Article Text

Abstract
Background There is wide variability in the reported incidence of perioperative thromboembolic (0–14%) and hemorrhagic (0–11%) complications after Pipeline Embolization Device (PED) procedures for cerebral aneurysm treatment, which could be partly due to differences in patient response to the P2Y12 receptor antagonist administered while the PED endothelializes. This study aims to identify an optimal pre-procedure P2Y12 reaction units (PRU) value range and determine the independent predictors of perioperative thromboembolic and hemorrhagic complications after PED procedures.
Methods We recorded patient and aneurysm characteristics, P2Y12 receptor antagonist administered, pre-procedure PRU value with VerifyNow, procedural variables and perioperative thromboembolic and hemorrhagic complications up to postoperative day 30 after PED procedures at our institution during an 8-month period. Perioperative complications were considered major if they caused a permanent disabling neurological deficit or death. Multivariate regression analysis was performed to identify independent predictors of perioperative complications in our cohort.
Results Forty-four patients underwent 48 PED procedures at our institution during the study period. There were eight thromboembolic and hemorrhagic perioperative complications in our cohort (16.7%), four of which were major (8.3%). A pre-procedure PRU value of <60 or >240 (p=0.02) and a technically difficult procedure (p=0.04) were independent predictors of all perioperative complications. A pre-procedure PRU value of <60 or >240 (p=0.004) and a history of hypertension (p=0.03) were independent predictors of major perioperative complications.
Conclusions In our cohort, a pre-procedure PRU value of <60 or >240 was the strongest independent predictor of all and major perioperative thromboembolic and hemorrhagic complications after PED procedures.
- Aneurysm
- Platelets
- Flow Diverter
- Hemorrhage
- Stroke
Statistics from Altmetric.com
Introduction
The novel concept of cerebral aneurysm treatment by flow diversion with the Pipeline Embolization Device (PED; Covidien/ev3, Irvine, California, USA) constitutes a significant paradigm shift in the field of endovascular treatment of cerebral aneurysms, which was previously limited to endosaccular therapy with coils or liquid embolic agents.
Flow diversion requires deployment of the PED(s) within the lumen of the parent artery to allow the vessel to endothelialize along the PED and exclude the aneurysm from the circulation. This process carries the risk of thromboembolic complications since platelets could become activated, adhere to the PED, form thrombus and cause either in situ PED thrombosis or distal embolization. Hence, PED procedures are usually performed under dual antiplatelet therapy (DAT) with aspirin and a P2Y12 receptor antagonist such as clopidogrel, prasugrel or ticagrelor. However, DAT carries the risk of hemorrhagic complications, with parenchymal intracerebral hemorrhage (ICH) being the most potentially devastating. Case series of 12–191 patients treated with the PED have reported a wide range of perioperative thromboembolic and hemorrhagic complications, with the risk of cerebral infarction in the range 0–14% and the risk of ICH in the range 0–11%.1–15 Among other factors, the variability in perioperative thromboembolic and hemorrhagic complications after PED procedures could be due in part to differences in the response of patients to the P2Y12 receptor antagonists used while the PED endothelializes. However, no studies have systematically examined the predictors of perioperative thromboembolic and hemorrhagic complications in this patient population.
The P2Y12 receptor plays a central role in platelet activation and aggregation. Clopidogrel and prasugrel cause irreversible inhibition of the P2Y12 receptor, while ticagrelor causes reversible inhibition of this receptor. VerifyNow (Accumetrics, San Diego, California, USA) is a point-of-care platelet function test that measures the degree of P2Y12 receptor inhibition after stimulation with ADP, a P2Y12 receptor agonist. This assay has been found to correlate strongly with light transmittance aggregometry, the gold standard for quantification of platelet reactivity, in patients treated with clopidogrel, prasugrel or ticagrelor.16–19 VerifyNow results are reported in P2Y12 reaction units (PRU), with a lower PRU value corresponding to a higher degree of P2Y12 receptor inhibition and, hence, a decreased likelihood of platelet activation and aggregation. Previously, VerifyNow also reported a ‘P2Y12 percent inhibition’ by measuring ‘base reaction units’ and comparing it with the PRU value; however, since August 2012, VerifyNow reports the PRU value only. Among neurointerventionalists performing the VerifyNow test for PED procedures, a ‘P2Y12 percent inhibition’ of 30–40% was generally used as a minimum degree of pre-procedure P2Y12 receptor inhibition required.10 ,12 ,20 However, there is no clear maximum degree of pre-procedure P2Y12 receptor inhibition desired for PED procedures. To date, no studies have attempted to determine an optimal pre-procedure PRU value range that could potentially minimize the risk of perioperative thromboembolic and hemorrhagic complications after PED procedures.
The aim of this study is to identify an optimal pre-procedure PRU value range and determine the independent predictors of perioperative thromboembolic and hemorrhagic complications in a cohort of patients undergoing treatment of cerebral aneurysms with the PED.
Methods
We conducted a retrospective analysis to examine the predictors of perioperative thromboembolic and hemorrhagic complications in patients who underwent treatment of cerebral aneurysms with the PED at our institution from 17 November 2011 until 23 July 2012.
Medical record review
We recorded baseline patient characteristics, P2Y12 receptor antagonist used, P2Y12 receptor inhibition with the VerifyNow test (in PRUs), aspirin dose, aneurysm characteristics, number of PEDs deployed, technical complications, procedure time, post-procedure corticosteroid regimen and the incidence and severity of perioperative thromboembolic and hemorrhagic complications occurring up to postoperative day 30. Procedures were considered technically difficult if there was PED herniation into the aneurysm, incomplete PED opening requiring balloon angioplasty for adequate wall apposition, PED migration during deployment requiring a second PED to cover the aneurysm neck or concurrent treatment of another cerebral aneurysm. Perioperative thromboembolic and hemorrhagic complications were reviewed by a panel of three neurointerventionalists and were designated as major if they caused a permanent disabling neurological deficit or death.
DAT protocol
P2Y12 receptor inhibition was assessed with the VerifyNow test in all patients before the procedure as well as 10 and 30 days after any changes to the dose or type of the P2Y12 receptor antagonist administered, or at any time if symptomatic with abnormal bruising/bleeding or focal neurological deficits.
For the majority of elective PED procedures (83%), DAT was started 10 days before the procedure with 325 mg aspirin daily and 75 mg clopidogrel daily. The clopidogrel response was assessed the day before the procedure, with a target P2Y12 receptor inhibition of 80–200 PRUs. Clopidogrel hyporesponders (PRU>200) received a 60 mg prasugrel loading dose the day before the procedure followed by 10 mg prasugrel daily, and the initial prasugrel response was assessed on the day of the procedure. Clopidogrel hyperresponders (PRU<80) were placed on every other day, every third day, every Monday and Friday or every fifth day dosing regimens as needed to reach the target PRU range. Prasugrel hyporesponders (PRU>200) received a 180 mg ticagrelor loading dose followed by 90 mg twice a day with the initial ticagrelor response assessed before the procedure. Prasugrel hyperresponders in follow-up testing (PRU<80) initially had the daily prasugrel dose reduced to 5 mg and, if needed, were subsequently placed on every other day or every third day dosing regimens in order to reach the target PRU range. Although the aforementioned adjustments to the dose or type of the P2Y12 receptor antagonist administered were made according to the pre-procedure PRU value, elective PED procedures were not rescheduled to a later date in order to reach the target PRU range prior to PED deployment.
For urgent/emergent PED procedures, a 60 mg prasugrel loading dose was administered followed by 10 mg prasugrel daily with the initial prasugrel response assessed before the procedure and follow-up testing performed as described above.
PED procedure
The PED procedure was performed under general anesthesia by a team of two neurointerventionalists using transfemoral access in a dedicated biplanar neuroangiographic unit (Axiom Artis, Siemens, Munich, Germany). Heparinization was used throughout the procedure to achieve an activated clotting time 2–2.5×baseline. A triaxial system was used with a 6 Fr long sheath (Shuttle; Cook Medical, Bloomington, Indiana, USA), distal access catheter (Reflex, Covidien/ev3 or Neuron; Penumbra, Alameda, California, USA) and Marksman microcatheter (Covidien/ev3). A 0.016 inch (Headliner; Terumo, Tokyo, Japan) or 0.014 inch (Traxcess; MicroVention, Tustin, California, USA or Avigo; Covidien/ev3) microwire was used to advance the Marksman microcatheter across the aneurysm neck. The PED device was deployed across the aneurysm neck under fluoroscopic guidance. A post-deployment Dyna-CT angiogram was performed to ensure adequate PED vessel wall apposition and aneurysm neck coverage. Final biplanar angiography was performed to document patency of the intracranial vasculature.
Statistical analysis
Statistical analysis was performed using the MedCalc 11.1 software package (MedCalc Software, Mariakerke, Belgium). We first performed univariate analysis with χ2 or Fisher exact tests for each variable to identify the predictors of all and major perioperative thromboembolic and hemorrhagic complications in our cohort. Multivariate regression analysis was then performed to identify the independent predictors of all and major perioperative thromboembolic and hemorrhagic complications in our cohort. A p value of ≤0.05 was considered statistically significant.
Results
From 17 November 2011 until 23 July 2012, 44 patients underwent 48 PED procedures to treat 54 cerebral aneurysms at our institution; 36 patients were women (81.8%) and there were eight men (18.2%). Their mean age was 59.2 years (median 63 years, range 31–81). Seven patients had a remote history of subarachnoid hemorrhage (15.9%) and 10 had a family history of cerebral aneurysms (22.7%). Ten aneurysms were symptomatic (18.5%), 11 had recurred after coiling (20.4%) and 27 were incidental (50%). The mean maximum aneurysm size was 8.4 mm (median 5.8 mm, range 1.9–27.6) and the mean aneurysm neck size was 4.8 mm (median 4 mm, range 1.1–17). The mean procedure time was 67.7 min (median 50.5 min, range 28–220). Seventeen procedures were technically difficult (35.4%), with a mean procedure time of 108.7 min (median 91 min, range 56–220). The mean number of PEDs deployed was 1.3 (range 1–5).
The mean pre-procedure PRU value was 111.7 (median 101.5, range 5–275). Two patients were started on prasugrel for urgent/emergent PED procedures (4.5%). Eleven patients were considered clopidogrel hyporesponders (26.2%, PRU>200), with a mean PRU of 272.8 (median 262, range 207–399); of note, these patients had a mean ‘P2Y12 percent inhibition’ of 13.5% (median 11%, range 0–31%). Nine patients were considered clopidogrel hyperresponders (21.4%, PRU<80), with a mean PRU of 48.1 (median 54, range 9–73); of note, these patients had a mean ‘P2Y12 percent inhibition’ of 83.8% (median 81%, range 72–97%).
Perioperative thromboembolic and hemorrhagic complications and associated PRU values
Table 1 summarizes the incidence of perioperative thromboembolic and hemorrhagic complications in our cohort according to three pre-procedure PRU value ranges using a pre-procedure PRU value of >240 as a proposed cut-off for P2Y12 receptor under-inhibition21 and a pre-procedure PRU value of <60 as a proposed cut-off for P2Y12 receptor over-inhibition.
Perioperative thromboembolic and hemorrhagic complications after treatment of cerebral aneurysms with the Pipeline Embolization Device (PED) by pre-procedure PRU value
There were four thromboembolic (8.3%) and four hemorrhagic (8.3%) perioperative complications in our cohort. Of these, four were major (8.3%): three resulted in a permanent disabling neurological deficit (6.3%, one thromboembolic, two hemorrhagic) and one ICH resulted in death (2.1%).
The four thromboembolic complications were: one patient with numerous infarctions ipsilateral to the PED on postoperative day 1 causing permanent disabling contralateral hemiparesis (figure 1); one patient with small pontine and cerebellar infarctions distal to the PED on postoperative day 2 causing transient hand weakness and ataxia; one patient with several frontoparietal infarctions ipsilateral to the PED on postoperative day 6 causing transient word-finding difficulty; and one patient with transient aphasia on postoperative day 0 without associated diffusion-weighted imaging abnormalities. Patency of the PED construct at the time of the complication was confirmed with CT angiography in all cases. Three thromboembolic complications (75%), including the one major complication, occurred after technically difficult procedures. Two thromboembolic complications (50%), including the one major complication, occurred shortly after the procedure in clopidogrel hyporesponders who received an additional 150 mg clopidogrel dose immediately before the procedure and had the daily clopidogrel dose increased to 150 mg thereafter without rescheduling the procedure to a later date in order to reach the target PRU range prior to PED deployment. Of note, the patient who experienced the major thromboembolic complication had a markedly elevated PRU value (292) at the time of the complication.

A 79-year-old patient with a history of hypertension presented with a 2-year history of diplopia and right cranial nerve III and VI palsies. The patient was considered a clopidogrel hyporesponder with a pre-procedure P2Y12 reaction units (PRU) value of 262 on the day of the procedure after seven 75 mg doses of clopidogrel. The patient received an additional 150 mg clopidogrel immediately before the procedure and the daily clopidogrel dose was increased to 150 mg thereafter. (A) Three-dimensional image showing a 16 mm fusiform right cavernous internal carotid artery (ICA) aneurysm. (B) Fluoroscopic image after deploying two Pipeline Embolization Devices (PEDs) showing a stenosis within the second PED which improved after balloon angioplasty (arrowhead). (C) Final lateral right ICA angiogram showing contrast stasis in the aneurysm (arrowhead) and patent cerebral vasculature. Procedure time was 97 min. (D) The patient developed left-sided hemiparesis on postoperative day 1. Diffusion-weighted image demonstrates numerous thromboembolic infarctions in the right cerebral hemisphere. PRU was 292 at the time of the thromboembolic complication. The patient was discharged with permanent disabling left-sided hemiparesis.
The four hemorrhagic complications were all ICHs ipsilateral to the PED: two patients with large basal ganglia ICHs on postoperative days 14 and 20 causing permanent disabling contralateral hemiplegia (figure 2), one patient with a large temporal ICH on postoperative day 4 causing brain herniation and death (figure 3) and one patient with a frontal ICH on postoperative day 8 causing transient expressive aphasia. No patient reported focal neurological deficits before the ICH. All ICHs occurred in patients with a history of hypertension after treatment of internal carotid artery (ICA) aneurysms (mean size 16 mm, median 15.5 mm, range 7.5–25.4). Three hemorrhagic complications (75%), including two of the three major complications, occurred after technically difficult procedures. All three major hemorrhagic complications occurred in clopidogrel hyporesponders who were either switched to prasugrel the day before the procedure (two patients) or had the clopidogrel dose increased to 150 mg prior to the procedure (one patient) without rescheduling the procedure to a later date in order to reach the target PRU range prior to PED deployment. Of note, 75% of hemorrhagic complications, including two of the three major complications, occurred in patients who had markedly decreased PRU values shortly before (PRU 0) or at the time of the ICH (PRU 2, 10). There was a trend towards a higher likelihood of major hemorrhagic complications in patients undergoing PED procedures on aspirin/prasugrel DAT (16.7%) versus aspirin/clopidogrel DAT (2.9%, p=0.16).

A 69-year-old patient with a history of hypertension presented with a 5-month history of diplopia and right cranial nerve VI palsy. The patient was considered a clopidogrel hyporesponder with a P2Y12 reaction units (PRU) value of 259 on the day before the procedure after nine 75 mg doses of clopidogrel. The patient received a 60 mg prasugrel loading dose the day before the procedure followed by a daily 10 mg dose. The pre-procedure PRU was 8 on the day of the procedure. (A) Three-dimensional image showing a 21 mm fusiform right cavernous internal carotid artery (ICA) aneurysm. (B) Fluoroscopic image after deploying two Pipeline Embolization Devices (PEDs) showing construct failure with herniation into the aneurysm sac (arrowheads). The aneurysm was ultimately treated with four PEDs. (C) Final lateral right ICA angiogram showing contrast stasis in the aneurysm (arrowhead) and patent cerebral vasculature. Procedure time was 193 min. (D) Follow-up P2Y12 receptor inhibition test on postoperative day 10 showed a PRU of 0, which was confirmed on repeat testing. Prasugrel was held for 3 days and the daily dose was decreased to 5 mg thereafter. In the evening of postoperative day 13 the patient was found to be less interactive by family members but did not seek medical attention. In the early afternoon of postoperative day 14 the patient experienced left-sided hemiplegia. Non-contrast CT shows a large right basal ganglia intracerebral hemorrhage. The patient was discharged with permanent disabling left-sided hemiplegia.
{kind=link}
{kind=link}
{kind=link}
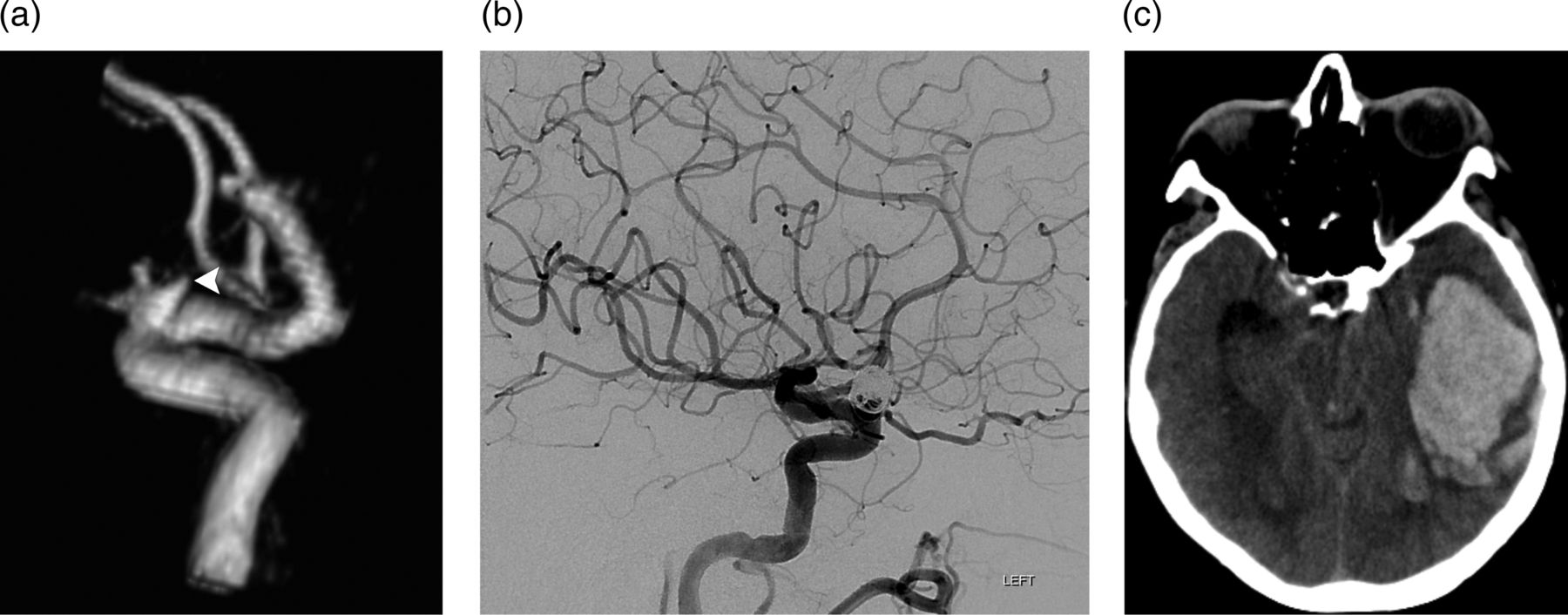
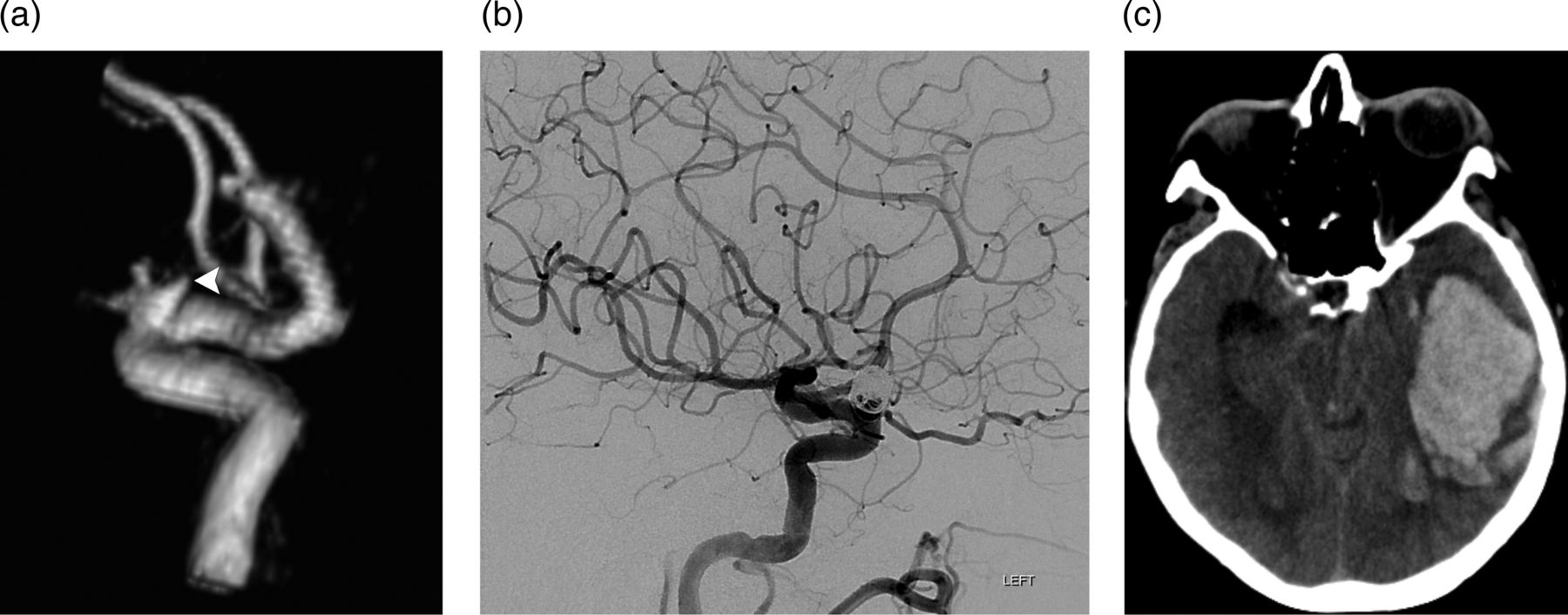
A 70-year-old patient with a history of hypertension presented with a recurrent left ophthalmic internal carotid artery (ICA) aneurysm 5 years after coil embolization. The patient was considered a clopidogrel hyporesponder with a P2Y12 reaction units (PRU) value of 246 3 days before the procedure after receiving nine 75 mg doses of clopidogrel. The daily clopidogrel dose was increased to 150 mg thereafter without repeat P2Y12 receptor inhibition testing before the procedure. (A) Three-dimensional image showing the recurrent left ophthalmic ICA aneurysm (arrowhead). The ophthalmic artery arises from the anterior aspect of the aneurysm sac. (B) Final lateral left ICA angiogram after uncomplicated deployment of a single Pipeline Embolization Device showing patent cerebral vasculature. Procedure time was 30 min. (C) On postoperative day 4 the patient was found unresponsive at home. Non-contrast CT shows a large left temporal intracerebral hemorrhage causing left uncal herniation. PRU was 10 at the time of the hemorrhage. The patient died that evening.
Overall, among the four major perioperative thromboembolic and hemorrhagic complications in our cohort, all occurred in patients who were considered clopidogrel hyporesponders and underwent changes to the dose or type of the P2Y12 receptor antagonist administered before the procedure without rescheduling the procedure to a later date in order to reach the target PRU range prior to PED deployment; three (75%) occurred after technically difficult procedures and three (75%) occurred in patients who had markedly elevated (292, thromboembolic complication) or markedly decreased (0, 10, hemorrhagic complications) PRU values shortly before or at the time of the complication.
Predictors of perioperative thromboembolic and hemorrhagic complications after PED procedures
Table 2 summarizes the predictors of perioperative thromboembolic and hemorrhagic complications in our cohort. In multivariate regression analysis, a pre-procedure PRU value of <60 or >240 (p=0.02) and a technically difficult procedure (p=0.04) were independent predictors of all perioperative complications. A pre-procedure PRU value of <60 or >240 (p=0.004) and a history of hypertension (p=0.03) were independent predictors of major perioperative complications.
Predictors of perioperative thromboembolic and hemorrhagic complications after treatment of cerebral aneurysms with the Pipeline Embolization Device (PED)
Discussion
The overall incidence of perioperative thromboembolic (8.3%) and hemorrhagic (8.3%) complications after PED procedures in our cohort is within the range of previously published studies (0–14% and 0–11%, respectively).1–15 The overall risk of major perioperative complications causing a permanent disabling neurological deficit or death in our cohort was 8.3%, which is higher than the risk of serious complications associated with endosaccular aneurysm treatment with coils (approximately 3–4%). However, the target patient population for PED procedures is usually those with large and wide-necked aneurysms, which are either not treatable by coil embolization or are at an increased risk of recurrence requiring multiple treatments. Nevertheless, the higher risk of major perioperative thromboembolic and hemorrhagic complications associated with flow diversion must be strongly considered when offering this treatment modality to patients with potentially coilable or clippable cerebral aneurysms.
The proportion of clopidogrel hyporesponders in our cohort (26% using a PRU>200 cut-off or 21% using a PRU>240 cut-off) is lower than that reported by Akbari et al20 (32.9%) and Lee et al22 (42.9%) in patients also tested with VerifyNow using a <40% ‘P2Y12 percent inhibition’ cut-off. In our experience, the ‘base reaction units’ previously reported with VerifyNow fluctuated in serial testing of the same patient and yielded variations in the reported ‘P2Y12 percent inhibition,’ while we found the PRU value to be more reliable in serial testing. To illustrate this point, 10 patients in our cohort underwent at least three VerifyNow tests within a 7-day period: we found that, in a given patient, the difference between the highest and lowest ‘base reaction units’ value reported constituted approximately 25% of the average ‘base reaction units’ value reported in the serial tests. These fluctuations in the ‘base reaction units’ value could potentially cause wide variations in the reported ‘P2Y12 percent inhibition’ despite a stable PRU value. Indeed, VerifyNow no longer reports ‘base reaction units’ or ‘P2Y12 percent inhibition’ and reports the PRU value only. In our cohort, all major thromboembolic and hemorrhagic complications occurred in patients who were considered clopidogrel hyporesponders and underwent changes to the dose or type of the P2Y12 receptor antagonist administered before the procedure without rescheduling the procedure to a later date in order to reach the target PRU range prior to PED deployment.
We found an increased risk of major hemorrhagic complications after PED procedures in patients on aspirin/prasugrel DAT (16.7%) versus aspirin/clopidogrel DAT (2.9%). Our results are similar to those of Akbari et al20 in patients undergoing various types of neurointerventional procedures under aspirin/prasugrel DAT (19.4%), although they are in disagreement with those of Stetler et al23 in a smaller cohort of patients (0%). Hence, while prasugrel is a very effective P2Y12 receptor antagonist and may be an alternative for clopidogrel hyporesponders, this may be at the expense of an increased risk of major hemorrhagic complications. Although aspirin/ticagrelor DAT could be a safer alternative to aspirin/prasugrel DAT for clopidogrel hyporesponders, further research on its safety in this specific patient population is needed.
The important issue of P2Y12 receptor over-inhibition in patients undergoing PED procedures has not been well examined in the literature. In our cohort, 21% of patients were considered clopidogrel hyperresponders in pre-procedure P2Y12 receptor inhibition testing using a cut-off of PRU<80 (using a cut-off of PRU <60, 14% of patients would have been considered clopidogrel hyperresponders). While the etiology of ICHs ipsilateral to the PED is probably multifactorial, P2Y12 receptor over-inhibition in the perioperative period could play a role. In our cohort, three of the four patients (75%) with perioperative ICHs were found to have markedly decreased PRU values (0, 2, 10) at the time of or just prior to the ICH. A recent study of 133 coil embolization procedures to treat unruptured cerebral aneurysms reported a 30% rate of peri-procedural thromboembolic diffusion-weighted imaging-positive lesions within 72 h of the intervention.24 Furthermore, a recent pathological study of three patients who suffered fatal ICHs after PED procedures demonstrated basophilic material occluding the blood vessels around the ICH,25 which may represent the hydrophilic coating of the catheters or wires used in these procedures. It is therefore plausible that some of the ICHs encountered after PED procedures could be explained by hemorrhagic transformation of subclinical infarctions caused by embolization of air bubbles, atherosclerotic plaque dislodged during catheterizations, thrombus formed on the devices used over the course of the procedure or hydrophilic coating from the catheters or wires used to deploy the PED, in the setting of P2Y12 receptor over-inhibition.
In our cohort, a pre-procedure PRU value of <60 or >240 and a technically difficult procedure were independent predictors of all perioperative thromboembolic and hemorrhagic complications, and a pre-procedure PRU value of <60 or >240 and a history of hypertension were independent predictors of major perioperative thromboembolic and hemorrhagic complications. Hence, it is plausible that P2Y12 receptor under-inhibition or over-inhibition in the perioperative period may place patients at risk of developing thromboembolic or hemorrhagic complications, respectively, particularly if the procedure is technically difficult or if the patient is prone to experiencing blood pressure fluctuations. Future research is needed to determine if active perioperative blood pressure control and P2Y12 receptor antagonist management to maintain patients within a target P2Y12 receptor inhibition range (PRU 60–240), including rescheduling patients who are outside this range in pre-procedure testing in order to make the P2Y12 receptor antagonist adjustments needed to reach the target PRU range prior to PED deployment, could lower the risk of thromboembolic and hemorrhagic complications after PED procedures.
Following the findings of our study, we have changed our DAT protocol for PED procedures (table 3). Due to the increased risk of major perioperative hemorrhagic complications, we no longer administer prasugrel to patients considered clopidogrel hyporesponders. While we have expanded our target PRU range to 60–240, PED deployment for elective cases is not undertaken until the patient is within the target PRU range in pre-procedure P2Y12 receptor inhibition testing performed no earlier than the day before the procedure (given our retrospective data, we expect to reschedule 35.7% of patients). Patients undergoing urgent/emergent PED procedures are started on ticagrelor before the procedure (180 mg×1, then 90 mg twice a day) without P2Y12 receptor inhibition testing and are transitioned to clopidogrel on postoperative day 30 following the protocol described in table 3. Further, all patients are admitted to the neurological intensive care unit for monitoring, a brain MRI with diffusion-weighted imaging is performed on postoperative day 1 and blood pressure is strictly controlled in the perioperative period (goal ≤140 mm Hg systolic).
Current dual antiplatelet therapy protocol for Pipeline Embolization Device procedures
The limitations of our study are the modest sample size, retrospective design and lack of PED procedures performed with pre-procedure PRU values in the 201–240 range (nonetheless, to date we have performed one PED procedure with a pre-procedure PRU value of 239 without encountering perioperative thromboembolic complications).
Conclusions
There were four major perioperative thromboembolic and hemorrhagic complications after PED procedures in our cohort (8.3%). All major perioperative complications occurred in patients who were considered clopidogrel hyporesponders and underwent changes to the dose or type of the P2Y12 receptor antagonist administered before the procedure without rescheduling the procedure to a later date in order to reach the target PRU range prior to PED deployment, and three (75%) occurred in patients who had markedly elevated (292, thromboembolic complication) or markedly decreased (0, 10, hemorrhagic complications) PRU values shortly before or at the time of the complication. A pre-procedure PRU value of <60 or >240 was the strongest independent predictor of all and major perioperative thromboembolic and hemorrhagic complications after PED procedures in our cohort.
Acknowledgments
The authors would like to acknowledge Sandee K Verootis, Radiology Department, Abbott Northwestern Hospital for her contribution to the data collection for this study.
Footnotes
-
Contributors JEDA: study conception and design, data collection, statistical analysis, data analysis and interpretation, manuscript preparation, responsible for the overall content as guarantor of the study. BMC: study conception and design, data collection, data interpretation, manuscript revision. JMS: study conception and design, data collection, data interpretation, manuscript revision. JLF: study design, data collection, data analysis, manuscript revision. REA: study design, data collection, manuscript revision. YK: study design, statistical analysis, data analysis and interpretation, manuscript preparation. DET: study conception, data interpretation, manuscript revision.
-
Competing interests JEDA, BMC and DET have consulting relationships with Covidien/ev3. None of the other authors has potential conflicts of interests pertaining to this research project.
-
Ethics approval The study was approved by the Abbott Northwestern Hospital institutional review board and was conducted in compliance with the Health Insurance Portability and Accountability Act.
-
Provenance and peer review Not commissioned; externally peer reviewed.