
Abstract
BACKGROUND AND PURPOSE: Collateral status at baseline is an independent determinant of clinical outcome among patients with acute ischemic stroke. We sought to identify whether the association between recanalization after intra-arterial acute stroke therapy and favorable clinical response is modified by the presence of good collateral flow assessed on baseline CTA.
MATERIALS AND METHODS: Data are from the Keimyung Stroke Registry, a prospective cohort study of patients with acute ischemic stroke from Daegu, South Korea. Patients with M1 segment MCA with or without intracranial ICA occlusions on baseline CTA from May 2004 to July 2009 who also had baseline MR imaging were included. Two readers blinded to all clinical information assessed baseline and follow-up imaging. Leptomeningeal collaterals on baseline CTA were assessed by consensus by use of the regional leptomeningeal score.
RESULTS: Among 84 patients (mean age, 65.2 ± 13.2 years; median NIHSS score, 14; interquartile range, 8.5), median time from stroke onset to initial MR imaging was 164 minutes. TICI 2b–3 recanalization was achieved in 38.1% of patients and mRS 0–2 at 90 days in 35.8% of patients. In a multivariable model, the interaction between collateral status and recanalization was significant. Only patients with intermediate or good collaterals who recanalized showed a statistically significant association with good clinical outcome (rate ratio = 3.8; 95% CI, 1.2–12.1). Patients with good and intermediate collaterals who did not achieve recanalization and patients with poor collaterals, even if they achieved recanalization, did not do well.
CONCLUSIONS: Patients with good or intermediate collaterals on CTA benefit from intra-arterial therapy, whereas patients with poor collaterals do not benefit from treatment.
ABBREVIATIONS:
- IAT
- intra-arterial therapy
- rLMC
- regional leptomeningeal collateral score
- SD
- standard deviation
Leptomeningeal collaterals are pre-existing anastomoses that connect a small number of distal-most arterioles within the crowns of the cerebral artery trees.1,2 During an acute stroke, ischemic brain depends on blood flow from these collaterals to survive until the occluded artery is opened.3⇓⇓⇓⇓–8 This collateral circulation is highly variable and potentially influences the rate at which an infarct grows.4,8⇓–10 Collateral status at baseline is an independent determinant of clinical outcome among patients with acute ischemic stroke.3,5,7,8,11 Nonetheless, “effect modification” by collateral status measured noninvasively by use of CTA of the relationship between recanalization and clinical outcome has not been demonstrated before. This tool can be used to select patients for intra-arterial therapy (IAT) through demonstration of a differential clinical response to recanalization by collateral status.
In this study, we first demonstrate the concept of validity of collateral status measured by use of CTA among patients presenting with acute ischemic stroke by correlating it with infarct volume on baseline MR DWI and infarct growth over 24 hours. We then demonstrate “effect modification” by collateral status of the relationship between recanalization and clinical outcome in patients with acute ischemic stroke undergoing IAT, thus justifying the use of baseline collateral status on CTA as a patient selection tool for IAT.
MATERIALS AND METHODS
The Keimyung Stroke Registry is an ongoing, single-center, prospective cohort study of patients with acute ischemic stroke presenting to the Keimyung University, Dongsan Hospital in Daegu, South Korea. All patients undergo an NCCT of the head at admission followed by CTA of the head and neck. For the study (time period, May 2004 to July 2009), we included only patients presenting with acute ischemic stroke with M1 segment MCA with or without ICA occlusion on baseline CTA with witnessed stroke symptom onset who were treated with IAT and had a pretreatment brain MR imaging and 24-hour posttreatment MR imaging. During this time period, there were 286 patients with documented anterior circulation occlusions on baseline CTA. We excluded 202 patients (43 patients with a documented MCA occlusion beyond the M1 MCA segment, 28 patients with isolated ICA without M1 MCA occlusion, 7 patients with simultaneously detected occlusions in the posterior circulation or contralateral ICA territory, 71 patients with unknown stroke onset time, 16 patients with baseline MR imaging obtained after treatment, 29 patients with poor-quality MR imaging at baseline, and 8 patients without 24-hour MR imaging). Finally, 84 patients were included in these analyses. Stroke severity was assessed by use of the NIHSS at baseline, immediately after treatment, at discharge, and at 90 days. Interval times from stroke symptom onset to presentation in the emergency department, imaging, and endovascular procedures were collected. Functional status was assessed at baseline and 90 days by use of the mRS. We collected data on mRS by clinical review in a face-to-face interview at 3 months (in approximately 70% of patients) and by telephone interview at 3 months (in approximately 25% of patients). For 5% of patients, we obtained the 3-month mRS information at 5–9 months. The study was approved by the local institutional review board.
Imaging Protocol
Standard nonhelical NCCT was performed on a multisection scanner (Sensation 16; Siemens, Erlangen, Germany) by use of 120 kV, 170 mAs, with 5-mm section thickness. NCCT was followed by CTA with the use of a helical scan technique. Coverage was from arch to vertex, with continuous axial sections parallel to the orbitomeatal line with 0.6–1.25-mm section thickness. Acquisitions were obtained after a single bolus intravenous contrast injection of 90–120 mL nonionic contrast media into an antecubital vein at 3–5 mL/s, auto-triggered by appearance of contrast in a region of interest manually placed in the ascending aorta. This was followed by a baseline MR imaging (3T Signa Excite; GE Healthcare, Milwaukee, Wisconsin) consisting of DWI, time-of-flight MRA, and gradient recalled-echo as a part of a stroke protocol. Follow-up MR imaging was performed within 24 hours by use of the same protocol.
Intra-Arterial Therapy
Intravenous tPA was given to all eligible patients within 3 hours of stroke onset as per accepted guidelines. MR imaging was primarily used to assess intracerebral hemorrhage on gradient recalled-echo and recanalization status on MR TOF. Patients were taken to the angiography suite from the MR imaging suite for IAT. Patients with MCA occlusions with or without ICA occlusions who did not show recanalization on MRA or rapid clinical improvement after IV tPA were considered for IAT. IAT included local urokinase (10,000–20,000 IU/min; maximum permissible dose, 300,000 IU; Green Cross Pharm, Seoul, Republic of Korea), balloon angioplasty, or wire manipulation. Glycoprotein IIb/IIIa receptor antagonists were given in a small number of patients. For clots not manageable by the above methods, we used off-label stent placement (with the use of coronary stents). Recanalization was assessed by means of angiography in all cases. Successful recanalization was defined as TICI 2b/3 flow on final angiogram. Penumbra Stroke System aspiration catheters (Penumbra, Alameda, California) and stent retriever devices (eg, Solitaire FR [Covidien, Irvine, California], Trevo [Stryker, Kalamazoo, Michigan]) were not available during this period.
Imaging Analyses
Baseline and follow-up images were analyzed at the imaging core lab of the Calgary Stroke Program. OsiriX version 3.5 (http://www.osirix-viewer.com), an image-processing software designed for multiplanar reconstruction, was used to reconstruct 2D multiplanar reconstruction images of CTA in axial, coronal, and sagittal planes by use of 24-mm-thick slabs. Leptomeningeal collaterals were assessed on baseline CTA by consensus (B.K.M., S.I.S.) by use of the regional leptomeningeal score (rLMC), a previously published ordinal scoring system that is based on the Alberta Stroke Program Early CT Score template that has excellent interrater reliability3 (Fig 1). Infarct volumes were measured on baseline and 24-hour MR DWI by use of an in-house–validated software, Quantomo (Cybertrial, Calgary, Canada). Infarct growth over 24 hours was calculated by subtracting initial infarct volume from the 24-hour volume measurement. Quantomo has been previously validated and has good interrater and intrarater agreement.12 Readers were blinded to all clinical information and follow-up data at the time of scan reading.

Collateral status on CTA as measured by the rLMC score with baseline and 24-hour infarct volume on MR DWI.
Statistical Analyses
Continuous variables are summarized as means (±1 SD) or medians (interquartile range or range) as appropriate. Collateral status by use of the rLMC score (0–20) was trichotomized into 3 groups: good (17–20), intermediate (11–16), and poor (0–10), according to previously published literature.3 Differences between these 3 groups were assessed by means of the Fisher exact test for proportions, 1-way ANOVA for parametric data, and a rank sum test for nonparametric data. We adjusted for multiple comparisons by use of the Bonferroni method. We tested for trend in outcome measure (infarct growth and mRS 0–2 at 90 days) by collateral status in the recanalizers (TICI 2b–3) and in the non-recanalizers (TICI 0–1) by use of the Cuzick test of trends. We then built a multivariable model by use of generalized linear modeling with a log link, with mRS 0–2 versus 3–6 at 90 days as the outcome and collateral status (good, intermediate, and poor), recanalization status (TICI 2b–3 versus 0–2a), and age (by decile) as independent variables. Because there was no significant association of sex, baseline NIHSS, or onset to imaging time with mRS at 90 days, these variables were not included in the model. We specifically included a multiplicative interaction term between collateral status and recanalization status. All hypothesis tests were 2-sided, with a value of P < .05 considered statistically significant. In multivariable analysis, interaction effects were considered significant at a value of P < .10.13 Analyses were performed with the use of STATA/SE 12.1 software (StataCorp, College Station, Texas).
RESULTS
Among 84 patients, the mean age was 65.2 ± 13.2 years, median NIHSS score was 14 (interquartile range, 8.5), and median time from stroke onset to initial MR imaging was 164 minutes. Successful recanalization (TICI 2b–3) was achieved in 38.1% of patients and good clinical outcome (mRS 0–2 at 90 days) in 35.8% of patients. Mean baseline infarct volume was 58.5 mL (±1 SD, 64.4 mL) and mean infarct growth over 24 hours was 58.3 mL (±1 SD, 72 mL). There were 19 patients with good, 34 with intermediate, and 31 with poor collateral scores at baseline. Baseline characteristics stratified by good, intermediate, and poor collateral status are described in Table 1. Patients with good collateral status had lower baseline NIHSS score, higher baseline ASPECTS on NCCT, smaller baseline infarct volume on MR imaging, and lesser infarct growth over 24 hours (Table 1).
Baseline characteristics of patients in study stratified by collateral status (n = 84)
Infarct growth over 24 hours was significantly lower in patients with good collateral status at baseline who achieved recanalization (7.0 mL; ±1 SD = 11.7 mL) when compared with those with intermediate collateral status who achieved recanalization (26.6 mL; ±1 SD = 43.4 mL) and those with poor collaterals who recanalized (67.7 mL; ±1 SD = 75.1 mL) (P = .05; between group difference). There was no difference in infarct growth in the non-recanalizers stratified by collateral status (good collaterals: 58.4 mL, ±1 SD = 58.6 mL; intermediate collaterals: 48.6 mL, ±1 SD = 63.7 mL; poor collaterals: 100.4 mL, ±1 SD = 91 mL; P = .09, between-group difference) (Fig 2). Similarly, good clinical outcome (mRS 0–2 at 90 days) was higher among patients with good collateral status who achieved recanalization (100%) when compared with those with intermediate collateral status who recanalized (58.8%) and those with poor collaterals who recanalized (33.3%) (P = .04). There was no statistically significant difference in good clinical outcome in the non-recanalizers stratified by collateral status (30.8% in those with good collaterals, 17.6% in those with intermediate collaterals, and 18.2% in those with poor collaterals; P = .67). The Cuzick test of trend by collateral status was statistically significant for good clinical outcome (mRS 0–2 at 90 days, P = .01) in the recanalizers. There was no statistically significant trend by collateral status for good clinical outcome (P = .08) in the non-recanalizers (Fig 3).
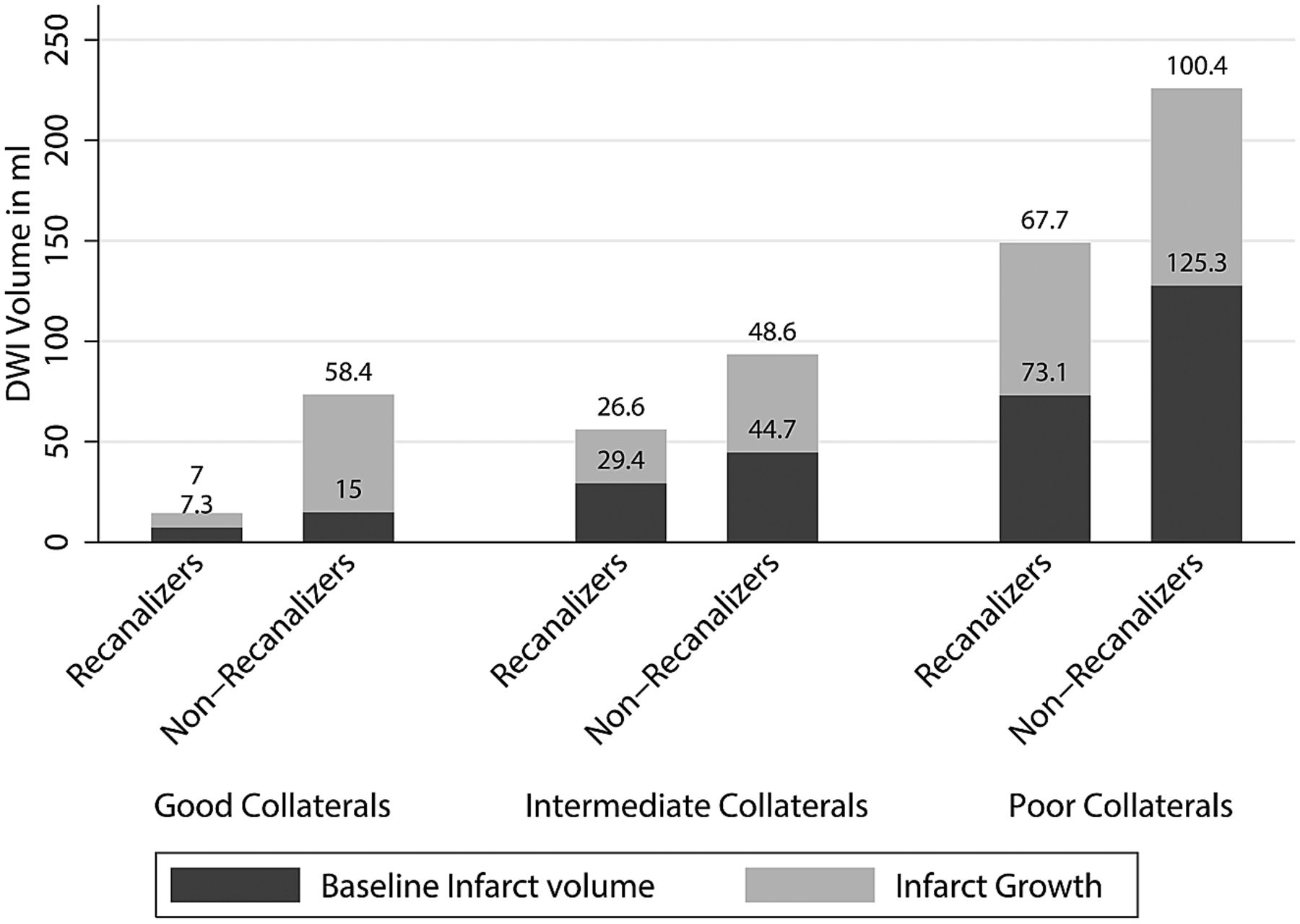
Mean baseline infarct volume and infarct growth over 24 hours stratified by baseline collateral status on CTA and final recanalization (TICI score 2b–3 versus 0–2a).

Ninety-day clinical outcome according to the mRS stratified by baseline collateral status on CTA and final recanalization (TICI score, 2b–3).
In the multivariable model, the interaction between collateral status and recanalization was relevant (P = .08). This final model also included age as a significant independent predictor of good clinical outcome. Given the presence of a statistically significant interaction in the model, we report age- and sex-adjusted rate ratios for patients in 4 groups, namely, group 1 (poor collaterals who do not recanalize, n = 22), group 2 (poor collaterals who recanalize, n = 9), group 3 (intermediate or good collaterals who do not recanalize, n = 30), and group 4 (intermediate or good collaterals who recanalize, n = 23). Patients with intermediate and good collaterals were collapsed into 1 group for ease of reporting interaction effects. Only patients with intermediate or good collaterals who recanalize showed a statistically significant association with good clinical outcome (rate ratio = 3.8; 95% CI, 1.2–12.1). None of the other groups did as well clinically (Table 2). Fig 3 shows the unadjusted mRS scores at 90 days in these 4 groups stratified by recanalization status.
Generalized linear model with the use of log link showing rate ratios for good clinical outcome (mRS 0–2 at 90 days) by collateral status and recanalization status adjusted for age and sex
DISCUSSION
Our results show that collateral status measured at baseline by use of CTA among patients with acute ischemic stroke correlates with baseline infarct volume and with infarct growth over 24 hours. Furthermore, we demonstrated effect modification by collateral status of the relationship between recanalization and good clinical outcome. Patients with good and intermediate collaterals who achieve recanalization with IAT do well when compared with those who do not achieve recanalization. Patients with poor collaterals do not do well even if recanalization is achieved with IAT (Table 2).
Several imaging paradigms propose to “select” patients most suitable for IAT.14⇓⇓⇓–18 MR imaging–based diffusion/perfusion mismatch is one such paradigm. MR imaging, however, takes time to screen, perform, and interpret.19 Many patients do not tolerate it as well as CT; image quality is affected by patient motion. MR imaging also has limited availability “after hours.”20 Moreover, the recent MR Rescue Trial showed that the tool may not help in selecting patients for IAT.21 NCCT ASPECTS has moderate interrater reliability, even among experts.22⇓⇓–25 Reliability is less in the early presenters (within 90 minutes from stroke symptom onset).26 In addition, ASPECTS interpretation is affected by patient motion and in the aged.27 CT perfusion needs algorithms for postprocessing images that are vendor-specific, not standardized, and therefore variable across centers.28⇓⇓–31 Trained personnel are sometimes needed to process these images. In addition, image quality is affected to some extent by patient motion.29 Additional radiation dose is also a concern.32 Collateral assessment on CTA has good interrater reliability.3,4,33 Good correlation with baseline infarct volume and infarct growth on MR DWI in our study demonstrates the tool's content validity. Furthermore, by demonstrating “effect modification” by collateral status among patients undergoing IAT, we demonstrate for the first time that this tool can be used to select patients for this therapy. Collateral assessment on CTA does not need any sophisticated algorithm or trained personnel for postprocessing images and is relatively resistant to patient motion–induced artifacts. It is available 24 hours a day in most centers. We therefore propose the use of this tool for patient selection within future endovascular trials.
Despite the variability in measuring collaterals at baseline in patients with acute ischemic stroke, our study further reinforces evidence from previous literature that patients with good collaterals at baseline have small baseline infarcts when compared with patients with intermediate and poor baseline collaterals.34,35 Recanalization helps reduce further infarct growth, thus limiting size of final infarct.8 Our study also shows that the rate of infarct growth is quicker in patients with intermediate collaterals; these patients may only benefit if recanalization is achieved quickly. Patients with poor collaterals at baseline grow their infarcts the quickest; the likelihood that they will benefit from recanalization is the least. Nonetheless, the fact that some patients with poor collaterals in our study achieved good clinical outcome raises the possibility that routine CTA may have underestimated good and intermediate collaterals in some patients, misclassifying these collaterals as poor. Routine CTA is a single snapshot of contrast-filled blood vessels. Early timing of image acquisition with respect to that of bolus injection could potentially result in underestimation of true collateral status by use of this technique.3 The 4 patients who achieved good clinical outcome despite having poor collaterals at baseline and not achieving recanalization had a mean baseline infarct volume of 63.1 mL (range, 13.3–133.5 mL) compared with a mean baseline infarct volume of 110 mL for all patients with poor collaterals in the study, thus suggesting possible misclassification of good and intermediate collateral status as poor by use of routine CTA in at least those patients with small or intermediate baseline infarct volume.36 The rLMC score used in our study, being more liberal when defining poor collaterals in comparison with stricter definitions used in other studies, could also explain why some patients with poor collaterals did well in our study.34 Finally, variability in brain eloquence or possible misclassification of 90-day clinical outcome as the result of telephone follow-up in approximately 25% of patients could potentially explain why 2 patients with poor baseline collaterals and baseline infarct volumes >80 mL in our study did well clinically.36 Both these patients had right hemisphere infarcts. Our study, however, is able to show with a degree of statistical certainty that the patients most likely to benefit from recanalization are those with good and intermediate baseline collaterals; patients with poor collaterals do not show a differential response to recanalization.
Reperfusion-related edema and injury has been postulated to be a cause for increased infarct growth among patients without mismatch who achieve reperfusion.18 In our study, patients with poor collateral status who did not recanalize had more infarct growth than did patients with poor collateral status who recanalized. Our results do not support the reperfusion injury hypothesis. On the contrary, we speculate that early recanalization, even among patients with poor collaterals, may reduce the risk of death.37
Our study is not a randomized, controlled trial. Similar to previous studies supporting the use of a “mismatch”-based paradigm on perfusion imaging, our study provides evidence for the use of a “CTA collateral assessment–based paradigm” in selecting patients for IAT.18 We did not have data on every procedural time metric; approximately 30% of follow-up clinical data (mRS at 90 days) was ascertained by telephone. We were also underpowered to do a secondary analysis on the effect of time to recanalization on clinical outcomes stratified by collateral status. Our recanalization rates are modest and reflective of the time period when patients were recruited; nonetheless, our study is unique in that we were able to show a statistically significant interaction between collateral status and recanalization. With the advent of stent retrievers that achieve recanalization rates in excess of 80%, future demonstration of such statistically significant “effect modification” may need very large cohorts.37 Our study is thus timely in being able to demonstrate the utility of this tool in patient selection for IAT.
Conclusions
The results from our study suggest a differential clinical and imaging response to recanalization by IAT in patients with good and intermediate collaterals. Patients with poor collaterals show no such differential response. Collateral assessment on CTA can potentially help aid patient selection for acute intra-arterial stroke treatment and for potential inclusion in endovascular stroke trials.
Footnotes
Disclosures: Emmad Qazi—UNRELATED: Employment: The Calgary Stroke Program, Comments: I work at the Calgary Stroke Program as a part-time employee. Mayank Goyal—UNRELATED: Consultancy: Covidien/ev3, Comments: For designing and conducting trial; Grants/Grants Pending: Covidien/ev3,* Comments: Funding for ESCAPE trial; Payment for Lectures (including service on speakers bureaus): Covidien/ev3, Comments: For speaking engagements related to acute stroke treatment. Michael Hill—UNRELATED: Board Membership: DSMB Aldagen trial; Grants/Grants Pending: Covidien,* Comments: Grant for a clinical trial; Stock/Stock Options: Calgary Scientific Inc. (stock). Bijoy Menon—UNRELATED: Grants/Grants Pending: Heart and Stroke Foundation of Canada,* CIHR*. Andrew Demchuk (UNRELATED): Grant support and lecture fees: Covidien,* Heart and Stroke Foundation of Canada,* CIHR*. (*money paid to institution).
REFERENCES
- Received July 19, 2013.
- Accepted after revision September 29, 2013.
- © 2014 by American Journal of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Collateral status and recanalization after endovascular treatment for acute ischemic stroke
- Factors associated with unfavorable outcome after anterior circulation stroke despite successful reperfusion and early neurological improvement
- Comparison between collateral status and DEFUSE 3 or DAWN criteria in patient selection for endovascular thrombectomy within 6-24 hours after stroke: a protocol for meta-analysis
- Circle of Willis variation and outcome after intra-arterial treatment
- Collateral status reperfusion and outcomes after endovascular therapy: insight from the Endovascular Treatment in Ischemic Stroke (ETIS) Registry
- Collateral status and recanalization after endovascular treatment for acute ischemic stroke
- Recent Administration of Iodinated Contrast Renders Core Infarct Estimation Inaccurate Using RAPID Software
- Dynamic CTA-Derived Perfusion Maps Predict Final Infarct Volume: The Simple Perfusion Reconstruction Algorithm
- Clinical prognosis of FLAIR hyperintense arteries in ischaemic stroke patients: a systematic review and meta-analysis
- Impact of single phase CT angiography collateral status on functional outcome over time: results from the MR CLEAN Registry
- Inter- and intraobserver reliability for angiographic leptomeningeal collateral flow assessment by the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) scale
- Collateral status affects the onset-to-reperfusion time window for good outcome
- Value of Quantitative Collateral Scoring on CT Angiography in Patients with Acute Ischemic Stroke
- CT angiography-based collateral flow and time to reperfusion are strong predictors of outcome in endovascular treatment of patients with stroke
- Initial hospital management of patients with emergent large vessel occlusion (ELVO): report of the standards and guidelines committee of the Society of NeuroInterventional Surgery
- Comparison of CTA- and DSA-Based Collateral Flow Assessment in Patients with Anterior Circulation Stroke
- Posterior circulation CT angiography collaterals predict outcome of endovascular acute ischemic stroke therapy for basilar artery occlusion
- CTA collateral score predicts infarct volume and clinical outcome after endovascular therapy for acute ischemic stroke: a retrospective chart review
- Leptomeningeal collateral vessels are a major risk factor for intracranial hemorrhage after carotid stenting in patients with carotid atherosclerotic plaque
- Impact of collaterals on the efficacy and safety of endovascular treatment in acute ischaemic stroke: a systematic review and meta-analysis
- Collateral Status on Baseline Computed Tomographic Angiography and Intra-Arterial Treatment Effect in Patients With Proximal Anterior Circulation Stroke
- Relative CBV ratio on perfusion-weighted MRI indicates the probability of early recanalization after IV t-PA administration for acute ischemic stroke
- Comparing Vessel Imaging: Noncontrast Computed Tomography/Computed Tomographic Angiography Should Be the New Minimum Standard in Acute Disabling Stroke
- Effect of Collaterals on Clinical Presentation, Baseline Imaging, Complications, and Outcome in Acute Stroke
- Poor Collateral Circulation Assessed by Multiphase Computed Tomographic Angiography Predicts Malignant Middle Cerebral Artery Evolution After Reperfusion Therapies
- Role of Imaging in Current Acute Ischemic Stroke Workflow for Endovascular Therapy
- Predictors of Reperfusion in Patients with Acute Ischemic Stroke
- Differential Effect of Baseline Computed Tomographic Angiography Collaterals on Clinical Outcome in Patients Enrolled in the Interventional Management of Stroke III Trial
- Consistently Achieving Computed Tomography to Endovascular Recanalization <90 Minutes: Solutions and Innovations
- Influence of Age on Clinical and Revascularization Outcomes in the North American Solitaire Stent-Retriever Acute Stroke Registry
- On the Search for the Perfect Mismatch!
- Challenges of Acute Endovascular Stroke Trials
- Computed Tomographic Angiography and Cerebral Blood Volume Can Predict Final Infarct Volume and Outcome After Recanalization