedure. The patients had a sufficient cross-flow over the communicating arteries, and clinical symptoms were not revealed. Some small DWI lesions after therapy were revealed in only 1 of these patients, with no morbidity.
The overall number of patients with small (4–10 mm) and very small (1–3 mm) DWI lesions was 17 (16%). In an additional 15 patients with SAH, ischemia from vasospasm was revealed at follow-up.
Procedural complications included thrombotic vessel occlusion (n = 9), rupture of aneurysm,4 and stenosis of the parent vessel from coil protrusion.2 Four (17%) thrombotic events occurred in patients with unruptured aneurysms and 5 (6%) in the patients with acute SAH. In the 9 patients with thrombotic vessel occlusion, an intra-arterial lysis was performed, which was successful in 7 of these patients. For intra-arterial lysis, a maximum of 20 mg of tissue plasminogen activator was administered over a microcatheter. DWI revealed a small infarct in 4 of the 7 patients, with only minor or no neurologic symptoms. In 3 of the 7 patients, no DWI lesion was detected. Of the 2 patients with acute SAH and unsuccessful lysis, 1 patient had an infarct of the entire territory of the anterior cerebral artery. The other patient had some collateral vascularization but had brain edema and died before another CT scan could be performed.
Procedural rupture of an aneurysm was seen only in patients with acute SAH (5%). The rupture led to a severe bleeding in 2 patients followed by extended vasospasm. The other 2 patients did not have a detectable rebleeding on follow-up CT scans.
The parent vessel stenosis in 2 (2%) patients with acute SAH did not lead to any ischemia on initial MR imaging and at follow-up.
GOS for the patients with SAH after 6 months was good recovery (n = 20 [23%]), moderate disability (n = 12 [14%]), severe disability (n = 28 [34%]), persistent vegetative state (n = 5 [6%]), and death (n = 18 [21%]); 2 patients could not be contacted for follow-up. Of the 18 patients who died at follow-up, 10 were at an initial HH 4 and 5.
The distribution of age groups were analyzed as follows. Eight (44%) patients of this group were between 65 and 70 years old, 8 (44%) between 71 and 80 years old, and only 2 (11%) older than 80 years. The patients with GR at follow-up were initially HH 1 to 3; no patient was HH 4 or 5. Ten (50%) patients with GR at follow-up were between 65 and 70 years old, 9 (45%) were between 71 and 80, and only 1 (5%) patient was older than 80 years. The exact outcome for each HH stage is summarized in Table 1. The relative outcome is given in Fig 1. The distribution of outcome in correlation to age and HH is given in Fig 2A, -B. Table 2 gives the relative number of patients of the HH grading related to the age of the patient. No significantly higher HH grading in the older patient group was found.

The outcome of all patients treated with endovascular therapy for aneurysms is plotted against HH grading and given in percentages of all patients.

A, In this figure, the distribution of 3 age groups is plotted for the GOS values GR, MD, SD, and D. V was not plotted because this group was too small for relative calculations. B, In this figure, the distribution of HH grades are plotted for the GOS values GR, MD, SD, and D. V was not plotted because this group was too small for relative calculations.
Correlation of Hunt and Hess grade with Glasgow Outcome Scale after 6 months of follow-up
Hunt and Hess grade and age of the patients*
The statistical analyses revealed significant differences of the distribution of outcome in relationship to the HH grading. HH comparison revealed the following significant levels: HH 1 compared with 3 was .015, HH 1 compared with 4 was .001, and HH 1 compared with 5 was .003. HH 2 compared with 4 was .001, and HH 2 compared with 5 was .01. HH 3 compared with 4 was .002, and HH 4 compared with 5 was .01. The analyses of outcome in relationship to age groups did not reveal any significant differences: comparison of age groups 1 and 2 was .79, group 1 and 3 was .51, and group 2 and 3 was .44. Therefore, no comparison was significantly different.
Outcome for the asymptomatic patients was good recovery in all 23 patients. The asymptomatic patients had, compared with the whole group, a similar mean age of 70 years and a distribution between the ages of 65 and 77 years.
DSA was performed in 69 patients after 6 months. Of the 3 patients with the therapeutic vessel occlusion, 2 had a follow-up DSA, which revealed no recanalization or complication. A complete occlusion of the aneurysm was revealed in 56 patients. Within this group, 6 patients with initial basal rest after coiling presented with an occlusion from thrombosis on the follow-up DSA. An unchanged basal aneurysmal rest was seen in 7 patients and an unchanged dog ear in 1 patient. Three patients had a small recanalization on the aneurysmal base and 2 had more recanalization, which was re-treated with coiling.
Illustrative Cases
Case 1.
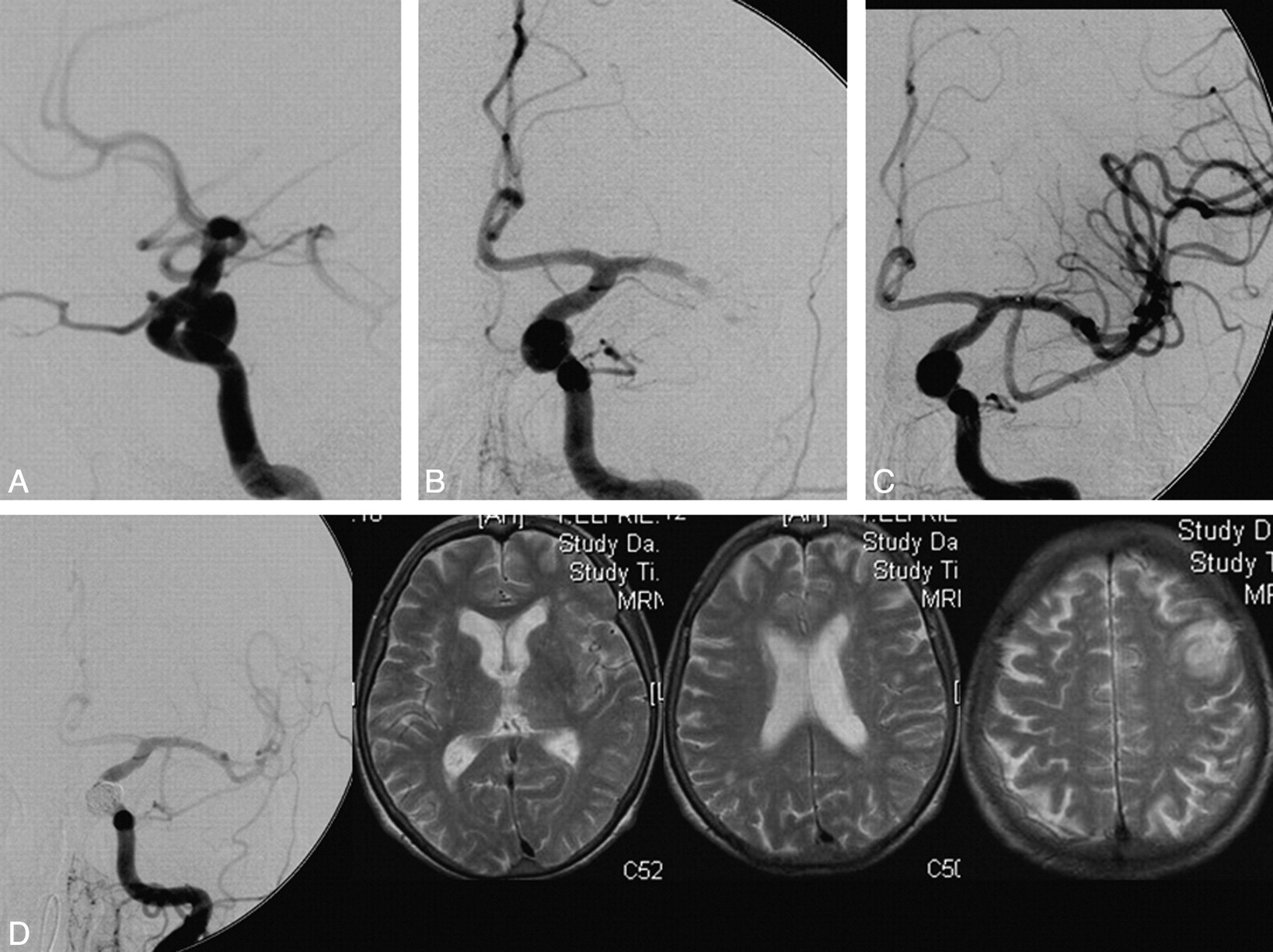
This patient was a 73-year-old woman with an incidental 7-mm aneurysm at the left ICA (Fig 3A). The patient was treated in October 2002. After insertion of the guiding catheter, a thrombotic occlusion of the left MCA occurred (Fig 3B). Therefore, the patient was first treated with local thrombolytic therapy (Fig 3C). After lysis of the thrombus, the aneurysm was coiled in a typical manner. The control DSA at the end of the procedure revealed a complete occlusion of the aneurysm and a regular perfusion of the left hemisphere (Fig 3D). The initial MR imaging examination 2 days after coiling did reveal a small infarct in the MCA territory (Fig 3D). The patient did not show any clinical symptoms and had a good recovery after 6 months of control.

A, DSA of a 73-year-old woman with an incidentally discovered aneurysm at the left ICA. B, After insertion of the guiding catheter, a thrombotic occlusion of the left MCA occurred. C, Therefore, the patient was first treated with local fibrinolysis therapy. D, Control DSA at the end of the coiling procedure revealed a complete occlusion of the aneurysm and a regular perfusion in the left hemisphere. The initial MR imaging 2 days after coiling did reveal a small infarct in the MCA territory.
Case 2.
A 70-year-old woman with an incidental 5-mm basilar tip aneurysm was admitted to our hospital. This aneurysm was wide necked (Fig 4A). Therefore, the endovascular procedure consisted of deployment of a Neuroform stent and subsequent coiling. Premedication was administered as usual. A small residual opacification was noted after treatment (Fig 4B). Follow-up angiogram after 6 months revealed subsequent thrombosis, resulting in a complete occlusion of the aneurysm and a stenosis in the distal part of the Neuroform stent without any clinical symptoms or hemodynamic relevance (Fig 4C).

A, DSA of 70-year-old woman with an incidentally discovered wide-necked basilar tip aneurysm. The endovascular procedure consisted of a Neuroform stent deployment and subsequent coiling. B, A small residual opacification was noted after the treatment. C, The follow-up angiogram after 6 months revealed subsequent thrombosis resulting in a complete occlusion of the aneurysm and in-stent stenosis of the P1 segment on the right.
Discussion
The literature reveals only few data about endovascular or surgical treatment of aneurysms in elderly patients. This study has to be divided into 2 aspects: first, treatment of unruptured aneurysms and, second, treatment of elderly patients with acute SAH.
The patient group with unruptured aneurysms was relatively small in this study (23/108). Therefore, a definite conclusion has to be drawn carefully. Four of these patients had thrombotic complications during the coiling procedure, 2 had small ischemic lesions on MR imaging examination, but none sustained permanent neurologic symptoms; these rates are not higher compared with other patient groups.12,13 Even therapeutic occlusion of the ICA in 1 patient was tolerated with a good clinical outcome. Overall, the endovascular treatment of unruptured aneurysms in elderly patients seems not to be associated with higher complication or failure rates compared with other patient groups.14,15 The occlusion rates were comparable with the known rates in other patient groups. Rates of technical failure range from 5.7% to 10% in the literature for a normal age distribution16 compared with a failure rate of 4% in our complete group.
These results in unruptured aneurysms could give an additional argument concerning the decision of elective aneurysm treatment in elderly patients. Together with known risk factors for bleeding, such as the size of the aneurysm and smoking as well as the assumed bleeding risk, the therapeutic procedure should be chosen individually for each patient. The cumulative bleeding rate in 10 years after diagnosis is 10.5%.17 Therefore, even for patients older than 65 years, this is a relevant risk for bleeding within the expected life span. The risk for bleeding dependent on the size of the aneurysm is given with 1.11 per mm aneurysmal diameter and the patient age at diagnosis inversely with 0.97 per year. Another significant risk factor for bleeding is the smoking status of the patients at the time of diagnosis. Other risk factors such as multiplicity of aneurysms and family history of bleeding are relevant for elderly patients as for the average population.18 The most relevant morbidity and mortality rates after SAH are related to rebleeding and vasospasm.19 As the incidence of vasospasm is reported to be increased in elderly patients, the prevention of SAH in this group is an important point.6 When all these analyses are taken together, the conclusion can be drawn that no patient should be excluded from treatment of an unruptured aneurysm because of age older than 65 years. When all risk factors are taken into account, an individual concept should be found. Because endovascular coil embolization of nonruptured aneurysms are associated with a 5% to 10% risk for morbidity and nearly zero mortality from the procedure, this therapy should be a good option.16,20
The patients with acute SAH included in this study presented with a range of HH scores between 1 and 5. Our results could not support the higher amount of higher HH grades in older patients.6 However, there are some restrictions concerning this point: the patients who died before undergoing a diagnostic DSA were not registered, and the number of patients with HH 5 was very small in our group.
In our series of 86 patients with acute SAH, a failure rate of 5% was found, which is comparable to other studies in younger populations.16 In 3 patients, the elongated and tortuous vessel anatomy led to a failure in catheterization of the aneurysm and is therefore an age-related factor. In 1 patient with an aneurysm involving the MCA, the coiling was not performed because of a flow reduction in an MCA branch after inserting a first coil into the aneurysm. This problem was not age related.
The complication of aneurysmal rupture is known to increase in patients treated after an acute SAH.21,22 There is no known correlation of procedural rupture and patient age so far, and our results do not indicate such a correlation.
An additional factor influencing the coiling procedure might be the vasospasm at the time of coiling. Again, this is not an age-related factor, and intra-arterial infusion of nimodipine or papaverine is used in other patient groups as well.23 Another problem of elderly patients with, say, atherosclerotic disease is the use of antiplatelet therapy.24 In our group, this medication did not affect clinical outcome. In our group, only 4 procedural aneurysmal ruptures occurred and led to a worsening of clinical symptoms in only 1 patient. There are some descriptions that outcome in elderly patients does not correlate with age but with the clinical HH grade.6 Our results support this finding: outcome of our patient group was associated with the HH grade but not with the age of the patients. However, this finding is true also for patient groups with an average distribution of age.25
Conservative treatment of ruptured aneurysms in elderly patients is known to be associated with a poor outcome.3 Some studies reveal a slightly better outcome after surgery4 or no change after clipping.5 Some recent studies revealed an independence rate of 33% to 54% in the follow-up of patients after clipping.25,26 Drawing conclusions about endovascular versus surgical treatment can be challenging because of evolving technology and changing indications for endovascular therapy, but the surgical therapy is generally reported to be associated with higher mortality and morbidity rates compared with endovascular procedures.27,28
Conclusion
Endovascular coil embolization can be performed safely and effectively in elderly patients. Endovascular embolization of unruptured intracranial aneurysms is an effective therapeutic tool in elderly patients with similar morbidity and mortality rates in the average population. Even older patients with acute SAH can be treated with endovascular therapy with an acceptable outcome.
Acknowledgments
We thank Dr. Susanne Ladd for her help with the statistical calculations.
References
- Received February 11, 2008.
- Accepted after revision April 16, 2008.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Elderly patients with intracranial aneurysms have higher quality of life after coil embolization: a decision analysis
- Endovascular Treatment of Intracranial Aneurysms in Elderly Patients: A Systematic Review and Meta-Analysis
- Perioperative safety of Hydrosoft coils
- Age-Related Complications following Endovascular Treatment of Unruptured Intracranial Aneurysms
- Endovascular treatment of unruptured intracranial aneurysms in the elderly: analysis of procedure related complications