Abstract
BACKGROUND AND PURPOSE: Multichannel phased-array head coils are undergoing exponential escalation of coil element numbers. While previous technical studies have found gains in SNR and spatial resolution with the addition of element coils, it remains to be determined how these gains affect clinical reading. The purpose of this clinical study was to determine if the SNR and spatial resolution characteristics of a 32-channel head coil result in improvements in perceived image quality and lesion evaluation.
MATERIALS AND METHODS: Twenty-one patients underwent MR imaging of the brain at 1.5T sequentially with both a 12-channel and a 32-channel receive-only phased-array head coil. Axial T2WIs, T1WIs, FLAIR images, and DWIs were acquired. Anonymized images were compared side-by-side and by sequence for image quality, lesion evaluation, and artifacts by 3 neuroradiologists. Results of the comparison were analyzed for the preference for a specific head coil.
RESULTS: FLAIR and DWI images acquired with the 32-channel coil showed significant improvement in image quality in several parameters. T2WIs also improved significantly with acquisition by the 32-channel coil, while T1WIs improved in a limited number of parameters. While lesion evaluation also improved with acquisition of images by the 32-channel coil, there was no apparent improvement in diagnostic quality. There was no difference in artifacts between the 2 coils.
CONCLUSIONS: Improvements in SNR and spatial resolution attributed to image acquisition with a 32-channel head coil are paralleled by perceived improvements in image quality.
Abbreviations
- BG/IC
- basal ganglia/internal capsule
- Ch
- channel
- CN
- cranial nerve
- CNS
- central nervous system
- CP
- circularly polarized
- CS
- centrum semiovale
- DWI
- diffusion-weighted imaging
- FLAIR
- fluid-attenuated inversion recovery
- GW
- gray-white
- LV
- lateral ventricle
- MB/RN
- midbrain/red nucleus
- MCP
- middle cerebellar peduncle
- MRA
- MR angiography
- N/A
- not applicable
- NMR
- nuclear magnetic resonance
- PI
- parallel imaging
- SNR
- signal-to-noise ratio
- ST
- section thickness
- TEM
- transverse electromagnetic
- T1WI
- T1-weighted image
- T2WI
- T2-weighted image
- WMT
- white matter tracts
Multichannel receive-only coils consist of multiple-element coils arranged in various geometric schemes for uniform data acquisition from the imaging volume. Data from each coil element are received in separate radio-frequency receiver chains, which are then combined to form a final composite image.1,2 A defining characteristic of multichannel coils is typically a gain in SNR greatest at the surface.1,3,4 When coupled with multichannel receiver MR imaging scanners and PI acquisition and processing techniques, additional data from these coils can be used to fill undersampled k-space. Thus, scanning times may be accelerated without expected changes in contrast or spatial resolution.5–7 Thus, PI has been optimized for use in imaging of dynamic systems such as cardiac MR imaging to increase spatial and temporal resolution.8–11
While PI is the most common use of multichannel coils, the additional data acquired by the coil elements can be processed by standard techniques to maximize spatial resolution and SNR.1,2,12–14 Recent studies with site-specific multichannel receiver coils and more conservative acceleration of scanning times have reported improvements in diagnostic quality in nondynamic organs, such as the breast and musculoskeletal system.15–17 Consequently, there is evidence that a multichannel coil and standard processing techniques can confer some of the advantages to image quality that are characteristic of increasing field strengths.18
Thus far, few studies have evaluated the diagnostic qualities of multichannel head coils in MR imaging of the brain. Head coils in widespread use in brain MR imaging are those that have 4- to 12-element coils. In 2006, Wiggins et al14 created and tested a 32-channel receive-only phased-array head coil characterized by “soccer-ball” geometry with 32 overlapping elements. Using a 3T magnet with 32-channel capability, they compared the constructed 32-channel coil with a standard commercially available 8-channel coil. The 32-channel coil yielded 3.5-fold and 1.4-fold improvements in SNR at the cortex and corpus callosum, respectively, as well as improvements in g-factor or noise amplification during PI.
More recently, a 32-channel receive-only phased-array head coil (Siemens, Erlangen, Germany) approved by the US Food and Drug Administration has become commercially available and is in current use at our institution. As expected, reports for this coil demonstrate improvements in SNR, though improvements are not uniformly distributed. While SNR is valuable in being both objective and reproducible, this parameter has been shown to be a poor predictor of perceived diagnostic value in the evaluation of complex imaging studies.19,20 For example, if the SNR is very high, ≥100 for example, we may see little to no gain in diagnostic ability going to SNR 150 or 200 without changes in the imaging sequence or image visualization to exploit the additional SNR. SNR may also not be predictive of diagnostic performance in the presence of artifacts or other structured noise.
In other areas of the body, especially in abdominal and cardiac imaging, our experience has shown us in particular that artifacts originating from very sensitive regions of an array coil may propagate to regions of low sensitivity, thereby reducing diagnostic confidence in the low SNR regions. Thus, gains in SNR due to use of this coil may not correlate perfectly with perceived image quality, much less diagnostic quality. We, therefore, designed this prospective study of the 32-channel coil versus the 12-channel coil in MR imaging of the brain, to qualitatively compare the performance of these coils at various anatomic sites in the brain without changes to the standard protocol and image visualization. In addition, we compared artifacts and lesion evaluation between the coils. Our hypothesis was that the 32-channel coil would provide improved diagnostic value across all sequences. To test this hypothesis, we directly compared image quality, lesion evaluation, and the presence of artifacts between these 2 head coils in order to capture any changes in diagnostic value.
Materials and Methods
Patients and Scans
The institutional review board approved this study. Between July and October of 2008, 21 patients with various indications for head MR imaging were enrolled in this study. Patients were scanned on a 1.5T scanner (Magnetom Espree or Magnetom Avanto, Siemens). Scanning was performed consecutively, allowing scanning times and setup times between the 12-channel head coil (Siemens) and 32-channel head coil (Siemens). Patients were randomized to be scanned with either the 32-channel or 12-channel head coil first. Axial T1WIs, T2WIs, DWI, and FLAIR sequences were acquired with both coils. For DWI, PI (integrated parallel acquisition techniques) with a modest acceleration of 2× was used for both coils to keep scanning times within clinical guidelines set forth by our institution. Technical parameters were controlled by patients, but the radiology technicians were given latitude to accommodate patient anatomy and clinical protocols. ST remained constant at 5.0 mm. A summary of technical parameters can be found in Table 1. Additional sequences or planes were also used as clinically indicated but were not included for evaluation under this research protocol.
Technical parameters for MR imaginga
Evaluation
All images were anonymized and stripped of any technical information specific to the head coils. Three board-certified neuroradiologists (K.A.B., M.D.C., D.H.) independently performed image evaluations. Images were displayed side by side on 2 monitors of the same manufacturer and make. Additionally, monitor settings were calibrated and matched. An initial training run of 5 patients was conducted before the beginning of the study. Training consisted of an agreement between the neuroradiologists concerning the definition of the parameters for evaluation as well as the metrics. Images were evaluated for image quality, artifacts, and lesion characterization.
The parameters for image quality are listed in Table 2. Each image-quality parameter was rated by sequence, though only b = 1000 s/mm2 images were evaluated for DWI. Parameters related to image quality were compared in each study pair so that for each parameter a preference of “indistinguishable to extremely subtle change,” “subtle improvement to apparent improvement,” or “immediately apparent to marked improvement” was assigned. For the purpose of statistical analysis, a scale of −2 to +2 was used after initial scoring so that all designations in favor of the 32-channel coil were recorded as the corresponding positive integer and those favoring the 12-channel were recorded as the corresponding negative integer. For example, a designation for the 32-channel coil of “immediately apparent to marked improvement” was assigned a +2, and a lack of designation or “indistinguishable to extremely subtle change” was assigned 0. Readers rated all categories for each sequence, with the exception of DWI, in which visualization of cranial nerves and white matter tract smoothness was not rated due to inherent imaging characteristics of the sequence.
Image-quality parameters as they appeared on the evaluators' score sheets
Motion artifacts, pulsation artifacts, susceptibility artifacts, and overall artifactual degradation were also evaluated by sequence. Evaluators were then directed to lesion sites identified in the clinical reading (eg, right parietal lobe), to compare the evaluation of each lesion. Lesions sites were categorized as “cortex/subcortical white matter,” “deep brain structures,” “cerebellum and brain stem,” and “extra-axial” for data analysis only. “Cortex/subcortical white matter” was defined as the cortex, centrum semiovale, and white matter up to the internal and external capsules. “Deep brain structures” were defined as the external and internal capsules, basal ganglia, and thalami.
For lesion and artifacts evaluation, each study pair was comparatively rated as “same quality,” “better quality, no improvement in diagnostic value,” or “better quality, improved diagnostic value,” with the same numeric scale applied for statistical analysis as for image-quality parameters. Image quality and artifacts comparisons were elicited by sequence, whereas lesion-evaluation comparisons were evaluated according to the overall study to more closely simulate a clinical reading.
Data Analysis
The scores assigned by each evaluator were averaged by sequence and parameter and reported as mean ± SD. Image quality and artifacts analysis were evaluated by sequence. For lesion analysis, lesions were grouped into the aforementioned categories and each category was analyzed independently. The hypothesis that these scores were different from zero or “indistinguishable to extremely subtle change/same quality” and that the neuroradiologists preferred either head coil was tested by a 2-sided 1-sample t test by using statistical software. A P value of .05 was used to determine statistical significance.
Results
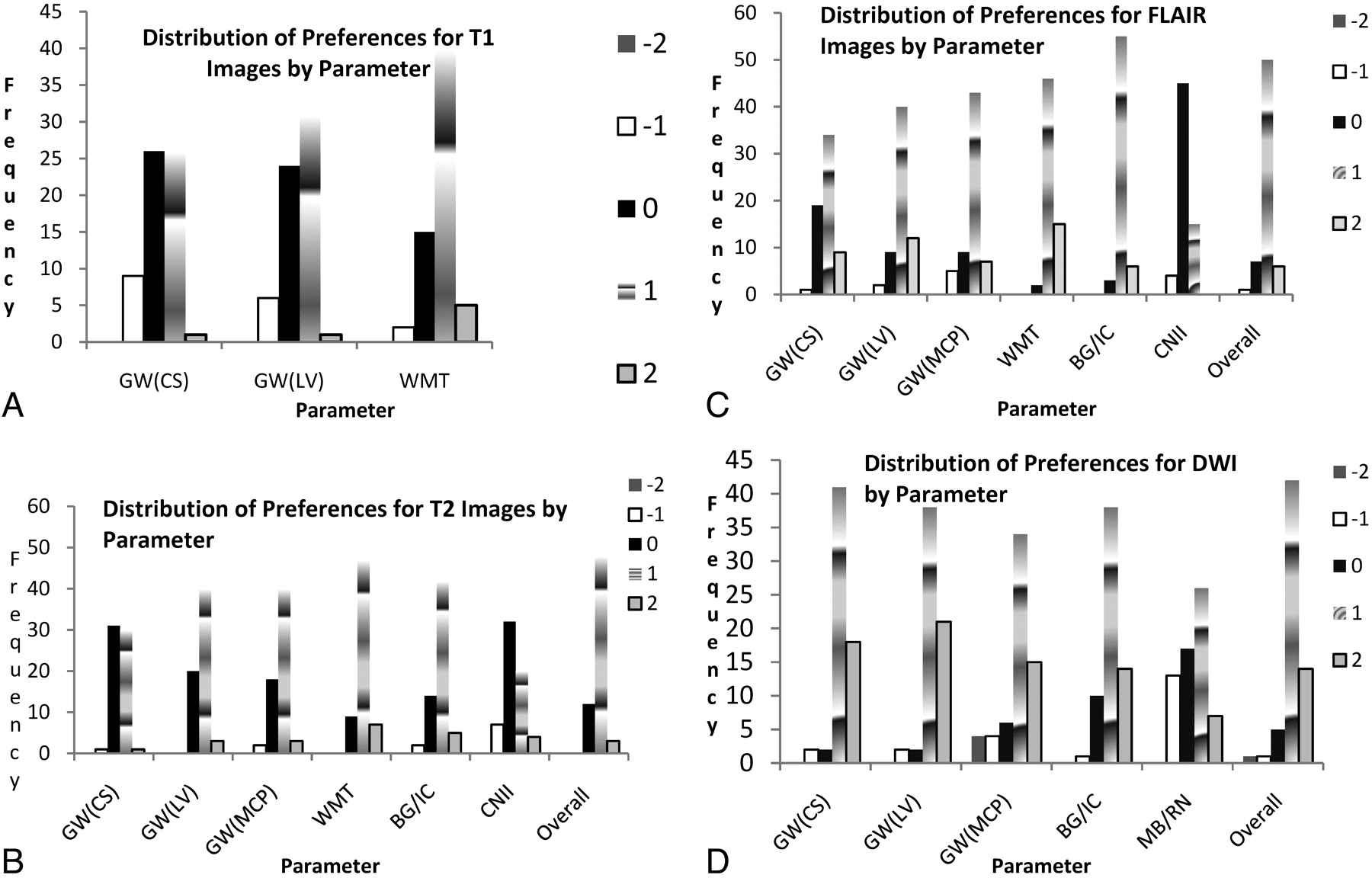
Twenty-one patients were included in the data analysis (9 men, 12 women; average age, 51.6 years). The frequencies of preferences found to be statistically significant are presented in Fig 1. A summary of statistically significant preferences can be found in Table 3, in which a preference for the 32-channel coil configuration is shown for most parameters.

Frequency of a possible 63 (3 evaluators' preferences for 21 patients) for statistically significant preferences between coils for T1 (A), T2 (B), FLAIR (C), and DWI (D) scans. 0 = “indistinguishable to extremely subtle change,” ±1 = “subtle improvement to apparent improvement,” or ±2 = “immediately apparent to marked improvement,” in which a positive integer indicates preference for the 32-channel coil and a negative integer indicates preference for the 12-channel coil. “Subtle improvement to apparent improvement” is the most common preference indicated for all significant preferences. FLAIR (C) and DWI (D) images were most likely to receive a preference of “immediately apparent to marked improvement.”
Summary of image-quality preferences by parameter and sequence
For T2WI sequences, the average rater ranking was significantly better than “indistinguishable/subtle” in favor of the 32-channel coil for gray-white differentiation at the level of the central sulcus, lateral ventricles, MCP, and internal/external capsule and basal ganglia. The mean ratings were 0.49 ± 0.33, 0.73± 0.36, 70 ± 0.39, and 79 ± 0.49 (P < .0005 for all), respectively. The overall quality, white matter smoothness, and differentiation of the optic apparatus were also significantly in favor of the 32-channel coil, with means of 0.86 ± 0.29, 0.97 ± 0.39, and 0.33 ± 0.62 (P < .0005, P < .0005, and P = .024), respectively (Fig 2). While none of these averages precisely equaled the +1 numeric designation of “subtle to apparent improvement,” the 95% confidence interval around the averages for differentiation of the internal/external capsule and basal ganglia and white matter smoothness did include this level of distinction.

T2WIs from 12-channel (A, C) and 32-channel (B, D) head coils. A and B, The 32-channel head coil images are characterized by increased gray-white matter differentiation (long arrows), smoothness of the white matter (star), and differentiation of the white matter from the basal ganglia/deep brain structures (thin arrow). C and D, Cerebellar gray-white matter differentiation is similarly improved. Contrast and edge detail are both markedly improved by the use of a 32-channel head coil (short arrows).
For T1WIs, the average rater ranking was significantly in favor of the 32-channel coil for gray-white differentiation at the levels of the central sulcus and lateral ventricles and for white matter smoothness, with means of 0.30 ± 0.56, 0.42 ± 0.52, and 0.78 ± 0.41 (P = .022, .001, and <.0005), respectively (Fig 3). There were no significant differences in artifacts or other parameters, though there was a nonsignificant preference for the 12-channel coil in differentiation of the midbrain/red nucleus and optic apparatus and the presence of motion artifacts and overall artifacts.

T1WIs from 12-channel (left) and 32-channel (right) head coils. A, Note the graininess of the white matter (arrow). B, The 32-channel head coil images display better delineation of the gray-white differentiation at both the cortex (black arrow) and basal ganglia/internal capsule (thick arrow).
Rating of FLAIR sequences revealed that the 32-channel coil was ranked significantly higher for gray-white differentiation at the levels of the central sulcus, lateral ventricles, and MCP with means of 0.81 ± 0.46, 0.98 ± 0.49, and 0.83 ± 0.60, respectively (P < .0005 for all). External/internal capsule and basal ganglia differentiation, white matter smoothness, optic apparatus, and overall quality were ranked significantly higher for the 32-channel head coil with means of 1.06 ± 0.29, 1.2 ± 0.39, 0.17 ± 0.36, and 0.96 ± 0.35 (P < .0005, <.0005, = 0.038, and <.0005), respectively (Fig 4). The numeric representation of “subtle to apparent improvement,” +1, fell within the 95% confidence interval for all of these except differentiation of the optic apparatus.

FLAIR from 12-channel (A, C, E) and 32-channel (B, D, F) head coils. A and B, There is markedly clearer gray-white matter differentiation (thin white arrow) and white matter smoothness (thick arrow) with the 32-channel head coil. C−F, Again, gray-white matter differentiation is improved at the deeper brain structures as well (arrow). Slightly different section position accounts for the difference in visibility of the discrete lesion in the left periventricular white matter.
Finally, DWI ratings were significantly in favor of the 32-channel coil in all parameters. Gray-white differentiation at the central sulcus, lateral ventricles, and MCP had means of 1.19 ± 0.39, 1.23 ± 0.38, and 0.83 ± 0.84 (P < .0005, for all), respectively. Ratings of the differentiation of the internal/external capsule and basal ganglia, midbrain and red nucleus, and overall quality had means of 1.03 ± 0.55, 0.43 ± 0.84, and 1.06 ± 0.49 (P < .0005, 0.031, and < 0.001), respectively (Fig 5). All parameters of image quality besides differentiation of midbrain and red nucleus contained the numeric representation of “subtle to apparent improvement” in the 95% confidence interval.

DWI images from 12-channel (A,C) and 32-channel (B,D) head coils. There is significant improvement in edge detail and contrast that is manifest as improvement in gray-white differentiation at the cortex (white arrow) and smooth delineation of midbrain structures.
Artifacts
There were no statistically significant preferences for motion, pulsation, or susceptibility artifacts. Overall, a difference in artifacts degradation was not apparent and did not change the diagnostic quality of the images.
Lesions
There were 41 lesions among the 21 patients. Furthermore, 25 lesions were in the cortex or subcortical white matter, 6 were in the deep brain structures, 3 were in the cerebellum or brain stem, and 7 were extra-axial. Overall, the mean preference for lesions was 0.55 ± 0.40 (P < .0005), indicating preference for the 32-channel coil configuration. The mean preference for cortical and subcortical white matter lesions was 0.65 ± 0.28 (P < .0005). The mean preference for deep brain structure lesions was 0.67 ± 0.30 (P = .0028). The mean preference for extra-axial lesions and cerebellar or brain stem lesions was nonsignificant.
Discussion
Multichannel head coils have 2 major clinical applications: 1) acceleration of scanning times without sacrifices in SNR and spatial resolution via PI techniques, and 2) improvements in spatial resolution, contrast, and SNR via standard processing. Specifically, phased-array head coils have been shown to have superior SNR profiles compared with TEM and CP head coils.21 The advantages of increasing the coil element number for phased-array coils that have been either theoretically or experimentally described are many. Significant gains in sensitivity are realized at small distances from the coils, and the addition of more coil elements reduces the sensitivity loss at farther distances.1,14,22 An initial study with a 32-channel receive-only phased-array head coil showed gains in SNR throughout the field compared with a similar 8-channel head coil.14 In contrast to the superiority of SNR profiles of phased-array coils, signal-intensity homogeneity can be slightly inferior to TEM and CP coils.21 Additionally, noise can be directly proportional to coil element numbers due to induction of current in neighboring coils (coupling) and signal averaging from each channel.14,23
The results of this study affirm that gains in SNR and spatial resolution achieved with a 32-channel receive-only phased-array head coil at 1.5T result in improvement in image quality as assessed in most regions of the brain by neuroradiologists. At the same time, the results indicate that objective gains in SNR and spatial resolution do not always or uniformly correlate with subjective preference or diagnostic value. Chapman et al (1999)19 found similar results in their evaluation of several MRA techniques. Even in the evaluation of vessels, increasing signal intensity and decreasing noise could only predict subjective preference until a certain threshold. Beyond, this threshold, raters favored more robust edge detail at the expense of objectively measured SNR.
Furthermore, objective improvements in image quality may compete with observer experiential preferences. In fact, 2 of our neuroradiologists during the initial training period found the images from the 32-channel coil to be esthetically displeasing and “cartoonlike” due to increased contrast and edge detail. Objectively, however, they did find these images to be superior as indicated by our results. Our results also indicate that while T1WIs are clinically useful in delineating anatomy, the added value of the 32-channel coil to these images in this respect was less readily apparent (Fig 3). In favorable contrast, the improvements were more readily apparent for FLAIR and T2WIs, and even more apparent for DWI, for which all parameters of image quality and delineation of anatomy improved significantly with the 32-channel coil (Fig 5).
In our study, the most drastic improvements with the 32-channel coil were seen in the DWI and FLAIR sequences in which almost all parameters of image quality were rated as “subtle to apparent improvement,” and many preferences indicated “immediately apparent to marked improvement.” In contrast, T1WIs yielded the least preference and T2WIs had more subtle improvements in several parameters.
Lesion and artifacts evaluation was an important aspect of this study because these were the only 2 sections in which direct evaluation of the overall diagnostic value of 1 coil compared with the other was possible. While images acquired by using the 32-channel coil were, on average, of better quality, only 4 of 41 lesions were rated by at least 1 neuroradiologist as having improved diagnostic value. Thus, it may be that improvements in spatial resolution, contrast, or SNR must reach a higher threshold before there is a clearer impact on the diagnostic value of the resultant images. That threshold remains to be determined in the current escalation of elements in a phased-array multichannel head coil.
An important issue identified in this study was central loss of signal intensity on 7 T1WI stacks and 1 FLAIR stack (Fig 6). The regular-shaped area of reduced signal intensity was most apparent at the level of the midbrain. As previously stated, multichannel surface coils confer gain in SNR at the surface with predictable dropoff with distance from each element coil, thus introducing signal-intensity inhomogeneity.14 Regardless, normalization of signal-intensity inhomogeneity is required to produce clinically uniform images.24 We hypothesize that the artifacts are the result of imperfect normalization in the postprocessing of these images. In fact, this was a predictable problem, and effort (though as yet not sufficient) was made to correctly normalize signal intensity before the beginning of this study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
T1WIs from 12-channel (A, C) and 32-channel (B, D) head coils showing central signal-intensity loss in the 32-channel coil. This figure is representative of the artifacts observed in several of the T1WIs. Note that section positioning is inexact, but the artifacts are apparent throughout the series.
A challenging aspect of this study relates to its design and, more specifically, the method of scaling for improvements in image quality and determination of parameters that should be evaluated. Previous studies that have qualitatively evaluated image quality in MR imaging have used scales of poor-to-excellent without direct comparison.15–17 In contrast, we aimed for a design that would directly compare differences in image quality. While direct comparison and ranking are robust and efficient, they may not necessarily reflect the diagnostic value of perceived improvements and are subject to observer bias.19 Thus, we attempted to carefully define the parameter to be compared and confirmed these definitions during the training period. When determining the parameters for evaluation, we prioritized the evaluation of both the contrast and edge detail/sharpness. We also attempted to stratify structures closest and farthest from the element coils to capture previously reported SNR characteristics.3,14
While our study design was intended to capture differences in parameters that are routinely evaluated in diagnostic neuroradiology, it may not fully extrapolate to conclusions about all aspects of diagnostic value. Although we were able to capture diagnostic value through lesion and artifacts evaluation, a study could more ideally compare lesions in a systematic manner. Examples of such studies are those that count multiple sclerosis plaques or, in musculoskeletal imaging, correlate the imaging measurements of the depth of cartilage defects to those found at dissection.17,25 Our study was also limited by section positioning, especially in the evaluation of cranial nerves and small lesions. As with all human observer studies, our study was also subject to observer bias, though we attempted to reduce this effect by standardizing the way in which disparities in section positioning and angle were handled during the training session.
Furthermore, from the results of this study, 2 additional avenues for future studies are apparent. The first avenue is to specifically investigate the utility of the 32-channel coil in specific protocols such as temporal lobe seizure, internal acoustic canal, or MRA. The second avenue is to evaluate the performance of the 32-channel coil with other sequences such as fast and ultrafast spin-echo.
Conclusions
This was an initial study of a hardware innovation in MR imaging technology that specifically evaluates the performance of a 32-channel head coil versus a 12-channel head coil at 1.5T with standard processing techniques. In this article, we have selected a defined set of parameters and a scoring scale to permit comparison between an older established coil and a newer technical improvement. We have shown that at 1.5T, compared with a 12-channel head coil, a 32-channel coil offers advantages in several image-quality parameters, most especially with FLAIR and DWI sequences, despite some identified problems. Thus, we conclude that in the clinical setting, the 32-channel phased-array head coil outperforms a 12-channel head coil across many, though not all, parameters. However, these results indicate that the potential of this coil may not be fully realized without changes to the imaging protocol and/or image-visualization methodology. This is highlighted by the results for T1WI scans here, in which little difference in diagnostic preference was noted, even though large gains in SNR were apparent in many anatomic locations. Therefore, the gains in SNR achieved through blind application of this new technology may not translate to increased diagnostic confidence. As with any new technology, we urge clinical users to fully evaluate the effort required to perform this application optimization before investing in such technology. However, our results also imply that such optimized protocols and image visualization may provide significant gains over the current clinical standards.
Footnotes
-
Indicates Fellows’ Journal Club selection

References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- Received May 7, 2010.
- Accepted after revision July 20, 2010.
- Copyright © American Society of Neuroradiology