
Abstract
BACKGROUND AND PURPOSE: Important findings, such as aneurysm remnants or major arterial occlusion, can be detected on intra- or postoperative angiography after surgical clipping of intracranial aneurysms. The purpose of this study was to evaluate the feasibility of IV-ACT for the postoperative detection of residual aneurysms and parent vessel patency compared with IA-DSA, which was selected as the standard reference method.
MATERIALS AND METHODS: Twenty-two patients with 27 aneurysms treated by surgical clipping were examined by using both IA-DSA and IV-ACT. Both diagnostic procedures were performed on an FPD-equipped angiography system. Postprocessing of IV-ACT acquisitions was performed on a dedicated workstation producing multiplanar reformations and maximum intensity projections of the clip region and other intracranial arteries. Three interventional neuroradiologists independently evaluated both procedures.
RESULTS: A residual aneurysm was delineated in 10 cases with IA-DSA. Sufficient opacification of the intracranial vessels was assigned in 26 IV-ACT cases. Due to metal artifacts, IV-ACT images were tagged as “not diagnostic” on 8 occasions. In the other 19 aneurysms, a residual aneurysm was delineated in 6 cases—all 6 being true-positive compared with IA-DSA—and was excluded in the remaining 13 cases—all true-negative. Even small aneurysm remnants with a diameter of 1.5 mm were detected with IV-ACT.
CONCLUSIONS: Currently IV-ACT cannot be recommended as a routine tool for postoperative evaluation of clipped aneurysms due to metal artifacts in 30% of the examinations. These artifacts appear with multiple normal-sized or large clips. In patients with single or multiple small clips, IV-ACT can reliably show aneurysm remnants.
Abbreviations
- ACT
- flat-panel angiographic CT
- CI
- confidence interval
- CTA
- CT angiography
- CTDIw
- weighted CT dose index
- DSA
- digital subtraction angiography
- FPD
- flat panel detector
- IA
- intra-arterial
- IV-ACT
- flat panel CTA after intravenous contrast agent application
- MDCTA
- multidetector row CT angiography
- MRA
- MR angiography
Surgical clipping of intracranial aneurysms is a widely used treatment for both ruptured and unruptured aneurysms. There are several studies suggesting that important findings such as major arterial occlusion or narrowing as well as residual aneurysm can be detected on routine postoperative angiography, often even to the surprise of the operating surgeon, therefore emphasizing the importance of intra- or postoperative vessel delineation after clipping of intracranial aneurysms.1–5 In various studies, the percentage of neck remnants ranges from 4% to 18%.5,6 Long-term follow-up data of clipped aneurysms also suggest that there is a risk of de novo appearance of new aneurysms and regrowth of previously treated aneurysms.7–9
DSA with the addition of 3D subtraction angiography is still considered the criterion standard for the depiction of postoperative vascular complications or aneurysm remnants. Thus, all studies validating new noninvasive methods of intracranial angiography correlate their results with those of IA-DSA series.10–12 The invasive character of IA-DSA, with possible permanent neurologic complications, and the fact that it is a time-consuming and expensive examination have led to the development of new noninvasive methods.13
MRA is a viable option for screening intracranial aneurysms, but in the postoperative setting, it has limitations due to the substantial artifacts created around the surgical clip, even with adjustments to MRA parameters such as TE.14 With the advances in scanner technology, modern reconstruction, and artifacts-reduction techniques, CTA is also emerging as a noninvasive examination for the delineation of cerebral vessels after surgical clipping.11,15,16 Again, the size of the neck remnant or the number of the implanted clips can limit the sensitivity of MDCTA.15,17–19
A new noninvasive technique for the depiction of the intracranial vasculature is IV-ACT—also known as flat detector CT or C-arm conebeam CT after intravenous contrast agent application. Based on the development of the FPD, it is an examination with characteristics similar to those of MDCTA20 but is performed in the angiography suite. High contrast resolution is close to the contrast resolution of MDCTA.21,22 The noteworthy aspect, compared with MDCTA, is the superior spatial resolution, with an isotropic voxel size of ≤0.15 mm3. Recent studies have shown the potential of IV-ACT in the delineation of even small-sized (2- or 3-mm diameter) intracranial stents and the accurate depiction of in-stent restenosis, compared with IA-DSA.23 In the postcoiling evaluation of intracranial aneurysms, ACT proved to be a useful addition to conventional IA-DSA.24 The ability of ACT to produce thin cross-sectional images with approximately 0.2-mm section thickness is also valuable in the characterization of spinal dural arteriovenous fistulas.25 Recently, Wachter et al26 published a small series of patients who underwent postoperative IV-ACT as an alternative to IA-DSA for noninvasive follow-up of surgically treated aneurysms.
The purpose of this study was to evaluate the feasibility and accuracy of IV-ACT in the postoperative detection of residual aneurysms and parent vessel patency compared with IA-DSA.
Materials and Methods
Patients
Twenty-two patients with 27 aneurysms were selected after surgical clipping from January 2009 to February 2010 (15 women, 7 men; mean age, 56 years; range, 28–76 years). In all cases, the surgeon was not confident about the position of the clip. Of the 27 aneurysms, 5 were located in the distal segment of the internal carotid artery; 3, in the intracranial carotid bifurcation; 1, in the proximal segment of the middle cerebral artery; 15, in the middle cerebral artery bifurcation; 2, in the proximal segment of the anterior cerebral artery; and 1, in the intracranial segment of the vertebral artery. Prior rupture with consecutive subarachnoid hemorrhage had been detected in 15 of the operated aneurysms, while 12 cases were incidental aneurysms. Eleven aneurysms were treated with a single clip; 13, with 2 clips; and 3 aneurysms required 3 surgical clips each. All clips were made of titanium (Yasargil; Aesculap, Tuttlingen, Germany). Cobalt clips were not an exclusion criterion for the study. Regarding the size of the implanted clips, 3 aneurysms were treated with miniclips (blade length, 3–5 mm); 17 aneurysms, with normal-sized clips (blade length, 5–20 mm); 6, by using oversized clips with a blade length >20 mm; and 1 aneurysm, with a fenestrated clip. All patients were admitted for postsurgical evaluation within an average of 5 days (range, 1–23 days) after surgery.
Approval of the local ethics committee and informed patient consent were obtained.
Image Acquisition
Both IV-ACT and IA-DSA acquisitions were performed on a biplane angiography system equipped with an FPD (Axiom Artis dBA; Siemens, Erlangen, Germany). Routinely, a transfemoral access was used for IA-DSA. Dedicated focused views were obtained when aneurysm remnants were suspected on standard projections. DSA series were processed by standard optimization of the mask images and pixel shifting. For the acquisition of IV-ACT, we used the DynaCT (Siemens) protocol in the angiography suite with the following parameters: 20 seconds of rotation; ∼500 projections; 220° total angle; CTDIw, approximately 35 mGy (manufacturer's information); a 30 × 40 cm detector, permitting the reconstruction of a nontruncated volume of approximately 22 cm (in-plane) and 16 cm (in the z-direction).
For planning purposes, the clipped aneurysm was placed near the center of the FOV, because a higher image quality can be achieved near the center of the conebeam.27 However, we avoided placing the clip exactly in the center of the FOV because ring artifacts can negatively affect the image quality.28 Before image acquisition, 80 mL of iomeprol (Imeron 400; Bracco Altana Pharma, Konstanz, Germany) was injected into a cubital vein at a flow rate of 5 mL/s by using a power injector, followed by 40 mL of saline flush. Due to the lack of automated triggering software, we used standard fluoroscopy images before acquisition of IV-ACT to track the contrast agent bolus. The time delay between triggering and the onset of data acquisition was approximately 1 second. During IV-ACT, patients were requested to close their eyes and to breath-hold during the 20 seconds of the C-arm rotation. Postprocessing of the rotational image data to a volume dataset was performed by using dedicated commercial software on a syngo X Workplace (In Space, syngo XWP, VD13f, Siemens). The software includes system-specific algorithms to correct beam-hardening, scattered radiation, truncated projections, and ring artifacts. Reconstruction resulted in a volume dataset of approximately 400 sections with a 512 × 512 matrix and an isotropic spatial resolution of approximately 0.2 × 0.2 × 0.2 mm.
Image Analysis
Three neuroradiologists (M.K., A.M., M.-N.P.) independently performed the image viewing and rating on the above-mentioned syngo X Workplace medical workstation to allow interactive reconstruction and interpretation. Two of the raters are experts in the field of neuroradiology (M.K., A.M.), while the third has experience with both procedures. Raters were blinded to surgical information and preoperative MDCTA or IA-DSA results. In a first session, anonymized IV-ACTs were rated regarding the depiction of neck remnants or incomplete clipping and the detection of parent vessel stenosis/occlusion after clipping by using the following scoring system: 1 = positive answer; 2 = negative answer; and 3 = images not diagnostic due to metal/other artifacts. With the help of a 4-step ordinal system (1 = excellent; 2 = good; 3 = limited; 4 = impossible), raters were asked to evaluate IV-ACT examinations with respect to delineation of the parent vessel and other intracranial vessels (eg, for the detection of vasospasms). To minimize recall bias, raters continued with the evaluation of the anonymized and randomized IA-DSA images 2 weeks later. In a third step and while studying simultaneously IV-ACT and IA-DSA images, raters suggested which was the superior technique for the diagnosis or exclusion of an aneurysm remnant in the respective cases and whether they could have diagnosed the aneurysm remnant by solely viewing IV-ACT images. Additionally, raters were asked whether the intracranial vessels were sufficiently opacified on IV-ACT and whether the IA-DSA projections were adequate for the depiction of the clipped segment and the parent vessel.
Statistical Analysis
At first, the mode (ie, the most frequent value) of the raters' judgments was determined for each aneurysm. Regarding complete aneurysm occlusion after clipping and parent vessel patency, the accordance of IV-ACT with IA-DSA was assessed by sensitivity and specificity as well as by the positive and negative predictive values (including 95% CIs).
The influence of the number and size of the clips on the occurrence of artifacts and the influence of clip size on the inability to make the diagnosis solely on IV-ACT were assessed by using logistic regression. The correlation of artifacts and aneurysm location was calculated by using the Fisher exact test. The ability to depict the parent vessel as well as the rest of the intracranial vasculature was compared between IV-ACT and IA-DSA by the Mann-Whitney U test. All tests were performed at a significance level of P = 5%.
Interobserver agreement was evaluated by using κ statistics and their 95% CIs. Values of >1 indicated an agreement larger than chance. All analyses were performed by using the free software R (version 2.8, www.r-project.org).
Results
Postsurgical evaluation after clipping was obtained for 27 intracranial aneurysms. There were no thromboembolic events documented during IA-DSA studies. All IA-DSA series (100%) were characterized as adequate for the depiction of the clipped aneurysm or the delineation of the parent vessel. There was no major vessel occlusion detected on IA-DSA after clipping; only 1 (4%) moderate parent vessel stenosis was found on IA-DSA. Regarding the delineation of residual aneurysms, a positive answer was given in 10 (37%) of the examined aneurysms: In 4 cases, large neck remnants were identified; in another 4 cases, the remnant was classified as “dog ear”; and finally, 2 aneurysms were rated as incompletely clipped. The average remnant size was 3 mm, with the biggest residual aneurysm detected measuring 8 mm. In the remaining 17 cases, there was no evidence of residual aneurysm on IA-DSA images. Twenty-four (89%) and 27 (100%) of the IA-DSA series were described as excellent for the depiction of the parent vessel and the rest of the intracranial vessels (eg, for the detection of vasospasm) respectively. In only 3 cases did raters classify IA-DSA images as good.
IV-ACT was well-tolerated by all patients, with no motion artifacts being detected in the examined series. Sufficient opacification of the intracranial vessels was assigned in 26 of 27 cases (96%). Due to extensive metal artifacts, IV-ACT images were rated as not diagnostic in 8 cases (30%). In the remaining 19 operated aneurysms (70%), a residual aneurysm was found in 6 cases (32%)—with all 6 being true-positive compared with the criterion standard IA-DSA—and was excluded in the remaining 13 cases (68%)—again all being true-negative (Figs 1⇓–3). Thus, in comparison with the criterion standard IA-DSA, a 100% sensitivity (95% CI, 54%–100%) and 100% specificity (95% CI, 75%–100%) could be ascribed to the 19 cases in which metal artifacts did not negatively affect image quality in IV-ACT. Even small aneurysm remnants with a diameter of 1.5 mm could be identified with IV-ACT (Fig 2B, black arrow).

A, Rotational angiogram of a 41-year-old woman with a saccular aneurysm of the left internal carotid artery. B and C, After surgical clipping, IV-ACT multiplanar reformations (B) and 3D volume-rendering IV-ACT reconstructions (C) depict an incomplete occlusion of the aneurysm. D, Lateral IA-DSA series confirm this finding.

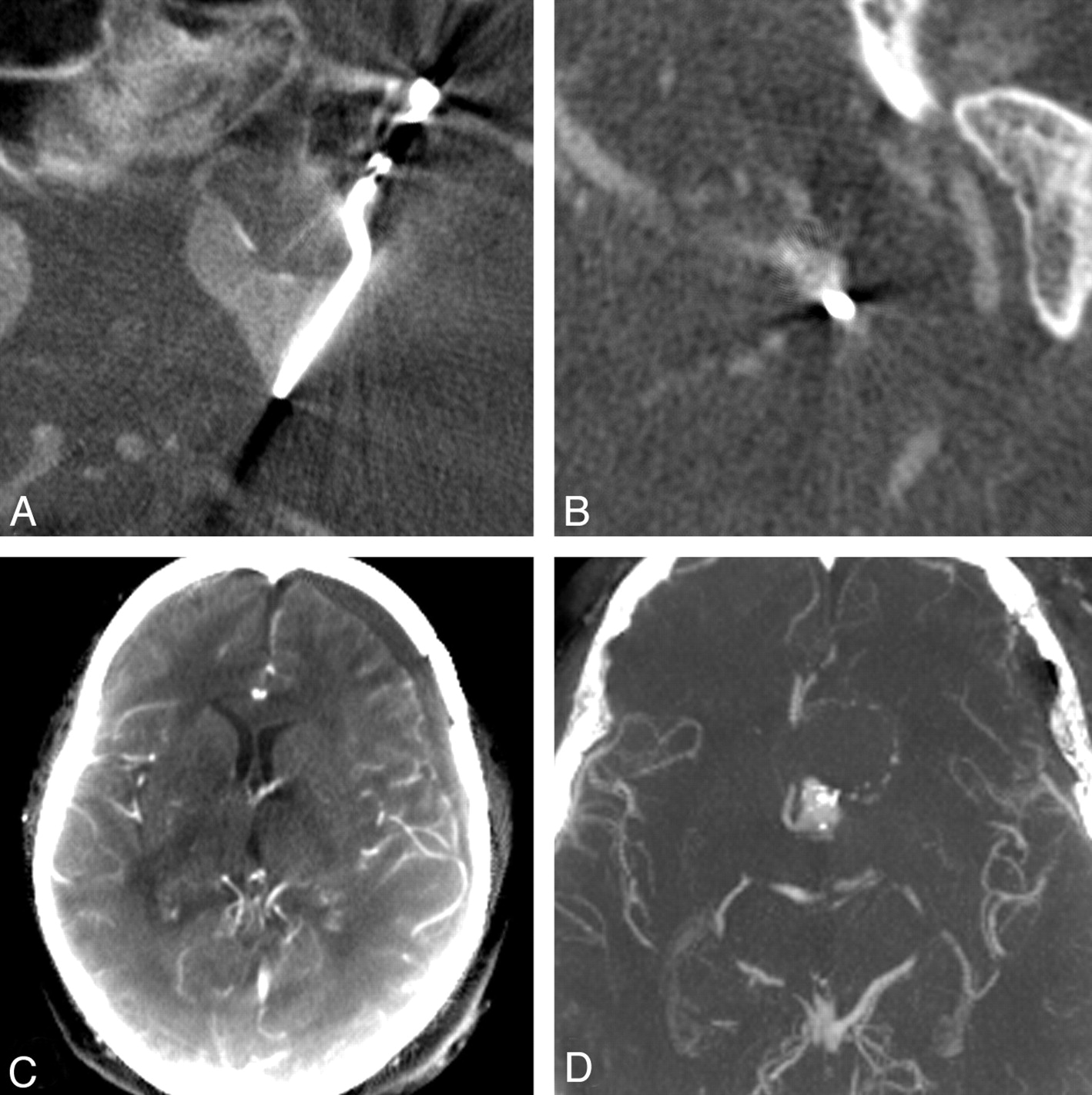
A, In another example, a middle cerebral artery bifurcation aneurysm was treated with 2 normal-sized clips. B, Coronal IV-ACT maximum intensity projection of the clipped aneurysm with a section thickness of 1 mm delineates a very small aneurysm remnant (black arrow) with a diameter of 1.5 mm. C and D, Again, raters could also detect the aneurysm remnant on anteroposterior IA-DSA images (C, small black arrow) and dual-volume 3D volume-rendering rotational angiography reconstructions (D).

Complete occlusion of an unruptured internal carotid artery aneurysm arising from the origin of the left posterior communicating artery. The 71-year-old-man underwent preoperative rotational angiography (A) and postoperative evaluation of the aneurysm with IV-ACT (B and C) and IA-DSA (D). Complete occlusion of the aneurysm and parent vessel patency can be diagnosed on both examinations.
Relevant metal artifacts mainly consisted of typical image degradation in continuation of the long axis of the clip in 5 cases in which the clip was implanted parallel to the rotational plane of the conebeam. In 3 IV-ACT series, in which the clip was localized perpendicular to the scanning plane, streak artifacts around the clip blade obscured the surrounding brain and vessels (Fig 4 ). In addition, all 11 IV-ACT series involving aneurysms with 1 clip showed no relevant image degradation, contrary to images with 2 or 3 clips, in which substantial image degradation was detected in 6 of 13 cases (46%) and 2 of 3 of the cases (67%), respectively (P < .03). Clip size was also significantly related to extensive metal artifacts around the clipped aneurysm (P < .05) (eg, miniclips had no significant effect on image degradation, while oversized clips produced extensive artifacts in 5 cases [83% of the cases in which an oversized clip was implanted]). The location of the clipped aneurysm had no significant influence on image degradation (P = .10). Regarding the patency of the parent vessel, raters correctly ruled out a stenosis or occlusion of the parent vessel in 16 cases (59%). However, raters tagged 11 IV-ACT cases (41%) as not diagnostic, thus not being able to detect the 1 stenosis seen on IA-DSA. Consequently, in the descriptive evaluation of the parent vessel delineation, IV-ACT was significantly worse compared with IA-DSA (P < .01), with only 4 cases (15%) described as excellent; 11 cases (41%), as good; 5 cases (18%), as limited; and in another 7 cases (26%) a classification was impossible with IV-ACT. Regarding the assessment of the rest of the intracranial vasculature, an excellent was given in 18 IV-ACT cases, while the remaining 8 acquisitions were described as good. This assessment was significantly worse compared with IA-DSA, in which classification was excellent in all 27 cases (P < .01).

A, Typical metal artifacts along the long axis of the clip are delineated in multiplanar reformations of IV-ACT examinations. Note that such artifacts are detected when the long axis of the clip is oriented parallel to the rotational plane of the C-arm. B, In cases in which the long axis of the clip lies perpendicular to the rotational plane, streak artifacts around the blade of the clip are common. C, Multiplanar IV-ACT reformations of the whole brain are adequate for the postoperative diagnosis of a left frontal hygroma—an advantage of IV-ACT compared with IA-DSA. D, Maximum intensity projections of IV-ACT allow the diagnosis of aneurysms on other vascular territories.
In the last section of our questionnaire, raters were asked to choose the superior examination for the detection or exclusion of aneurysm remnants and to decide whether they could have made a correct diagnosis only by viewing the IV-ACT images. In 14 cases (52%), the 2 methods were described as equal; in 12 cases (44%), IA-DSA was considered superior to IV-ACT; and in 1 case (4%) in which a fenestrated clip was implanted, IV-ACT was rated as superior to IA-DSA. Moreover, raters suggested that they could have made the right diagnosis only with IV-ACT in 18 of the clipped aneurysms (67% of the overall population; ie, 95% of the group without relevant metal artifacts). A negative answer was given in 9 cases (33%), with 8 of these being occasions where extensive metal artifacts resulted in significant image degradation around the implanted clips. In addition, the relation of clip size and the inability to make the diagnosis solely on IV-ACT series due to artifacts tended to be significant (P = .06) (eg, in the group in which oversized clips [>20 mm] were implanted, raters could have made the diagnosis solely on IV-ACT images in only 17% of the cases).
Analysis of interobserver agreement regarding the ratings in the category “detection of aneurysm remnant” resulted in κ = 0.78 (95% CI, 0.53–1.04) for IV-ACT and κ = 0.90 (95% CI, 0.68–1.11) for IA-DSA. Regarding parent vessel patency, the interobserver agreement was κ = 0.61 (95% CI, 0.35–0.87) for IV-ACT and κ = 0.56 (95% CI, 0.28–0.83) for IA-DSA. Thus, interobserver agreement was significantly larger than chance agreement.
Discussion
Incomplete surgical treatment of an intracranial aneurysm may lead to regrowth and recurrent symptoms of hemorrhage or mass effect. The percentage of neck remnants documented in the literature ranged from 4% to 18%,5,6 with the rebleed rate after clip ligation ranging from 3% to 5% in recent studies.29,30 Several research articles supported the fact that incomplete occlusion of operated aneurysms or other major findings, such as parent artery stenosis or occlusion, can be, even unexpectedly, detected on routine postoperative angiography, thus emphasizing the importance of intra- or postoperative imaging after surgical clipping.1–5 Nevertheless, current clinical convention holds that intra- or postoperative angiography be used on a selective basis for complex aneurysms when the surgeon is not confident of the outcome of the operation, though prospective studies have documented that even experienced surgeons cannot accurately predict the necessity of intraoperative angiography.4 The most likely reason for this discrepancy, besides its invasive nature, has to lie in the time-consuming and resource-intensive character of IA-DSA.
On the other hand, noninvasive techniques such as MR imaging and CTA are currently increasingly being used for the postoperative assessment of clipped aneurysms. MRA is substantially limited due to artifacts around the clip—even with modifications in MR imaging parameters.14 MDCTA studies have documented high sensitivity and specificity rates in the diagnosis of neck remnants, compared with IA-DSA.11,15,16 Dehdashti et al16 demonstrated, in a series of 60 clipped aneurysms with 90% of the cases being treated with a single clip, a 100% sensitivity and specificity for detecting neck remnants and an 80% sensitivity with 100% specificity for evaluating vessel patency. Gerardin et al19 examined a population with significantly more clips per aneurysm and found lower sensitivity and specificity values, concluding that MDCTA is a valuable examination for aneurysm remnants with a diameter of >2 mm.
IV-ACT is a method based on the development and use of FPD in angiographic suites. Imaging characteristics (eg, contrast resolution) are similar to those of MDCTA, especially in the higher range, but the use of a FPD allows volume datasets with superior and isotropic spatial resolution of up to 0.1 mm3.21,27 In our study, IV-ACT demonstrated high sensitivity and specificity for the detection of aneurysm remnants compared with IA-DSA in those cases in which image quality was not degraded due to metal artifacts. Even small 1.5-mm remnants could be detected with IV-ACT (Fig 2). Additionally, being a volume dataset, IV-ACT has apparent advantages over IA-DSA in the postoperative setting because not only can the intracranial vasculature be delineated but multiplanar reformations of the cerebral parenchyma can also be extracted from the same dataset; this procedure helps with the detection of postoperative hygroma or hemorrhage (Fig 4C). In long term follow-up, IV-ACT can be used to identify not only regrowth of previously treated aneurysms but also de novo formation of aneurysms at other sites of the cerebral vasculature after a single administration of contrast agent (Fig 4D), whereas a complete 4-vessel IA-DSA would be necessary for the same purpose.31 Moreover, IV-ACT becomes more and more attractive with the increased use of combined FPD angiography suites in fully equipped operating theaters because a noninvasive examination will be available for intraoperative imaging.32,33 Schaller et al33 performed intraoperative 3D rotational angiography 54 times in 42 patients, with repositioning of surgical clips in 9 patients. With the establishment of IV-ACT, these intraoperative control examinations could be performed with a noninvasive tool.
Another not-so-obvious aspect of IV-ACT in comparison with MDCTA is the availability of angiography suites for such examinations. In our department, for example, there are 2 shifts working nonstop on the CT scanner from 8 am till 10 pm with a high load of patients. On the other hand, the angiography suites are mainly being occupied until 2 or 3 pm for diagnostic angiographies and endovascular interventions with free slots thereafter for examinations such as IV-ACT. Given the lack of CT scanners in some European countries such as France or Portugal, this availability may be a relevant administrative fact.34
Regarding the IV-ACT images tagged as not diagnostic, the effect of multiple clips as well as clip size on image quality is important. Contrary to the authors in an above-mentioned MDCTA study,16 we did not exclude series with significant artifacts from our evaluation, to assess the effect of clip number and size on image quality. For clinical practice, single clips, even when oversized, did not negatively affect image quality. Also miniclips, even in numbers, did not lead to classifying an IV-ACT image as not diagnostic. On the other hand, multiple oversized clips produced substantial artifacts on every single occasion. Maybe, with the development of new metal artifacts-reduction algorithms for IV-ACT as described by Prell et al,35 the delineation of an aneurysm remnant after clipping with multiple large clips will be possible in the near future, but with the current state of the technique, it is impossible to diagnose an aneurysm remnant in these cases.
Concerning the radiation dose, the use of a 20-second ACT protocol results in a CTDIw value of ∼35 mGy, which is comparable with or even lower than the usual MDCTA or conventional cranial CT protocols (∼50–60 mGy).36,37 In contrast to other studies that have used a high-dose 20-second ACT protocol with a CTDIw of ∼75 mGy, we used the low-dose protocol solely in our study.38
The amount of contrast media injected for IV-ACT in our study was slightly higher than the amount being used in a conventional MDCTA (60 mL in our department). The reason for this difference is the necessity of a longer acquisition time with the ACT protocol. The radiation and contrast agent dose could be further reduced with the application of a 5-second (CTDIw ∼ 9 mGy)38 or an 8-second ACT protocol (cumulative incident dose, 15 mGy; reference value for a single biplane IA-DSA series, 53 mGy),39 but neither of these acquisitions provide a sufficient image quality for different reasons. In vitro, we are currently testing a 10-second dual-rotation protocol, which allows the acquisition of subtracted images during the injection of the contrast agent for better tracking of the contrast agent bolus and has image characteristics similar to those of the 20-second DynaCT. Furthermore, with the implementation of novel imaging techniques for FPD angiography suites in the near future, like the volume-of-interest imaging method proposed by Kolditz et al,40 high image quality will be guaranteed within the volume of interest, while simultaneously reducing the cumulative patient dose.
There are several limitations to our study. Because of the specific inclusion criteria, the population we examined had a high prevalence of aneurysm remnants (37%), contrary to other studies in which the incidence of residua was estimated to range between 4% and 18%.1,41 This bias may have led to an apparent increase in the sensitivity and specificity of IV-ACT.42 Moreover, our results apply to patients treated with titanium clips, which are known to produce fewer metal artifacts in CTA than cobalt-containing alloy clips.43 This means that the use of IV-ACT in patients with cobalt-containing alloy clips may be limited. The use of a 20-second rotation protocol for IV-ACT means that venous contamination cannot be prevented, even with exact tracking of the contrast agent bolus. Finally, the small sample size of our study is another limiting factor; however, the fact that our sample size was quite small and nonetheless still displayed positive results means that further research is indicated.
Conclusions
Currently, IV-ACT cannot be recommended as a routine tool for postoperative evaluation of clipped aneurysms due to metal artifacts in 30% of the examinations. These artifacts appear with multiple normal-sized or large clips. In patients with single or multiple small clips, IV-ACT can reliably show aneurysm remnants. With advances in the FPD technique, like the introduction of new metal artifacts-reduction algorithms or the volume-of-interest imaging method, as well as the increased use of combined angiography suites in fully equipped operating theaters, IV-ACT may become a viable follow-up method after aneurysm clipping. Further research is warranted.
Footnotes
M.-N. Psychogios and D. Wachter contributed equally to this article.
References
- Received November 18, 2010.
- Accepted after revision February 20, 2011.
- © 2011 by American Journal of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
{kind=link}