Abstract
Purpose
Valve surgery for active infective endocarditis (IE) can cause fatal brain hemorrhage. Our current study aimed to evaluate the incidence of septic cerebral lesions in active IE patients by performing preoperative magnetic resonance imaging (MRI) including T2*- weighted sequences and magnetic resonance angiography (MRA) before urgent valve surgery, and to investigate whether such preoperative evaluation affects postoperative outcomes.
Methods
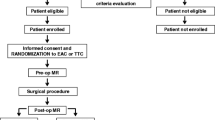
Eighteen patients were referred to our department for native valve IE during 2006–2010. Urgent surgery was indicated in cases of hemodynamic failure resulting from valve destruction, refractory sepsis, and mobile vegetations measuring >10 mm. For these patients, we performed preoperative MRI and MRA.
Results
Males comprised 67% of the subjects, with average age 53 ± 15 years. No clinical evidence of acute stroke was noted. Of the 18 patients, urgent surgery was indicated in 15; of these, 10 (67%) showed a brain lesion related to IE: 6 patients had acute or subacute brain infarctions, 2 patients had brain infarction with brain abscess, and 2 patients had hemorrhagic brain infarction and so did not undergo urgent surgery. Thus, 13 patients underwent urgent valve surgery. Among the 5 patients who did not undergo urgent surgery, 4 patients later underwent valve surgery for healed IE. No hospital deaths or neurological complications occurred.
Conclusion
MRI of patients with active IE revealed a high incidence of cerebral lesions caused by IE. The use of MRI to detect septic embolism and intracerebral hemorrhage may provide important information for better surgical outcomes.
Similar content being viewed by others


References
Vilacosta I, Graupner C, San Roman JA, Sarria C, Ronderos R, Fernández C, et al. Risk of embolization after institution of antibiotic therapy for infective endocarditis. J Am Coll Cardiol 2002;39:1489–1495.
Salgado AV, Furlan AJ, Keys TF, Nickols TR, Beck GJ. Neurologic complications of endocarditis: a 12-year experience. Neurology 1989;39:173–178.
Hart RG, Foster JW, Luther MF, Kanter MC. Stroke in infective endocarditis. Stroke 1990;21:695–700.
Kanter MC, Hart RG. Neurologic complications of infective endocarditis. Neurology 1991;41:1015–1020.
Thuny F, Avierinos JF, Tribouilloy C, Giorgi R, Casalta JP, Milandre L, et al. Impact of cerebrovascular complication on mortality and neurologic outcome during infective endocarditis: a prospective multicentre study. Eur Heart J 2007;28:1155–1161.
Atlas SW, Mark AS, Grossmann RI, Gomori JM. Intracranial hemorrhage: gradient-echo MR imaging at 1.5 T. Comparison with spin-echo imaging and clinical applications. Radiology 1988;168:803–807.
Offenbacher H, Fazekas F, Schmidt R, Koch M, Fazekas G, Kapeller P. MR of cerebral abnormalities concomitant with primary intracerebral hematomas. AJNR Am J Neuroradiol 1996;17:573–578.
Netzer RO, Zollinger E, Seiler C, Cerney A. Infective endocarditis: clinical spectrum, presentation and outcome. An analysis of 212 cases 1980–1995. Heart 2000;84:25–30.
Mylonakis E, Calderwood SB. Infective endocarditis in adults. N Engl J Med 2001;345:1318–1330.
Hoen B, Alla F, Selton-Suty C, Beguinot I, Bouvet A, Briançon S, et al. Changing profile of infective endocarditis: results of a 1-year survey in France. JAMA 2002;288:75–81.
Beynon RP, Bahl VK, Prendergast BD. Infective endocarditis. Br Med J 2006;333:334–339.
Murdoch DR, Corey GR, Hoen B, Miro JM, Fowler VG Jr, Bayer AS, et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med 2009;169:463–473.
Ruttmann E, Willeit J, Ulmer H, Chevtchik O, Hofer D, Poewe W, et al. Neurological outcome of septic cardioembolic stroke after infective endocarditis. Stroke 2006;37:2094–2099.
Piper C, Wiemer M, Schulte HD, Horstkotte D. Stroke is not a contraindication for urgent valve replacement in acute infective endocarditis. J Heart Valve Dis 2001;10:703–711.
Cooper HA, Thompson EC, Laureno R, Fuisz A, Mark AS, Lin M, et al. Subclinical brain embolization in left-sided infective endocarditis: results from the evaluation by MRI of the brains of patients with left-sided intracardiac solid masses (EMBOLISM) pilot study. Circulation 2009;120:585–591.
Shang E, Forrest GN, Chizmar T, Chim J, Brown JM, Zhan M, et al. Mitral valve infective endocarditis: benefit of early operation and aggressive use of repair. Ann Thorac Surg 2009;87:1728–1734.
Horstkotte D, Follah F, Gutshik E, Lengvel M, Oto A, Pavie A, et al. Guidelines on prevention, diagnosis, and treatment of infective endocarditis: the task force on infective endocarditis of European Society of Cardiology. Eur Heart J 2004;25:267–276.
Subramaniam S, Puetz V, Dzialowski I, Barber BA. Cerebral microhemorrhages in a patient with mycotic aneurysm: relevance of T2-GRE imaging in SBE. Neurology 2006;67:1697.
Klein I, Iung B, Wolff M, Brochet E, Longuet P, Laissy JP, et al. Silent T2* cerebral microbleeds: a potential new imaging clue in infective endocarditis. Neurology 2007;68:2043.
Klein I, Iung B, Labreuche J, Hess A, Wolff M, Messika-Zeitoun D, et al. Cerebral microbleeds are frequent in infective endocarditis: a case-control study. Stroke 2009;40:3461–3465.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Takagi, Y., Higuchi, Y., Kondo, H. et al. The importance of preoperative magnetic resonance imaging in valve surgery for active infective endocarditis. Gen Thorac Cardiovasc Surg 59, 467–471 (2011). https://doi.org/10.1007/s11748-011-0777-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-011-0777-1