
Abstract
Introduction
The reported intracerebral hemorrhage rate due to ventriculostomy placement varies widely. As studies emerge regarding alternative techniques of ventriculostomy placement, and placement by non-neurosurgeons, further definition of the true intracerebral hemorrhage rate associated with ventriculostomy is warranted. We performed a meta-analysis of the existing literature to further elucidate the incidence of intracerebral hemorrhage due to ventriculostomy.
Methods
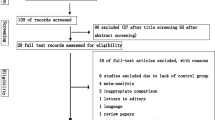
We performed an extensive literature search using Ovid MEDLINE and PubMed for relevant studies published after 1970. Only studies with more than 25 ventriculostomy procedures were included. Data were extracted regarding number of hemorrhages, clinically significant hemorrhages, and the use of routine post-ventriculostomy CT scanning. We performed subgroup analyses based on the use of routine post-ventriculostomy CT scanning. Chi-squared test was used to determine statistical significance.
Results
Overall, 102 hemorrhagic complications from 1,790 ventriculostomies were reported, a hemorrhage rate of 5.7%. Of the 102 hemorrhages, 11 were clinically significant (clinically significant hemorrhage rate = 0.61%). In studies that used routine post-placement CT scans, the hemorrhage rate was 10.06%, compared to a hemorrhage rate of 1.53% in studies in which routine CT scans were not performed (P < 0.001). Eight clinically significant hemorrhages (0.91%) were identified in the studies utilizing routine post-procedural CT scanning, compared to three clinically significant hemorrhages (0.33%) in studies without routine CT scans (P = 0.113).
Conclusion
The overall hemorrhage risk associated with ventriculostomy placement based on the existing literature is 5.7%. Clinically significant hemorrhage due to ventriculostomy is less than 1%. Modifications of technique that might reduce hemorrhage risk, and the utility of routine post-procedural CT scanning, merit further investigation.

Similar content being viewed by others

References
Maniker AH, et al. Hemorrhagic complications of external ventricular drainage. Neurosurgery. 2006;59(4 Suppl 2):ONS419–24; discussion ONS424–5.
Leung GK, et al. Extended subcutaneous tunnelling technique for external ventricular drainage. Br J Neurosurg. 2007;21(4):359–64. doi:10.1080/02688690701392881.
Guyot LL, et al. Cerebral monitoring devices: analysis of complications. Acta Neurochir Suppl (Wien). 1998;71:47–9.
Paramore CG, Turner DA. Relative risks of ventriculostomy infection and morbidity. Acta Neurochir (Wien). 1994;127(1–2):79–84. doi:10.1007/BF01808552.
North B, Reilly P. Comparison among three methods of intracranial pressure recording. Neurosurgery. 1986;18(6):730–2. doi:10.1097/00006123-198606000-00009.
Rhodes TT, et al. External ventricular drainage for initial treatment of neonatal posthemorrhagic hydrocephalus: surgical and neurodevelopmental outcome. Pediatr Neurosci. 1987;13(5):255–62. doi:10.1159/000120339.
Anderson RC, et al. Complications of intracranial pressure monitoring in children with head trauma. J Neurosurg. 2004;101(Suppl 1):53–8.
Ehtisham A, et al. Placement of external ventricular drains and intracranial pressure monitors by neurointensivists. Neurocrit Care. 2008. doi:10.1007/s12028-008-9097-4.
Khanna RK, et al. Prolonged external ventricular drainage with percutaneous long-tunnel ventriculostomies. J Neurosurg. 1995;83(5):791–4.
Roitberg BZ, et al. Bedside external ventricular drain placement for the treatment of acute hydrocephalus. Br J Neurosurg. 2001;15(4):324–7. doi:10.1080/02688690120072478.
Friedman WA, Vries JK. Percutaneous tunnel ventriculostomy. Summary of 100 procedures. J Neurosurg. 1980;53(5):662–5.
Narayan RK, et al. Intracranial pressure: to monitor or not to monitor? A review of our experience with severe head injury. J Neurosurg. 1982;56(5):650–9.
Wiesmann M, Mayer TE. Intracranial bleeding rates associated with two methods of external ventricular drainage. J Clin Neurosci. 2001;8(2):126–8. doi:10.1054/jocn.2000.0749.
Hassler W, Zentner J. Ventricle puncture for external CSF drainage and pressure measurement using a modified puncture needle. Acta Neurochir (Wien). 1988;94(1–2):93–5. doi:10.1007/BF01406623.
Vieweg U, Kaden B, Van Roost D. A flexible metal ventricular catheter for treatment of complicated and protracted infections of the cerebrospinal fluid spaces: preliminary experiences. Acta Neurochir (Wien). 1996;138(12):1431–6. doi:10.1007/BF01411122.
Bogdahn U, et al. Continuous-pressure controlled, external ventricular drainage for treatment of acute hydrocephalus—evaluation of risk factors. Neurosurgery. 1992;31(5):898–903; discussion 903–4. doi:10.1097/00006123-199211000-00011.
Acknowledgment
The authors are deeply indebted to Mrs. Margaret Anderson and Mrs. Gale Hannigan for their assistance with this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Binz, D.D., Toussaint, L.G. & Friedman, J.A. Hemorrhagic Complications of Ventriculostomy Placement: A Meta-Analysis. Neurocrit Care 10, 253–256 (2009). https://doi.org/10.1007/s12028-009-9193-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-009-9193-0