
Abstract
BACKGROUND AND PURPOSE: Impairment of macrophage polarization from a proinflammatory macrophage type 1 (M1) population to an anti-inflammatory macrophage type 2 (M2) population is a hallmark of poor wound healing. In this study, we aimed to evaluate the distribution of M1 and M2 macrophages and to analyze their association with healing in aneurysms embolized by endovascular coiling.
MATERIALS AND METHODS: Elastase-induced aneurysms were created in female rabbits and subsequently embolized with platinum coils. Aneurysm occlusions were evaluated with angiographic imaging at 1 (n = 6), 3 (n = 5), or 6 (n = 6) months. Aneurysm tissues were harvested for histologic analysis, quantification of M1 and M2 macrophages by immunofluorescence, and collagen deposition determined by Masson trichrome staining. Histologic grading of aneurysm healing was also performed. Untreated aneurysms were used as controls (n = 6).
RESULTS: The M1 macrophage population was highest at 1 month posttreatment, progressively decreasing at 3 and 6 months. The M2 macrophage population progressively increased at 3 and 6 months posttreatment. The highest collagen deposition was at 6 months posttreatment. We found a moderate-to-weak direct correlation between the percentage of M2 macrophages and collagen deposition, as well as total histologic scores overall, and a strongly positive direct correlation between the percentage of M2 macrophages and total histologic scores at 6 months posttreatment.
CONCLUSIONS: Our data support the direct correlation between M2 macrophage polarization and healing in aneurysm tissues. Our results show a positive relationship between M2 macrophage populations and total histologic scores at later stages of healing after endovascular coiling. We conclude that interventions aimed at stimulating M2 macrophage expression locally may improve aneurysm healing after coil embolization.
ABBREVIATIONS:
- CD80
- cluster of differentiation 80
- CD206
- cluster of differentiation 206
- M1
- macrophage type 1
- M2
- macrophage type 2
Endovascular coiling is a safe and effective treatment to achieve occlusion of saccular intracranial aneurysms. With time, however, incomplete occlusion and recurrence remain challenging obstacles to successful endovascular treatment.1,2 Several previous studies have demonstrated associations between poor occlusion or recurrence of aneurysms and factors such as aneurysm size and volume, coil packing density, coil compaction,3,4 unorganized thrombus, blood pressure, lack of neointima formation, and regulation of cells.5,6 Few studies have evaluated the infiltration of inflammatory cells into the aneurysm dome during the healing process after endovascular coiling.7,8
Inflammatory cells are emerging as a topic of clinical interest in this area. Macrophages may be particularly valuable, due to the unique process of macrophage polarization and its potential impact on wound healing and tissue remodeling. The remarkable plasticity of macrophages enables these cells to change their form and functional phenotype from classically activated macrophage type 1 (M1) to alternatively activated macrophage type 2 (M2) in response to signals in their local environment.9,10
The regulation of macrophage subtype M1 (cluster of differentiation 80 [CD80]) and M2 (cluster of differentiation 206 [CD206]) markers has been studied in several disease models.11-14 Previous studies have demonstrated the persistence of a proinflammatory M1 macrophage population without a subsequent transition to an anti-inflammatory M2 phenotype in poorly healing wounds. Enhancement of T1 M2 macrophage polarization could be a potential therapeutic option in wound healing.15,16
In this study, we aimed to evaluate the distribution of M1 and M2 macrophages and to analyze their association with healing in aneurysms embolized by endovascular coiling.
MATERIALS AND METHODS
Aneurysm Creation and Tissue Harvest
Elastase-induced saccular aneurysms were created in 23 New Zealand white female rabbits, weighing between 2.5 and 4 kg. The procedures for aneurysm creation were performed as described previously.17 Aneurysms were permitted to mature for at least 3 weeks after creation. All treated aneurysms were embolized with the standard bare platinum coils as previously described.18 The animals were euthanized by lethal injection of pentobarbital at 1 month (n = 6), 3 months (n = 5), or 6 months (n = 6) after endovascular treatment. Untreated control animals were sacrificed at 1 month (n = 3) and 3 months (n = 3). The harvested aneurysm tissue samples were fixed in 10% neutral buffered formalin, embedded in paraffin, and sectioned as previously described.19 Some of the rabbits used in this study were originally part of another investigation, in which bare platinum coils were used to treat the aneurysms. The original investigation was entirely unrelated to this project,20 and did not interfere with the goals of this study.
Angiography
DSA images were obtained immediately after coil implantation and just before sacrifice. The follow-up, presacrifice images were assessed by comparing them with the images after coil implantation using a 3-category grading system (stable occlusion, progressive occlusion, recanalization [coil compaction]).
Immunofluorescence
The paraffin-embedded tissue sections were mounted on microscope slides (Superfrost; Cardinal Health) and incubated for 2 hours at 56°C. The slides were de-paraffinized with xylene and alcohol and washed with water. Antigen retrieval was performed by boiling at 95°C for 15 minutes in a 0.1- mol/L citric acid buffer. The slides were then blocked with appropriate blocking buffer for 30 minutes at room temperature. Slide sections were incubated overnight at 4°C in primary antibodies for M1 (CD80, 1:100 dilution, catalog number 8679; ProSci) or M2 (CD206, 1:50 dilution, catalog number AF2535; R&D Systems). The slides were washed and incubated in secondary antibodies (Cy3; Jackson Immuno-Research Laboratories) for 2 hours. The slides then were counterstained with nucleic acid stain (Hoechst 33258; Thermo Fisher Scientific) for 5 minutes, then washed, dehydrated, and mounted with mounting medium (Shandon Consul-Mount; Thermo Fisher Scientific). Five randomly assigned fields were chosen and captured on a FluoView FV1200 confocal microscope (Olympus Life Science). Human tonsil was used as a positive control and for a negative control when the primary antibody was omitted. The number of positively staining cells in each image was counted manually by 3 separate individuals.
Collagen Deposition
Collagen deposition was analyzed quantitatively through Masson trichrome staining as previously described.21 The images were captured using microscopy imaging (RTV 5.0; Qimaging MicroPublisher). The images were analyzed using a recently described and experimentally verified image analysis technique,22 using Photoshop software (Adobe).
Histologic Grading
Histologic grading of aneurysm tissues was performed by an experienced reviewer (>15 years of experience in aneurysm-specific pathology), and grading was followed according to the previously described protocol.21,23 Neck healing was based on both gross and microscopic inspection. The scores of the gross (0–3) and microscopic inspection (0–4) were averaged to yield a single neck score. If different areas of the aneurysm neck showed different levels of healing, intermediate scores (0.5) were used. Microcompaction assessment (0–3) was based on the shape of the coil mass across the neck, from concave to convex. Healing characteristics in the dome (0–5) were categorized on the basis of the density of cellular infiltration and the area of organized tissue. Accordingly, each score was added together to obtain a total histologic score, as described in Equation 1.
Equation 1: Calculation of total histologic score

Statistical Analysis
All statistical analyses were performed using GraphPad Prism software (GraphPad Software). The differences between the treatment-to-sacrifice time groups were evaluated using the Student t test. The strength of the linear relationships between M2 macrophages and both collagen deposition and histologic grading was evaluated using the Pearson correlation coefficient. Descriptive data were presented as means ± standard error of mean. A P value of < .05 was considered statistically significant.
RESULTS
Angiography
Angiographic imaging of aneurysms before coiling indicated that the mean measurements did not differ significantly among the 3 treatment-to-sacrifice time groups (Table). Follow-up images obtained 1 month posttreatment demonstrated stable occlusion in 4/6 (66.7%) aneurysms, progressive occlusion in 1/6 (16.7%) aneurysms, and coil compaction in 1/6 (16.7%) aneurysms. In the group sacrificed 3 months posttreatment, 5/5 (100%) aneurysms showed stable occlusion. In the group sacrificed 6 months posttreatment, 5/6 (83.3%) aneurysms showed stable occlusion and 1/6 aneurysms (16.7%) showed progressive occlusion. All control, untreated aneurysms remained patent before sacrifice.
Aneurysm geometry results of all the study groupsa
M1 and M2 Macrophage Populations
The mean number of proinflammatory M1 macrophages (CD80) found in the 1-month posttreatment group (58.86 ± 29.52) was significantly higher compared with both the 3-month posttreatment group (4.96 ± 3.79, P = .003) and the 6-month posttreatment group (6.2 ± 3.67, P < .01) (Fig 1). The number of M1 macrophages did not differ significantly between the 3- and 6-month groups (P = .587). In contrast, the mean number of anti-inflammatory M2 macrophages (CD206) was significantly higher in the 6-month posttreatment group (15.8 ± 4.50) compared with both the 1-month group (6 ± 5.23, P < .01) and the 3-month group (7.8 ± 4.32, P = .015). No significant differences were observed between 1 and 3 months (P = .555). There were no positively staining cells observed in the untreated aneurysm control group for either M1 or M2 markers (Fig 1B).
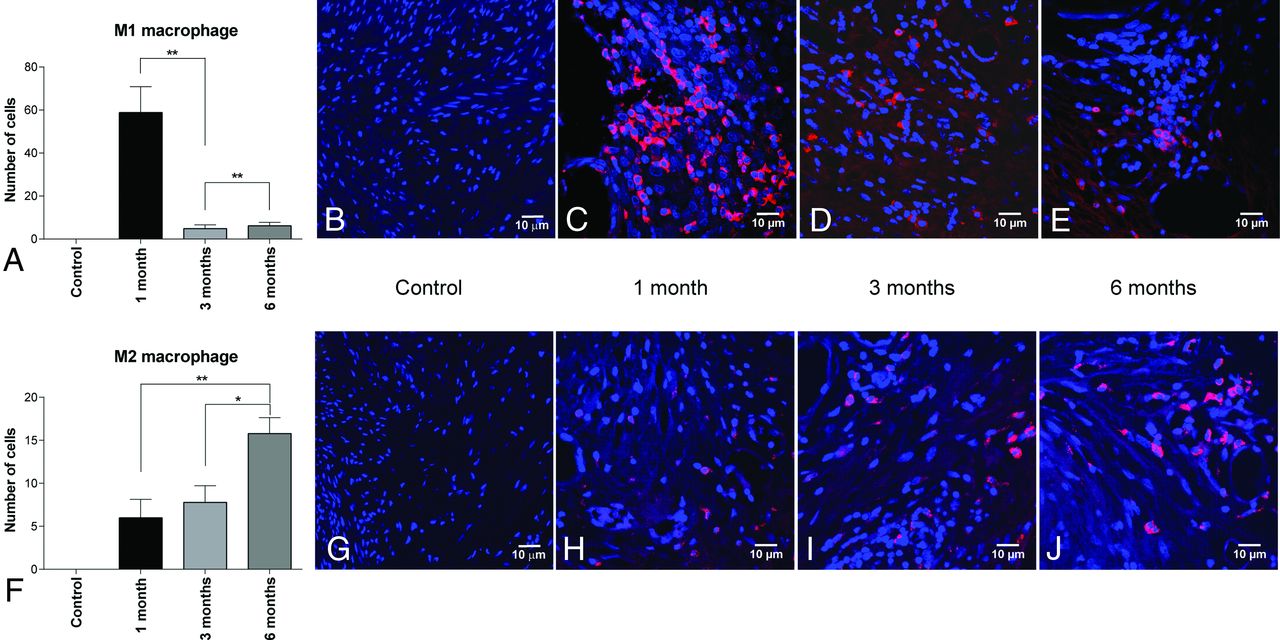
M1 and M2 macrophage populations in aneurysm tissues after endovascular coiling for control and treatment groups. A, Mean number of M1 macrophages ± standard error of the mean. Representative confocal microscopy images of cells staining positive for CD80 (60× oil magnification) at 1 month (C), 3 months (D), and 6 months (E). F, Mean number of M2 macrophages ± standard error of the mean. Representative confocal microscopy images of cells staining positive for CD206 (60× oil magnification) at 1 month (H), 3 months (I), and 6 months (J). B and G, Representative confocal images of control aneurysm tissues stained for CD80 and CD206, respectively, at 1 month (20× oil magnification). Asterisk indicates P < .05; double asterisks, P < .01.
Collagen Deposition
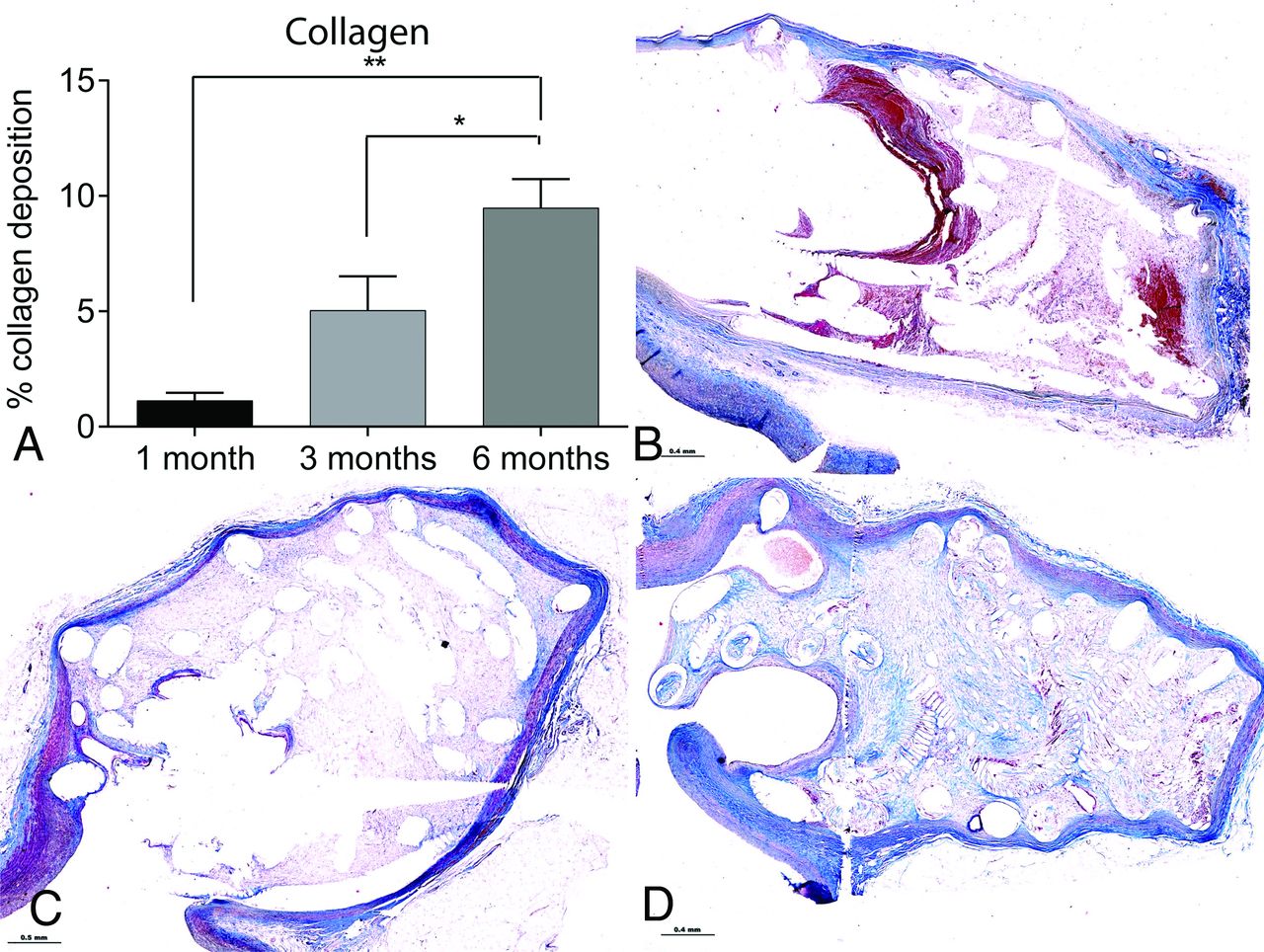
The mean percentage of collagen deposition was significantly higher in the 6-month posttreatment group (9.48 ± 3.07%) compared with both the 1-month (1.14 ± 0.81%, P < .001) and 3-month (7.43 ± 3.29%, P < .05) posttreatment groups (Fig 2). No significant difference was observed between 1 and 3 months posttreatment (P > .05).
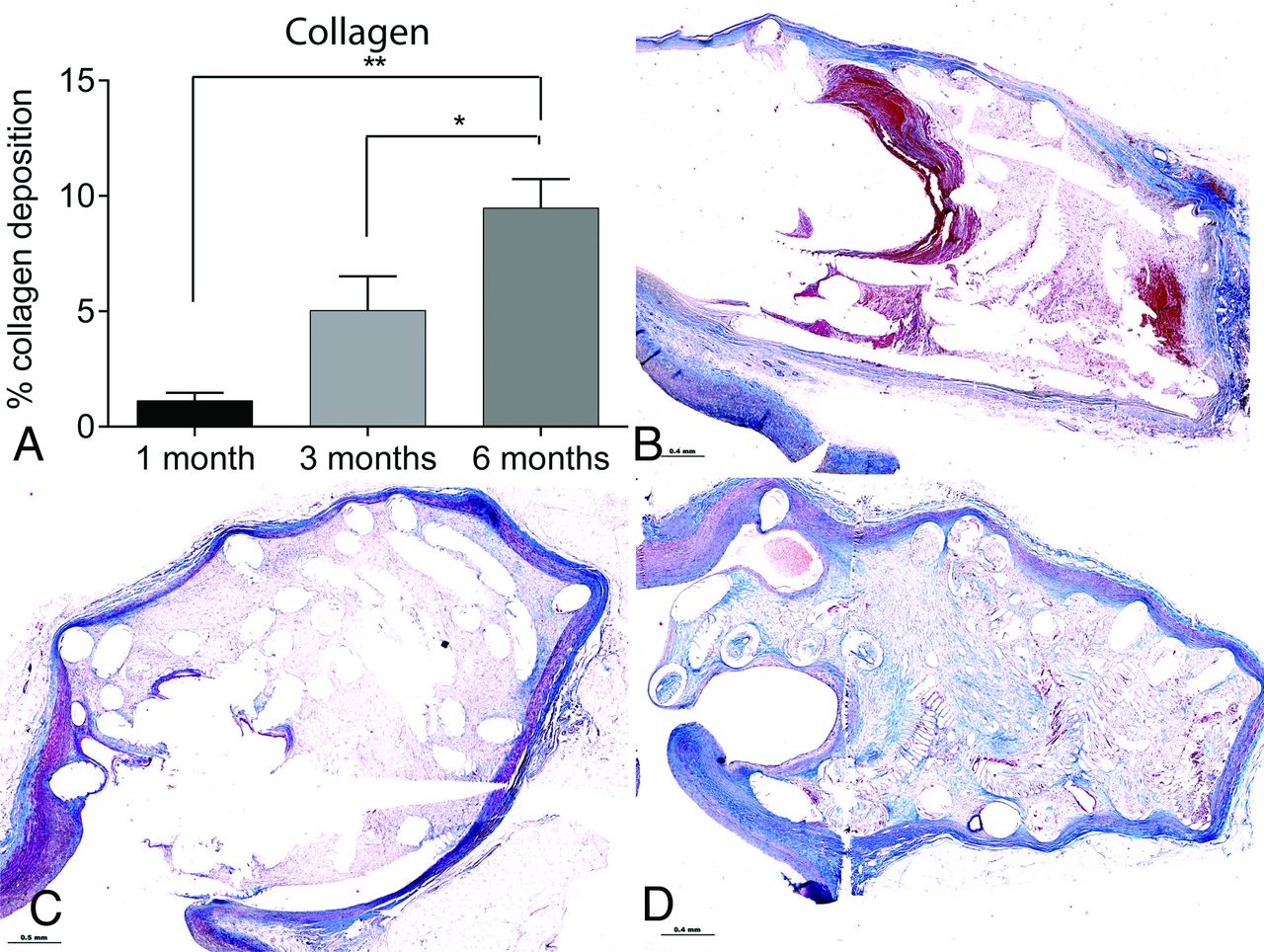
Collagen deposition in aneurysm tissues after endovascular coiling for 3 treatment-to-sacrifice time groups. A, Mean percentage of collagen deposition ± standard error of the mean. Photomicrographs of collagen deposition using Masson trichrome stain are shown for 1 month (B), 3 months (C), and 6 months (D) (2.5× magnification; scale bar =0.4 mm). Asterisk indicates P < .05; double asterisks, P < .01.
Histologic Grading
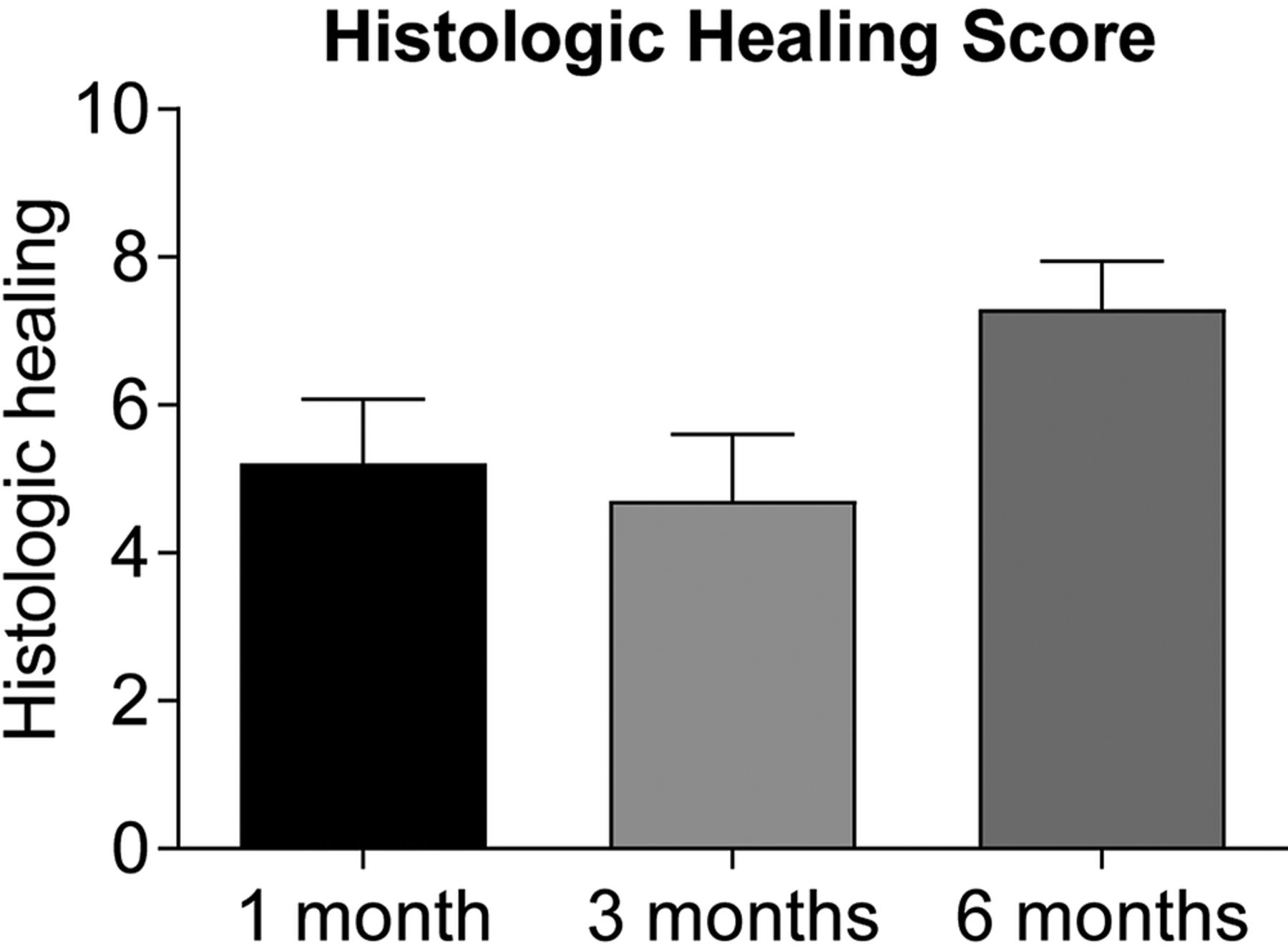
The mean total histologic scores at 1 month posttreatment (5.21 ± 2.12) did not differ significantly compared with the 3-month (4.7 ± 2.03, P > .05) or 6-month (7.3 ± 1.59, P > .05) posttreatment groups (Fig 3). There was also no significant difference between the 3- and 6-month posttreatment groups (P >.05).

Total histologic healing scores for aneurysm tissues after endovascular coiling for 3 treatment-to-sacrifice time groups.
M2 Macrophages and Correlations with Collagen Deposition and Histologic Grading
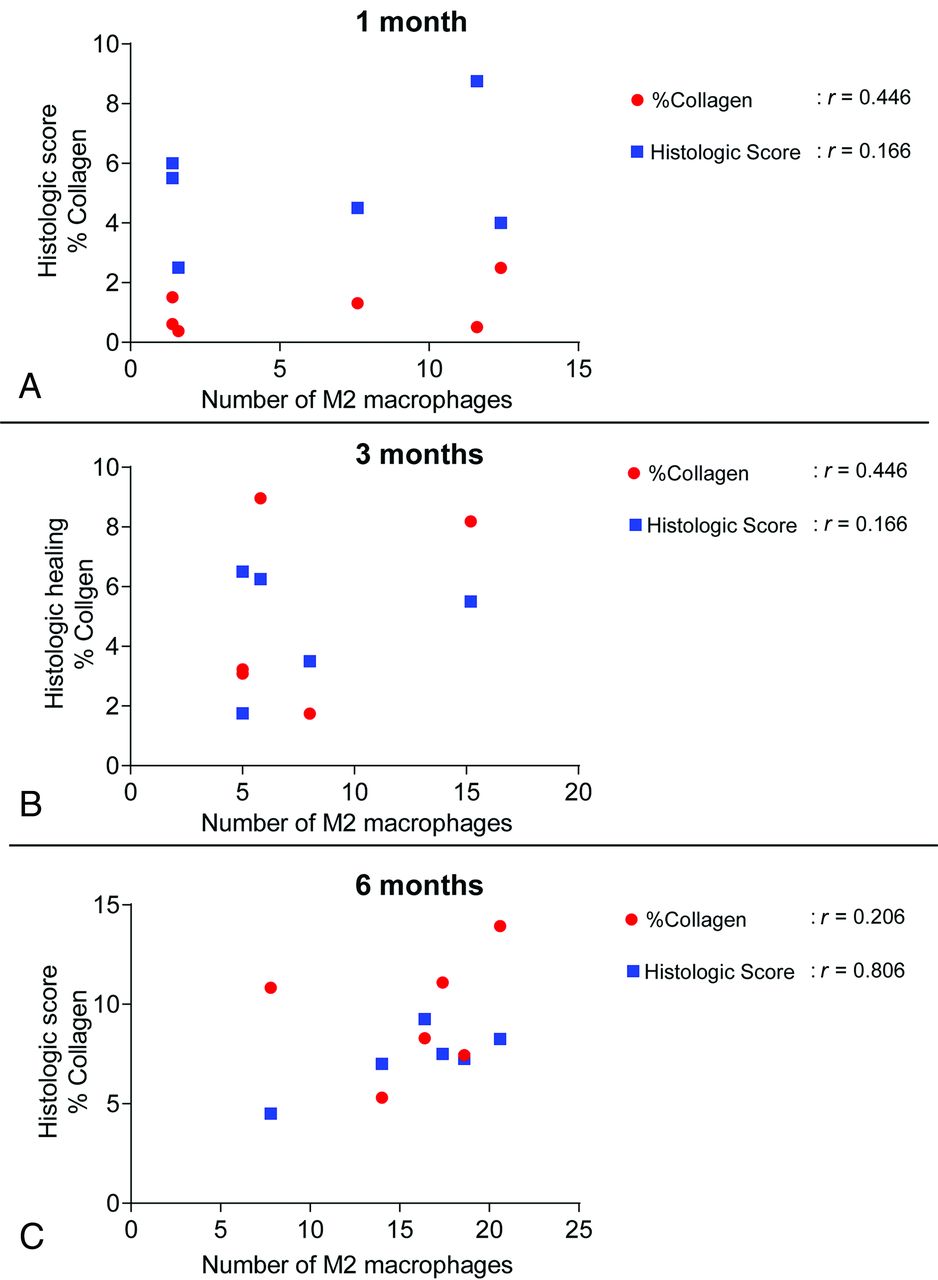
The prevalence of M2 macrophages had a moderately positive correlation with collagen deposition in both the 1-month (r = 0.450) and the 3-month (r = 0.446) posttreatment groups (Fig 4). A weak positive correlation between M2 macrophages and collagen deposition was observed in the 6-month posttreatment group (r = 0.206). M2 macrophages were strongly positively correlated with the total histologic grading score in the 6-month posttreatment group (r = 0.806); this relationship was weakly positive in the 3-month (r = 0.166) and 1-month (r = 0.323) posttreatment groups.

Correlational relationships of M2 macrophages to collagen deposition and histologic grading in aneurysm tissues after endovascular coiling for 3 treatment-to-sacrifice time groups. A, One month posttreatment. B, Three months posttreatment. C, Six months posttreatment.
DISCUSSION
In this study, we found that the presence of proinflammatory M1 macrophages in aneurysm tissues was significantly higher at 1 month after endovascular coiling compared with 3 or 6 months posttreatment. In contrast, the prevalence of anti-inflammatory M2 macrophages was highest at 6 months after endovascular coiling. These findings demonstrate that macrophage polarity is skewed toward the M1 phenotype in aneurysms on initial tissue damage, whereas M2 macrophages predominate in the later healing phases of tissue formation and remodelling.9,24 The M2 macrophage phenotype has been found to be important for promoting wound healing and tissue repair and for resolving inflammation.9 Studies have suggested that increasing the ratio of M2-to-M1 macrophages in wounds can accelerate the healing process. This has been demonstrated experimentally by reducing the effects of endogenous M1 macrophages using neutralizing antibodies or by delivering exogenous polarized M2 macrophages to stimulate wound healing in animal models.25,26 Previous approaches using proinflammatory coatings on inert platinum coils showed promise in some preclinical models,27,28 succeeding in stimulating inflammation in clinical trials but failing to reduce recurrence rates,29,30 possibly due to an unfavorable balance between M1 and M2 macrophages. Coil-mediated delivery of the proinflammatory cytokine, monocyte chemotactic protein-1, has been shown to accelerate aneurysm healing through macrophage inflammatory protein-1α and macrophage inflammatory protein-2-dependent pathways in a mouse model.27 Our findings suggest that similar interventions aimed at stimulating M2 polarization may improve aneurysm healing after treatment. However, a robust study is needed to delineate the role of M2 macrophage activation in a coil-implanted aneurysm.
We also found that the percentage of collagen deposition progressively increased with time, with statistically significant differences at both 3 and 6 months after treatment. These data are consistent with the findings of a previous study in which we reported that the aneurysm dome became acellular and vascularized with visualized connective tissue and observed increased collagen deposition 3 months after endovascular coiling.31 Additionally, we have previously demonstrated that collagen synthesis and increased histologic scores are associated with improved healing of aneurysms.19,31 One way in which M2 macrophages could be involved in this healing process is through secretion of transforming growth factor β1. Factors like transforming growth factor β1 induce the proliferation of fibroblasts, which differentiate into myofibroblasts. These cells are responsible for collagen production and closure of skin wounds.10 Thus, in this study, we evaluated any potential correlation between M2 macrophage polarity and collagen deposition. Our data demonstrate a moderate-to-weak positive correlation between M2 macrophages and collagen deposition in each of the 3 treatment-to-sacrifice time groups and a strongly positive correlation between M2 macrophages and the total histologic score at 6 months posttreatment. These findings suggest that the activity of M2 macrophages in aneurysm wound healing is not limited to collagen deposition but may also be aided by other mechanisms, such as promoting secretion of platelet-derived growth factor, chemoattractant stabilizing pericytes, extracellular matrix deposition and augmentation, and sprouting endothelial cells.24,32 In the control group, as expected, we did not find any M1 or M2 macrophages because inflammation is absent in the rabbit “untreated” aneurysm wall beyond 2 weeks following the model creation.33 Coil treatment itself increases the inflammatory response in the rabbit model.34 Our findings indicate that M1 and M2 macrophage levels are due to tissue responses to coil implants.
This study has several limitations. It focused exclusively on M1 and M2 macrophage numbers in relation to collagen deposition and total histologic scoring in coil-embolized aneurysms. We did not study the correlation between M1/M2 polarization and the recurrence rate, due to the small sample size. Furthermore, high-throughput microarray or gene profiling will facilitate a better understanding of the underlying mechanisms of the M2 phenotype switch. However, in the current preliminary work, we have only analyzed the distribution of the macrophage subtype (M1 and M2) population in the coil-treated aneurysm environment. A more in-depth study of macrophage subtypes and other immune cells involved in aneurysm healing will give us a deeper understanding of aneurysm healing after coil implantation. All of our current observations are based on animal aneurysm tissues; studying the distribution of macrophage subtypes in human aneurysm tissues will be more directly applicable for future therapeutic approaches.
CONCLUSIONS
We found that the number of M2 macrophages had a strong positive correlation with total histologic scores at a later stage of healing (6 months) after embolization treatment in a rabbit aneurysm model. This finding provides an important impetus for further studies aimed at understanding possible associations between M2 macrophages and other vascular components involved in the healing of coil-embolized aneurysms.
ACKNOWLEDGMENTS
The authors acknowledge Superior Medical Experts for editing assistance.
Footnotes
This study was supported by a grant from the National Institutes of Health (R01NS076491 and U01-NS089692) and, in part, by a fellowship award through the National Defense Science and Engineering Graduate Fellowship Program, sponsored by the Air Force Research Laboratory, the Office of Naval Research, and the Army Research Office.
Disclosures: Scott Herting—RELATED: Grant: Department of Defense, National Defense Science and Engineering Graduate Fellowship, Comments: The National Defense Science and Engineering Graduate fellowship supported me by providing tuition and stipends during graduate school. Duncan Maitland—RELATED: Grant: National Institutes of Health, Comments: National Institute of Neurological Disorders and Stroke, Grant/Award No.: U01-NS089692*; UNRELATED: Board Membership: Shape Memory Medical Inc, Comments: Shape Memory Medical Inc (shapemem.com) is commercializing neuorvascular and other vascular occlusion devices. These devices and Shape Memory Medical Inc were not involved in the work in this article. I am a cofounder and board member at Shape Memory Medical Inc; Patents (Planned, Pending or Issued): Texas A&M University and Lawrence Livermore National Laboratory, Comments: I have 40 issued patents and many pending related to vascular occlusion technology. None of the technology that I developed was part of this work; Royalties: Texas A&M University and Lawrence Livermore National Laboratory, Comments: I receive licensing royalty payments from the license of vascular occlusion technology by Shape Memory Medical Inc, paid to my former (Lawrence Livermore) and current (Texas A&M) employers. None of my licensed principal investigator was involved in this work; Stock/Stock Options: Shape Memory Medical Inc, Comments: I own stock and stock options in Shape Memory Medical Inc. Shape Memory Medical Inc was not involved in this article. David F. Kallmes—UNRELATED: Grants/Grants Pending: Medtronic, MicroVention, NeuroSigma, Neurogami, Comments: preclinical aneurysm research support.* Ram Kadirvel—RELATED: Grant: National Institutes of Health.* *Money paid to the Institution.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received March 27, 2020.
- Accepted after revision June 4, 2020.
- © 2020 by American Journal of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.