
Abstract
SUMMARY: We report a case of severe RCVS treated with a combination of selective intra-arterial verapamil infusions and intracranial angioplasty, resulting in angiographic and clinical improvement. Endovascular techniques more commonly used in the treatment of SAH-induced vasospasm are potentially important adjuncts to systemic drug therapy in the management of severe RCVS.
Abbreviations
- ACA
- anterior cerebral artery
- CNS
- central nervous system
- FLAIR
- fluid-attenuated inversion recovery
- ICA
- internal carotid artery
- MCA
- middle cerebral artery
- MRA
- MR angiography
- PCA
- posterior cerebral artery
- PRES
- posterior reversible encephalopathy syndrome
- PTA
- percutaneous transluminal angioplasty
- RCVS
- reversible cerebral vasoconstriction syndrome
- SAH
- subarachnoid hemorrhage
RCVS is a rare syndrome characterized by sudden-onset thunderclap headache and focal neurologic deficits, most commonly in women 20–50 years of age.1,2 The common finding is diffuse segmental cerebral vasoconstriction of the intracranial ICAs, basilar artery, and major arteries of the circle of Willis that is spontaneously reversible in weeks to months.2 Different names are given to this syndrome according to clinical context: Call-Fleming syndrome,2 benign angiopathy of the CNS,3 postpartum angiopathy,4 thunderclap headache with reversible vasospasm,5 migrainous vasospasm or angiitis,6 and drug-induced cerebral arteritis or angiopathy.7,8
We report a case of pseudoephedrine-associated severe RCVS in which the patient developed profound neurologic deficits. Prompt angiographic reversal of vasoconstriction was achieved with intra-arterial verapamil infusion and PTA. Clinical deficits improved following endovascular therapy.
Case Report
A 53-year-old woman experienced several days of afebrile cough, sore throat, and nasal discharge, similar in nature to a viral syndrome experienced by her husband several days earlier. The patient developed a severe fluctuating headache on the third day of her symptoms, also following 3 days of pseudoephedrine-containing cold medicine use. Her initial headache was associated with fatigue, nausea, and vomiting. She had no other medical history, no substance abuse history, and took hormone replacement. She presented to an outside hospital on illness day 3 with systolic blood pressure >200 mm Hg. MR imaging and MRA of the brain were performed (Fig 1 A−D), yielding a provisional diagnosis of PRES. Diffusion-weighted images were not obtained at the time of the initial MR imaging.

A, On day 9 of illness, MRA of the circle of Willis demonstrates normal caliber of the ICAs, MCAs, ACAs, and vertebrobasilar system. B−D, At the same time, FLAIR shows bilateral parieto-occipital white matter edema, leading to an initial diagnosis of PRES. E−H, FLAIR MR imaging on illness day 19 shows progressive edema involving the occipital, parietal, and paramedian posterior frontal lobes. I−P, Diffusion-weighted imaging (I−L) and concomitant apparent diffusion coefficient maps (M−P) on illness day 19 confirm extensive infarction in the occipital, parietal, and paramedian posterior frontal lobes, corresponding to almost the entire extent of FLAIR abnormality.
The patient's headaches and hypertension persisted despite antihypertensive therapy. On illness day 9, she developed cortical blindness, right hemiparesis, and paresthesias. The patient became less responsive and quadriparetic. Although vasculitis serology findings were negative, intravenous methylprednisolone was initiated for presumed CNS vasculitis.
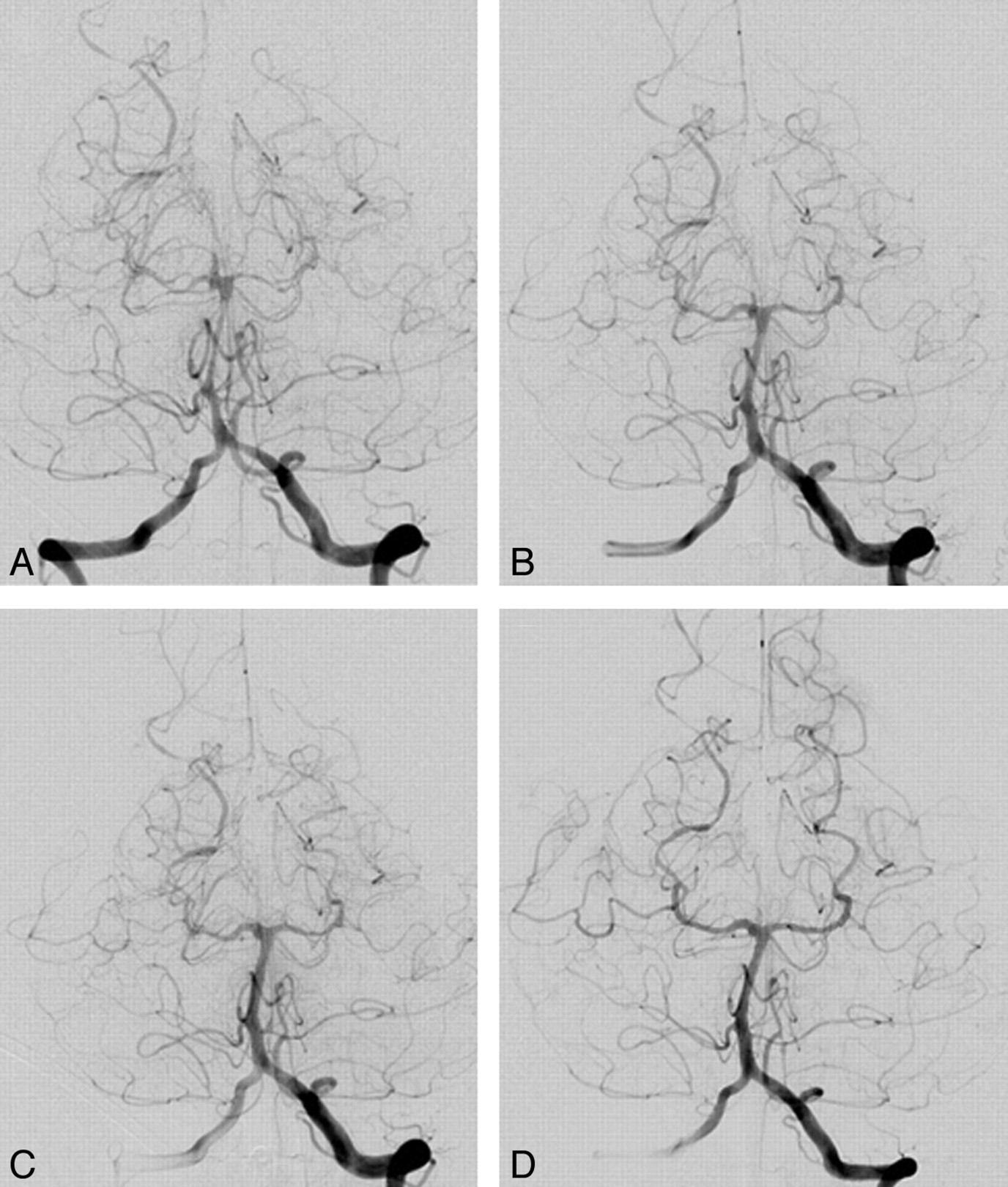
The patient was transferred to our hospital for further management. CSF was not inflammatory, hemorrhagic, or xanthochromic. Conventional angiography was performed (Fig 2 A). Verapamil was selectively infused into the left vertebral artery during angiography, yielding marked angiographic improvement in the degree of vasoconstriction within 20 minutes (Fig 2B). Given these findings, RCVS was also considered. PTA was performed in the supraclinoid ICAs, M1 MCAs, intracranial left vertebral artery, and basilar artery (Fig 2C), restoring nearly normal luminal caliber. Additional intra-arterial verapamil was infused in the ICAs, ACAs, and left vertebral artery to treat vasoconstriction beyond the reach of PTA. The patient's level of consciousness improved following endovascular therapy.

A, Before endovascular treatment, digital subtraction angiography on illness day 19 demonstrates marked narrowing of the basilar artery (measuring 1.1 mm in diameter) and proximal PCAs, with beaded irregular areas of narrowing and dilation in the distal PCAs. B, Following intra-arterial verapamil infusion, marked improvement is noted in the caliber of the basilar artery (2.2 mm) as well as the proximal PCAs. C, After PTA of the basilar artery, basilar artery caliber is further improved (3.1 mm). D, Repeat digital subtraction angiography on illness day 32 demonstrates stable basilar caliber (3.0 mm), though subsequent to further intra-arterial verapamil administration, further basilar artery dilation was observed (to 3.7 mm, not shown).
The patient was managed in the intensive care unit with oral verapamil and intravenous dantrolene. Vasopressor support with intravenous phenylephrine was titrated to systolic blood pressure >160 mm Hg to maintain cerebral perfusion in the setting of intracranial vasoconstriction. Serial transcranial Doppler imaging was performed to monitor proximal vasoconstriction.
On illness day 32, the patient became unresponsive during an episode of hypotension. Cerebral angiography was performed, revealing mild anterior and posterior (Fig 2D) circulation vasoconstriction. Again, intra-arterial verapamil was administered into the ICAs and left vertebral artery. Language function improved following this second endovascular intervention.
Phenylephrine was weaned, and the patient was transferred to a skilled nursing facility. She was blind but fluent and oriented to person, place, and time. She had spontaneous movement of bilateral fingers, left wrist, and left elbow; her legs remained plegic. The patient remained on oral verapamil therapy with 12-week follow-up MRA scheduled to confirm resolution of vasoconstriction.
Discussion
The pathophysiology of RCVS is not well-understood. Pregnancy, migraines, exposure to certain vasoactive drugs (pseudoephedrine, selective serotonin reuptake inhibitors, triptans, ergot derivatives, and cocaine), and trauma have been associated with this condition.1,8 The clinical course of RCVS is usually benign without treatment. However, severe neurologic dysfunction can occur due to ischemia in brain regions perfused by severely constricted arteries.1
Our patient developed RCVS after ingestion of pseudoephedrine, a known potential precipitator. Diagnosis of RCVS was delayed, with initial diagnoses of PRES and then cerebral vasculitis. Diagnosis of RCVS is challenging because angiographic findings are nonspecific. Multisegmental vasoconstriction has been reported in patients with a history of migraines, as well as in the postpartum period, following sexual intercourse, following aneurysmal SAH, and after administration of serotonergic or sympathomimetic drugs.9 Similar angiographic findings can also be associated with cerebral vasculitis or primary angiitis of the CNS, but these patients present with gradually progressive neurologic symptoms, encephalopathy, and CSF abnormalities in 80%–90% of cases.10 The clinical context of pseudoephedrine ingestion, acute thunderclap headache, the rapidly progressive clinical course, and the imaging findings combined led to a diagnosis of RCVS in our case.
The relationship between RCVS, hypertensive encephalopathy, and PRES is unclear. PRES is characterized by reversible gray matter and white matter lesions on MR imaging that often occur in the setting of hypertensive encephalopathy but also have been described in patients with presentations typical of RCVS.11 It is possible, therefore, that RCVS may occur as a cause of PRES, due to ischemia or cerebral edema, and as a consequence of hypertension in PRES when cerebral autoregulation is overwhelmed by massive increases in arterial and cerebral perfusion pressure. The coexistence of PRES and RCVS suggests that a disturbance in cerebral arterial tone is the pathophysiologic basis of both syndromes.1
Vasoconstriction of medium and large cerebral vessels can occur in PRES. Reduced perfusion at the resistance or microvascular level may also be related to endothelial activation and alterations in lymphocyte/T-cell trafficking.12 Given these features of PRES, overlap with RCVS is a complex issue. In many ways, they may be the same process. In the setting of immune suppression, a diagnosis of PRES would be clearer. In the case reported here, however, the trigger for vasculopathy or vasoconstriction could be either the patient's initial viral illness or her use of pseudoephedrine-containing cold medicine; the former would be more in keeping with PRES13 and the latter is more classically associated with RCVS.
RCVS has been demonstrated many times in PRES, and when the patient is evaluated, reduced perfusion has generally been observed, potentially leading to brain ischemia.14,15 While the older hypertension-hyperperfusion theory is popular, hyperperfusion has not been convincingly demonstrated in PRES. Angiography has often been performed in the setting of PRES during the onset of a sudden and severe (thunderclap-like) headache when the possibility of a ruptured aneurysm is suspected. The difference between PRES and RCVS might be the acuity of onset of the headache (resembling an aneurysm rupture) and the more common demonstration of vasoconstriction in the setting of vasoconstrictive drugs.
The optimal management of acute neurologic deficits caused by RCVS is uncertain.16 Alleviation of symptoms and reversal of vascular abnormalities have been reported with calcium channel blockers, glucocorticoids, magnesium sulfate, and observation.1,9 Unfortunately, the clinical course may be devastating; symptoms may clear initially only to return within days.17 Prolonged vasoconstriction leads to infarction of ≤54% of patients, most commonly in watershed areas and the posterior circulation.10,18
Given angiographic similarities and presumed vasospastic etiology, as well as the rapid clinical deterioration of our patient, we decided to treat our patient with RCVS in a manner similar to that of patients with SAH-induced vasospasm.19 It is not known, however, if the blood vessel narrowing observed in RCVS is actually due to vasospasm. This report demonstrates that RCVS-associated vascular narrowing responds to intra-arterial verapamil even more robustly than typical SAH-induced vasospasm. We used intra-arterial verapamil injection as a provocative test to demonstrate responsiveness of the basilar artery before treating the remainder of the cerebral vasculature with intra-arterial verapamil and PTA (Fig 2).
When vasospasm occurs following SAH, the most studied endovascular therapies are intra-arterial vasodilators and PTA.17,19,20 Cerebral blood flow improves after PTA for vasospasm with durable results. This is the first report of intra-arterial verapamil used in combination with PTA in a patient with RCVS. Reversal of vasoconstriction confirms the prompt effectiveness of this technique. Although intravenous or oral verapamil treatment alone might have been effective, that approach runs the risk of systemic hypotension resulting in decreased cerebral perfusion and watershed infarction in the setting of cerebral vasoconstriction. Direct intra-arterial application of calcium channel blockers may permit preferential intracranial arterial dilation while minimizing systemic hypotension.20
Intracranial PTA coupled with intra-arterial verapamil administration appears to be an effective treatment for RCVS. We propose that in cases of severe RCVS, PTA plus intra-arterial verapamil administration should be considered a therapeutic option to reverse neurologic deficits. Further clinical studies are warranted to determine optimal treatment.
References
- Received July 10, 2010.
- Accepted after revision August 23, 2010.
- © 2011 by American Journal of Neuroradiology
In this issue









{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Quantifying Intra-Arterial Verapamil Response as a Diagnostic Tool for Reversible Cerebral Vasoconstriction Syndrome
- Intra-Arterial Verapamil Treatment in Oral Therapy-Refractory Reversible Cerebral Vasoconstriction Syndrome
- Glucocorticoid-associated worsening in reversible cerebral vasoconstriction syndrome
- Reversible Cerebral Vasoconstriction Syndrome, Part 2: Diagnostic Work-Up, Imaging Evaluation, and Differential Diagnosis
- Multimodal Imaging of Reversible Cerebral Vasoconstriction Syndrome: A Series of 6 Cases