
Abstract
Background: The definition of normal values is a prerequisite for the reliable evaluation of abnormality in the lumbar spine, such as spinal canal stenosis or dural ectasia in patients with Marfan syndrome. Values for vertebral body diameter (VBD) and dural sac diameter (DSD) for the lumbar spine have been published in adults. In children, normal values have been established using conventional radiography or myelography, but not by MRI. Objective: To define normal values for the sagittal diameter of the vertebral body and dural sac, and to calculate a dural sac ratio (DSR) in the lumbosacral spine (L1–S1) in healthy children using MRI. Materials and methods: A total of 75 healthy children between 6 years and 17 years of age were examined using a sagittal T2-weighted sequence. Sagittal VBD and DSD were measured and a DSR was calculated. This was a retrospective and cross-sectional study. Results: With increasing age there is a significant increase of VBD, a slight increase of DSD, and a slight decrease of DSR. There is no significant sex difference. DSR in healthy children is higher than in healthy adults. Conclusions: MRI is a reliable method demonstrating the natural shape of the lumbosacral spine and its absolute values. These normal values compare well with those established by conventional radiological techniques. Our data may serve as a reference for defining dural ectasia in children with Marfan syndrome.
Similar content being viewed by others


Introduction
Evaluation of lumbar spine abnormality is nowadays routinely established by using MRI or CT. Historically, normal dimensions of the paediatric lumbar spine were established by conventional radiography [1, 2], or myelography for the cervical and thoracic spine [3]. Conflicting data exist for the age-dependant increase of the sagittal diameter of the lumbar spine [1, 2]. Some studies state an age-dependant increase for the dimensions of the lumbar spine [1], while other studies deny this age dependency, discussing different methodological factors, such as magnification [2]. Normal values for the dimensions of the paediatric lumbar spine as demonstrated by MRI or CT are lacking. Therefore, the aim of this study was to establish reliable values by a digital technique that circumvents the methodological problems of magnification.
Some pathological entities of the lumbar spine, such as spinal canal stenosis or lumbar dural ectasia in patients with Marfan syndrome or neurofibromatosis manifest even in early childhood [4–7]. In order to improve our understanding of these diseases, the aim of this study was to define normal values of the lumbar spine in healthy children between 6 years and 17 years of age.
Materials and methods
Study population
Sagittal diameters of the lumbar spine (vertebral body and dural sac) were measured in 75 healthy children (32 boys, 43 girls) between 6 years and 17 years of age. The children were referred for MRI of the lumbosacral spine for routine clinical indications (e.g. back pain, rheumatic disorders, traumatic or other orthopaedic reasons). An exclusion criterion was a pathologic process of the lumbosacral spine, particularly scoliosis. Data sets were also excluded when the patient was not exactly positioned along the sagittal axis. The study group was divided into four groups according to age: 6–8, 9–11, 12–14 and 15–17 years. The study was cross-sectional and retrospective.
MRI
All examinations were obtained using a 1.5-T MRI (Siemens Symphony, Erlangen, Germany). Since the evaluation was performed retrospectively, we selected T2-weighted sagittal images to measure the vertebral body diameter (VBD) and dural sac diameter (DSD). Slice thickness was 4 mm in all examinations.
Measurements
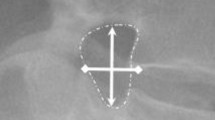
All measurements were performed by one radiologist (C.K.) at a workstation (J-Vision, Tiani Co., Vienna, Austria). The diameters were obtained at each level of the lumbar vertebral column (L1–L5) and at the level of the first sacral vertebral body (S1). Measurements were made perpendicular to the long axis of the vertebral body and the dural sac (Fig. 1). The landmarks for the measurement of VBD were the anterior and posterior border at the middle of each vertebral body (at the level of vessel entry). The DSD was measured as the longest distance between the posterior border of the vertebral body and the anterior border of the spinous process. We calculated the dural sac ratio (DSR) as the quotient of DSD to VBD in the different age groups. For all data the mean (±SD) were calculated. A P-value of less than 0.05 was considered to indicate a significant difference.

Example of measurement VBD and DSD in a healthy child
Results
The mean and standard deviation of the sagittal VBD and DSD of the lumbar spine and the first sacral vertebral body in children between 6 and 17 years of age are presented in Tables 1 and 2. There was no significant difference between the sexes (P>0.05) (Fig. 2). For further analysis, we divided our patients into four age groups 6–8, 9–11, 12–14 and 15–17 years. In all age groups there is a decrease of DSD from L1 to L3, followed by a slight increase at the level of L4 to L5, and a large decrease at the level S1, resulting in the lowest diameter of the dural sac at S1 (Fig. 3). We observed a slow increase of the DSD (Fig. 3) during growth with a difference Δ=+0.8 mm every 3 years up to the age of 14 years, which afterwards is reduced to a difference of Δ=+0.03 mm in children older than 14 years (Table 1).

Sagittal DSD and VBD of the lumbar spine from L1 to S1 in children between 6 years and 17 years, mean and standard deviation are given. No significant difference between the sexes could be detected

Sagittal DSD and sagittal VBD of the lumbar spine from L1 to S1 calculated for different age groups, mean and standard deviation are given
Regarding the VBD (Table 2), there is an increase from L1 to L3 in all age groups with a peak at L3 or L4. Beyond L5 there is a slight decrease of VBD, followed by a significant decrease at S1 (Fig. 3). The growth of the vertebral bodies from L1 to S1 is Δ=+2.4 to +2.7 mm (mean) every 3 years between 6 years and 14 years of age (P<0.05 at all levels). In children older than 14 years the growth is reduced to a Δ=+0.75 mm over 3 years (P<0.05 at L1) (Table 2).
For this reason the DSR is comparable to the absolute values of the diameters of the lumbar spine from L1 to S1. The DSR decreases from L1 to L3 (Fig. 4) due to the increase of VBD and decrease of DSD (Fig. 3). The DSR at L3 and L4 are at their minimum, while there is an increase at L5 and S1 (Fig. 4). During growth, DSR decreases by approximately 10% every 3 years (Table 3).

Ratio of dural sac diameter to vertebral body diameter (DSR) of the lumbar spine from L1 to S1 calculated for different age groups, mean and standard deviation are given
Discussion
The aim of this study was to establish normal values for the sagittal diameter of the vertebral body and dural sac of the lumbar spine in children using MRI. In adults, there have been some historical anatomical investigations concerning the normal anatomy of the lumbar vertebral column by Huizinga et al. [8] and Eisenstein [9]. For the paediatric age group, conventional radiographic evaluation of the lumbar spinal canal was undertaken by Hinck et al. [1] and Larsen and Smith [2], while anatomical studies of the lumbar spinal canal were performed by Papp et al. [10]. Brandner [11] defined normal values of the vertebral body during growth using conventional radiographic techniques. To our knowledge our study is the first presenting normal values of the lumbar vertebral column in the paediatric age group performed by MRI.
As mentioned before, for adult and paediatric patients [1, 2, 8, 9, 10], our data reflect the natural shape of the lumbar spine. There is an increase of the VBD from L1 to L3, with maximum VBD at L3 or L4, a slight decrease of VBD at L5 and a big decrease of VBD at S1 (Fig. 3). In contrast, the DSD reflects a mirror-like image of VBD with a decrease from L1 to L3 or L4, followed by a slight increase at L5, that does not reach the highest values of L1 (Fig. 3). At S1 there is a parallel decrease of VBD and DSD to the lowest absolute values (Fig. 3).
Our data for DSD are comparable to those of Larsen and Smith [2] and Papp et al. [10] with a difference of approximately 1 mm between L1 and L5 (Fig. 5). Compared to the spinal canal sagittal diameters published by Larsen and Smith, the DSD in our series were lower in the 6–8-year age group, increasing in the age groups 9–11 years and 12–14 years (Fig. 3). Therefore, we conclude that with increasing age there is a slight increase in DSD. In contrast, Papp et al. [10] concluded that mid-sagittal growth of the lumbar spinal canal is complete at L1–L5 by 4 years of age. The values for the lumbar spinal canal found by Hinck et al. [1] were higher in all age groups and at all levels (Fig. 5). The reason for the differences between the data of Hinck et al. [1] and our data for the DSD may be attributed to errors caused by magnification, as discussed by Larsen et al. [2]. MRI is not affected by the problem of magnification.

Comparison of normal values for lumbar spinal canal diameter respectively. DSD published by different authors
VBD increases significantly with increasing age (P<0.05). Brandner [11] also described this age-related growth of VBD [11], although the absolute values for L1 were higher than ours. Therefore, DSR decreases with increasing age, because VBD increases more rapidly than DSD (Fig. 4).
The upper limit of DSR may serve to define pathological entities such as dural ectasia in patients with Marfan syndrome (Fig. 1). Compared to the cut off values for normal DSRs published by Oosterhof et al. [12] our DSR values in the different age groups were higher (Table 3). Therefore, the incidence of dural ectasia in children with Marfan syndrome may be overestimated using the cut-off values defined for adult patients [12]. Further studies are needed to compare DSD and DSR values of patients with Marfan’s syndrome with normal subjects.
Conclusions
Normal values for the sagittal diameter of the vertebral body and dural sac in the lumbosacral spine, and the DSR from L1 to S1, as measured by MRI, have been defined in healthy children between 6 years and 17 years of age. The data reflect the natural shape of the vertebral column with an increase of the vertebral body dimensions from L1 to L3 with a maximum at L3 or L4, and a decrease at L5 and S1. Dural sac dimensions mirror the vertebral body dimensions.
References
Hinck VC, Hopkins CE, Clark WM (1965) Sagittal diameter of the lumbar spinal canal in children and adults. AJR 96:929–937
Larsen JK, Smith D (1981) The lumbar spinal canal in children. Part 1: the sagittal diameter. Eur J Radiol 1:163–170
Boltshauser E, Hoare RD (1976) Radiographic measurements of the normal spinal cord in childhood. Neuroradiology 10:235–237
Fattori R, Nienaber CA, Descovich B et al (1999) Importance of dural ectasia in phenotypic assessment of Marfan’s syndrome. Lancet 354:910–913
Jamjoom ZA, Malabarey T, Kolawole TM et al (1990) Lumbosacral dural anomalies in von Recklinghausen neurofibromatosis. Acta Neurochir 105:140–146
Schonauer C, Tessitore E, Frascadore L et al (2000) Lumbosacral dural ectasia in type 1 neurofibromatosis. Report of two cases. J Neurosurg Sci 44:165–168
Katz SG, Grunebaum M, Strand RD (1978) Thoracic and lumbar dural ectasia in a two-year-old boy. Pediatr Radiol 6:238–240
Huizinga J, Heiden JA, Vinken PJ (1951) The human lumbar vertebral canal. A biometric study. P K Ned Akad Wetensc 55:22–33
Eisenstein S (1977) The morphometry of pathological anatomy of the lumbar spine in South African negroes and caucasoids with specific reference to spinal stenosis. J Bone Joint Surg Br 59:173–180
Papp T, Porter RW, Aspden RM (1994) The growth of the lumbar vertebral canal. Spine 19:2770–2773
Brandner ME (1970) Normal values of the vertebral body and intervertebral disk index during growth. Am J Roentgenol Radium Ther Nucl Med 110:618–627
Oosterhof T, Groenink M, Hulsmans FJ et al (2001) Quantitative assessment of dural ectasia as a marker for Marfan syndrome. Radiology 220:514–518
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Knirsch, W., Kurtz, C., Häffner, N. et al. Normal values of the sagittal diameter of the lumbar spine (vertebral body and dural sac) in children measured by MRI. Pediatr Radiol 35, 419–424 (2005). https://doi.org/10.1007/s00247-004-1382-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-004-1382-6