
Abstract
SUMMARY: Brown syndrome describes the inability of a patient to perform an upward gaze while the eye is adducted due to an abnormality of the superior oblique tendon sheath complex. Use of CT in diagnosing the condition has been reported; however, the use of MR imaging has not. We describe a unique case of Brown syndrome in which the initial CT findings were normal, but MR imaging revealed the abnormality. Key imaging features are illustrated.
Brown syndrome is characterized by the inability to gaze upward beyond the horizontal level while adducting the eye due to an abnormality of the superior oblique tendon sheath complex.1
The course of the superior oblique tendon can be demonstrated on axial CT images. CT is unable to resolve fully the different components of the trochlea area; however, the combined structures are discernible (Fig 1). Axial MR imaging offers even less resolution, and both coronal CT and MR imaging allow visualization of only portions of the muscle belly (Fig 2).

Axial CT scan of the orbits demonstrates the course of the superior oblique muscle/tendon. The muscle extends anteriorly to the superomedial corner of the orbit (white arrowhead). Here it reaches the trochlea (black arrow), a fibrocartilaginous structure lying deep within the orbital fascia. Just before reaching the trochlea, the muscle becomes tendinous, and while passing through it, the tendon is compressed into a fibrous cord. Exiting the trochlea, the tendon runs inferiorly, posteriorly, and laterally (white arrow) to insert into the posterolateral portion of the sclera.

Coronal T1-weighted MR image of the orbits demonstrates the extraocular muscles in relation to the optic nerve: superior rectus (s), lateral rectus (l), medial rectus (m), inferior rectus (i), superior oblique (so), and optic nerve (on).
CT characteristics of the condition have been described and include thickening of the tendon, often the reflected portion following passage through the trochlea.2 This feature was not discernible on the CT performed on our patient. Conversely, MR imaging confirmed the diagnosis. This unique case describes the salient features of acquired Brown syndrome on MR imaging and highlights the use of MR imaging as a diagnostic tool when CT findings are negative.
Case Report
A 46-year-old woman with known systemiclupus erythematosis (SLE) presented acutely with a 2-week history of severe headache associated with vertical double vision, particularly in an upward gaze to the left. She experienced tenderness to palpation over the right trochlea region.
Laboratory values for blood tests, including full blood count, urea and electrolytes, plasma glucose, immunoglobulins, serum complement, antineutrophil cytoplasmic antibody, and cardiolipin antibodies were normal. The antinuclear antibody-2 test was positive, but retrospective review of her blood results showed that this had been positive during a 4-year period before this presentation and was attributable to SLE.
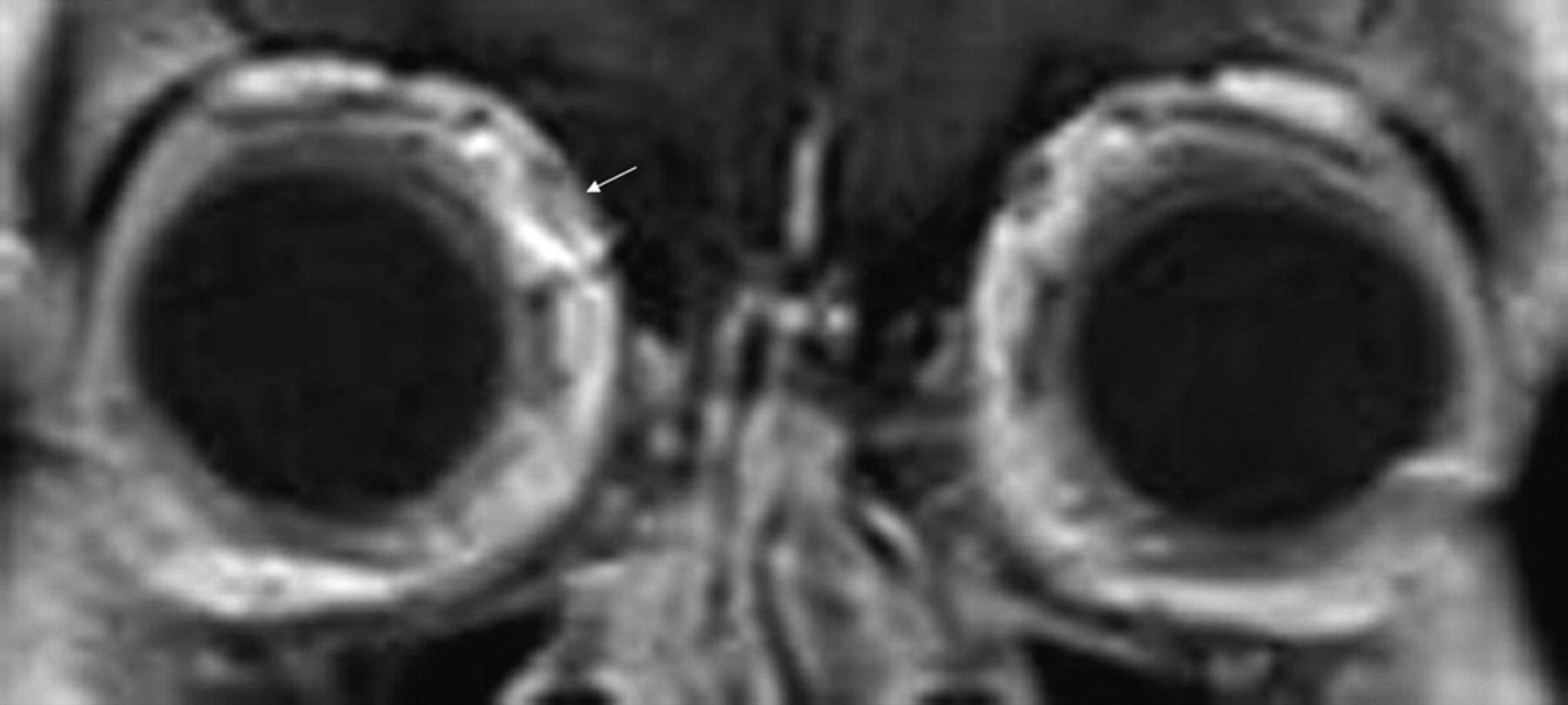
CT head imaging findings with and without contrast were normal (Fig 3). MR imaging of the brain showed no intracranial abnormality. However, the right superior oblique tendon was abnormally thickened on T1-weighted imaging (Fig 4) and of abnormally high signal intensity on T2-weighted fat-saturated imaging (Fig 5) and demonstrated mild enhancement after administration of gadolinium (Fig 6).

Axial CT scan of the patient's orbits shows no discernable difference between the appearances of both superior oblique tendons (white arrows).
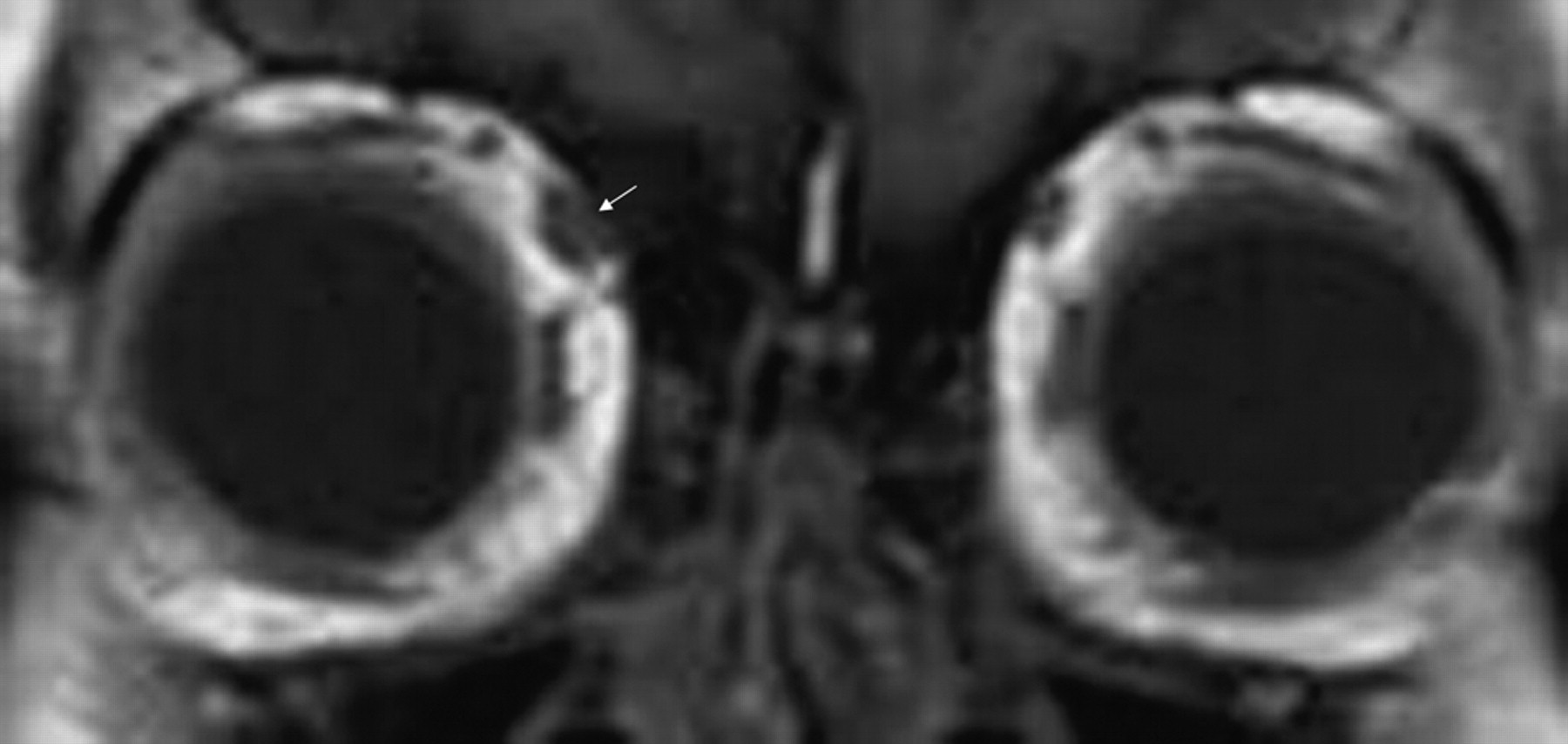
Coronal T1-weighted MR image shows abnormal asymmetric thickening of the right superior oblique tendon (white arrow).

Coronal T2-weighted fat-saturated MR image shows abnormal high signal intensity in the right superior oblique tendon.

Coronal T1-weighted gadolinium-enhanced MR image shows mild abnormal enhancement of the right superior oblique tendon.
The diagnosis of inflammatory Brown syndrome was made, and she was treated with an initial 2-week course of 50-mg flurbiprofen 3 times a day and was given a frosted lens to aid her double vision. On 2-week review, her symptoms had improved, though she continued to have vertical double vision, particularly in her left gaze. She was prescribed a further 4-week course of flurbiprofen and is currently awaiting review in 6 weeks.
Discussion
Brown described the syndrome in 1950 and classified its etiology into true (congenital) and simulated (acquired) types.1 Congenital Brown syndrome is seen in those patients with a congenitally short or taut superior oblique tendon sheath complex. The acquired form replicates the clinical presentation of its congenital counterpart and differs only in its cause.2 Pathology commonly reveals swelling of the tendon associated with thickening of the sheath, and it has been postulated that the acquired form primarily involves the posterior fascia and tendon as a result of an inflammatory process.3 Various acquired causes have been reported, including rheumatoid arthritis,4 scleritis, systemic lupus erythematosus, trauma,5 and sinusitis6 and following peribulbar anesthetic injection.7
Previous reports have illustrated the use of CT as a valuable tool in assessing Brown syndrome.2 Imaging reveals thickening of the reflected portion of the superior oblique tendon, which may be accompanied by localized low attenuation representing edema. These features were not clearly present on the CT images of our patient.
To our knowledge, the features of the disease on MR imaging have yet to be described in the literature. This case clearly demonstrated abnormal thickening of the tendon on T1-weighted imaging, abnormal high signal intensity on T2-weighted fat suppression, and abnormal enhancement on T1-weighted gadolinium-enhanced imaging. These findings support an inflammatory and edematous pathologic process. SLE is a known cause of acquired Brown syndrome, and the patient's symptoms improved with nonsteroidal anti-inflammatory therapy. The literature supports conservative management of acquired Brown syndrome because the results of surgery to reduce the tethering caused by scarring in the region of the trochlea are generally disappointing.5
This case shows that MR imaging can play an important role in the identification of Brown syndrome and should be considered in cases where CT fails to confirm the abnormality.
- Received January 30, 2009.
- Accepted after revision February 7, 2009.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.