Article Text

Abstract
Background and purpose Treatment of intracranial fusiform aneurysms is complex and controversial, and is associated with high morbidity and mortality rates. The goal of this study was to evaluate the strategy of stent only therapy.
Materials and methods A retrospective analysis of 20 patients with 20 intracranial fusiform aneurysms undergoing endovascular treatment using stent only therapy was undertaken. Feasibility, safety, and angiographic follow-up were evaluated.
Results 28 Leo Plus stents were successfully deployed in 20 patients. No technical difficulties in relation to stent navigation, placement, or detachment from the delivery system were observed. A 6 month, 1 year, and 2 year follow-up angiograms were performed in all patients. 15 aneurysms showed complete occlusion and five partial stable occlusion. During the follow-up period, there was no evidence of in-stent stenoses or occlusion of the incorporated branching vessels. In this study, no patient presented with subarachnoid hemorrhage or died during follow-up.
Conclusions Stent only therapy in this study proved very useful as a flow diverter for the treatment of intracranial fusiform aneurysms in which parent artery occlusion or stenting–coiling was not feasible.
- Aneurysm
- Balloon
- Catheter
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Fusiform intracranial aneurysms are circumferential dilatations of a cerebral artery without an ostium or neck, with an incidence of less than 1% of all intracranial aneurysms. Usually they progressively enlarge over time. The pathologic etiology of fusiform aneurysms is partial or total absence of the internal elastic lamina and/or media, either congenital or acquired, which reduces elastic wall tension and allows subsequent expansion of the vessel diameter over time.
These aneurysms are commonly located in the supraclinoidal internal carotid artery, the vertebral artery (VA) or the basilar artery. Although the etiology of these aneurysms remains unclear, some authors have suggested that underlying atherosclerotic disease and recurrent arterial dissections secondary to hypertension may be involved.1 ,2 These lesions may present symptoms related to mass effect, ischemia secondary to dissection involving perforated branches or thromboembolic events, and subarachnoid hemorrhage (SAH).
Treatment of these aneurysms is complex and remains controversial. Until recently, the only definitive treatment was complete trapping of the aneurysm by endovascular coiling or surgical clipping, entailing high morbidity and mortality rates. The development of self-expandable intracranial stents for the endovascular treatment (EVT) of complex aneurysms has enabled the preservation of the affected parent artery, altering intra-aneurysm flow dynamics leading to thrombus formation within the aneurysm. Thus this innovative endovascular option involves significant changes in the therapeutic strategy. Initial clinical experience in this setting consisted of treating intracranial fusiform aneurysms with high porosity stents and then placing coils through the pores of the stent into the most dilated section of the lesion.3
Recent studies have reported a small series of fusiform aneurysms effectively treated by stent only therapy.4–6
Thus the purpose of this study was to retrospectively evaluate the feasibility, safety, and efficacy of stent only therapy for intracranial fusiform aneurysms.
Materials and methods
Patients
This retrospective study consisted of 197 consecutive patients with 211 aneurysms treated in our hospital between May 2008 and May 2011. For 20 patients (13 women and seven men; average age 57.2 years, range 38–79 years) with fusiform aneurysms, EVT was considered to be the therapeutic treatment of choice by the multidisciplinary neurosurgical, neurological, and neurointerventional team, taking into account collateral blood supply, as determined by balloon test occlusion, aneurysm localization, surgical accessibility, branches arising from the aneurismal wall, and patient preference.
The most common clinical presentation was transient ischemic attacks (10/20), symptoms related to mass effect (7/20), and SAH (3/20). Aneurysms were located in the posterior cerebral vascular territory (75%) and the anterior cerebral vascular territory (25%). Six of the vertebrobasilar fusiform aneurysms involved a branching vessel of the posterior inferior cerebellar artery or anterior inferior cerebellar artery (table 1).
Clinical and imaging outcome
Therapeutic strategy and endovascular procedure
All patients received clopidogrel (75 mg/day) and aspirin (150 mg/day) for at least 7 days before the procedure. Three patients with a minimum 4 month history of HSA who were referred to our unit received the same premedication.
All procedures were performed under general anesthesia and therapeutic heparinization with activated clotting times of approximately 300 s. Patients were kept on heparin for at least 24 h. All procedures were performed by a senior interventional neuroradiologist with extensive experience in intracranial stent placement techniques.
A 6 F guide (Envoy; Cordis, Miami Lakes, Florida, USA) was introduced into the internal carotid artery or VA via femoral access. Through the guiding catheter, a 0.21–0.28 Vasco microcatheter (Balt, Montmorency, France) was navigated on a Synchro 0.14 inch microwire (Boston Scientific, West Valley, Utah, USA) distally to the aneurysm with a sufficient margin for maneuver to facilitate stent navigation, positioning, and liberation.
Stent diameter and length were selected by three-dimensional angiography, and stent length was determined as 30% longer than the aneurysm neck length. When measurements were complicated due to vessel tortuosity, the length of the stent was determined with the aid of a microwire. The Leo Plus stent has been designed to combine high radial force and easy delivery. It is made of braided nitinol wires, and there are two highly radiopaque platinum wires that run the entire length of the stent that ensure visibility of both diameter and length. The Leo stent has an innovative distal hook that allows for resheathing and repositioning of the stent when as much as 90% deployed. The Leo stents are available in diameters of 2.5–7.5 mm and lengths of 12–50 mm. The stent, with its open cell design, is similar to the Neuroform (Boston Scientific/Target, Natick, Massachusetts, USA) but contains a modified geometry with three connectors between adjacent segments, providing a 39% decrease in the area of the open cells. A Leo Plus stent (Balt) was used given its differential characteristics in relation to other types of stent (wider range of diameters and lengths, continuous surface coverage, visualization of both diameter and length, and a delivery system allowing for stent resheating and repositioning even when it is 90% deployed). In cases requiring overlapping stents, the number was determined according to the location, tortuosity of the parent artery, and control angiogram findings following deployment of the first stent.
Immediate postprocedural angiography was performed to assess the degree of exclusion of the aneurysm and the patency of the arteries incorporated into the aneurysmal dilatation. Angiographic findings were classified as either complete occlusion (no contrast agent filling the aneurysmal sac) or incomplete occlusion (residual contrast agent filling the aneurysm sac). Six, 12, and 24 month follow-up angiograms were undertaken in all patients.
Periprocedural and postoperative complications such as thromboembolism, parent artery occlusion, rebleeding, in-stent thrombosis, in-stent stenosis, and retroperitoneal hematoma were evaluated. According to the protocol for intracranial stent placement in our hospital, all patients underwent an MRI between 24 and 48 h post procedure.
Patients with unruptured aneurysms were clinically assessed on admission using the modified Rankin Scale score, and patients with HSA were clinically graded using the Hunt and Hess grading system. Clinical outcome was evaluated at discharge and during clinical follow-up using the modified Rankin Scale.
Results
A total of 28 stents were successfully deployed in 20 patients. There were no technical difficulties in terms of stent navigation, placement, or detachment from the delivery system. Stent shortening was observed in three vertebrobasilar fusiform aneurysms that required overlapping stents to ensure endovascular remodeling. There was no stent shrinkage beyond the limits outlined by the manufacturer.
One patient suffered intra-stent thrombosis during the procedure that was resolved by administering a standard intra-arterial abciximab bolus (ReoPro; Eli Lilly) and intra-stent angioplasty. Three patients had a minor stroke, as documented by diffusion weighted MRI. Two patients had femoral hematoma, and another patient had a renal hematoma. Hematomas were resolved without complications.
Immediately following stent placement, significant flow reduction and stagnation of blood within the aneurysm lumen were observed.
Six month, 1 year, and 2 year follow-up angiograms were performed on all patients. Final follow-up angiogram, at 24 months, showed complete occlusion in 15 aneurysms and five with partial stable occlusion.
No evidence of in-stent stenosis by hyperplasia or occlusion of the jailed perforating vessels in the stent treated portion of the vessel was observed during follow-up. In this study, there were no cases of SAH or fatalities during follow-up.
Illustrative cases
Case No 1
A 61-year-old patient presented with diplopia as a clinical sign of brainstem compression slowly progressing over at least the past 6 weeks. A cerebral angiographic study showed the presence of a non-thrombosed fusiform aneurysm involving the terminal VA V4 segments on both sides and the proximal two-thirds of the basilar artery (figure 1A, B). First, two overlapping stents (Leo stent 5.5×45 mm and 4.5×40 mm) were deployed (figure 2A, B) and immediate angiographic control showed significant flow reduction within the sac. Three months later, the patient was rescheduled for endovascular coil occlusion of the left VA V4 segment distal to the posterior inferior cerebellar artery (figure 2C). Control angiography performed at 6 months showed complete aneurysm occlusion with preservation of all basilar artery branches (figure 2D). Clinically, the patient had a normal neurological examination and had remained asymptomatic thereafter.
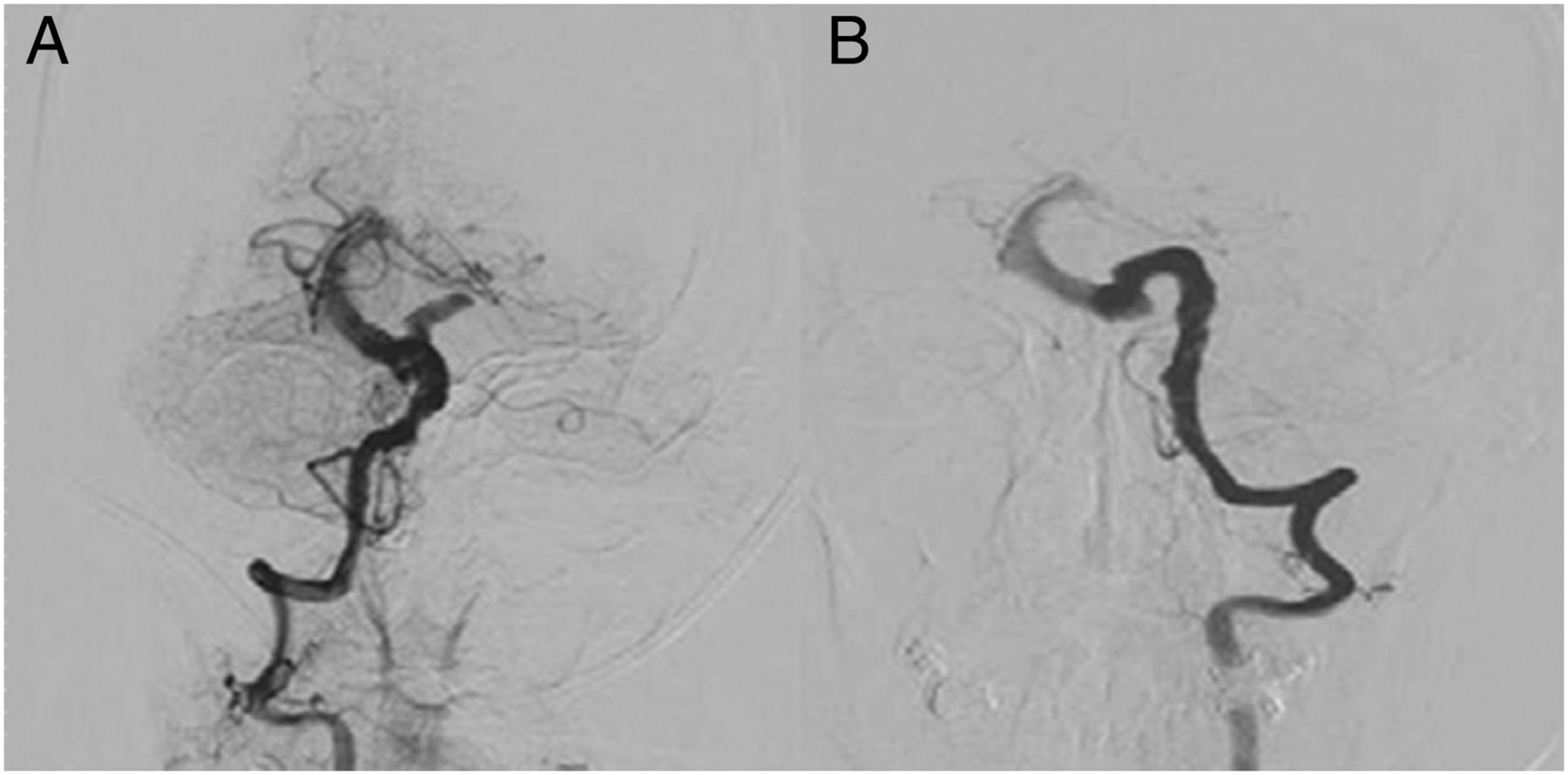
Conventional angiography of the right vertebral artery (VA) (A) and left VA (B), showing a fusiform aneurysm of the basilar artery (BA) involving the terminal VA segments on both sides and the proximal two-thirds of the BA.

Angiogram acquired at the end of endovascular treatment (A) and coronal multiplanar reformatting from bolus enhanced CT angiography (B), showing two overlapping Leo stents along the aneurysm. At 3 months, the patient was rescheduled for endovascular coil occlusion of the left vertebral artery distal to the posterior inferior cerebellar artery (C). Angiogram acquired at 6 months showed marked remodeling of the vessel with minimal residual aneurysm (D).
Case No 2
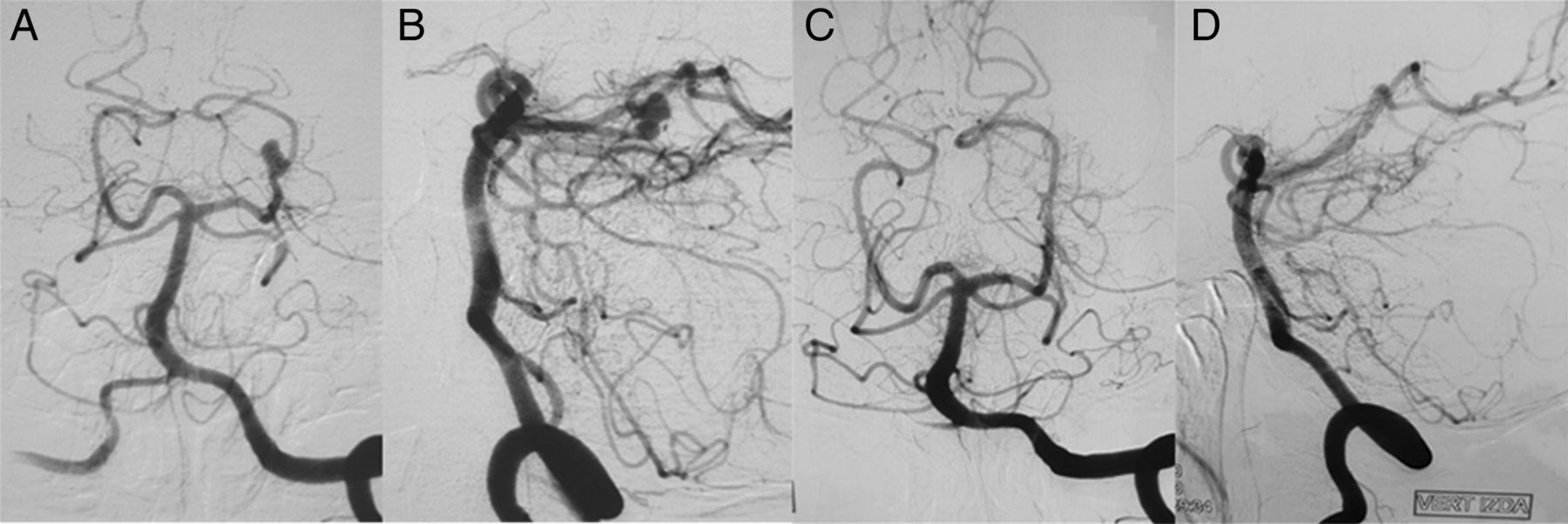
A young woman aged less than 40 years presented with headache of 2 days’ duration. A CT scan of the head demonstrated findings consistent with SAH. On angiography, a fusiform aneurysm of the left posterior cerebral artery (PCA) was noted.
Catheter angiography was performed under conscious sedation and confirmed the presence of a left first and second segment (P2) PCA aneurysm (figure 3A, B). The patient underwent reconstructive endovascular repair of the fusiform aneurysm by stent placement (2.5 mm/18 mm Leo Plus stent) across the PCA aneurysm neck without complications. Follow-up control angiography at 6 months showed complete aneurysm occlusion (figure 3C, D). The patient was found to be neurologically intact at follow-up visits at 12, 24, and 36 months.

Anteroposterior (A) and lateral (B) digital subtraction angiographic images of the left vertebral artery showing a fusiform left posterior cerebral artery aneurysm. Anteroposterior (C) and lateral (D) angiograms acquired at 6 months after placement of the intracranial stent show complete disappearance of the aneurysm and preservation of the parent artery.
Case No 3
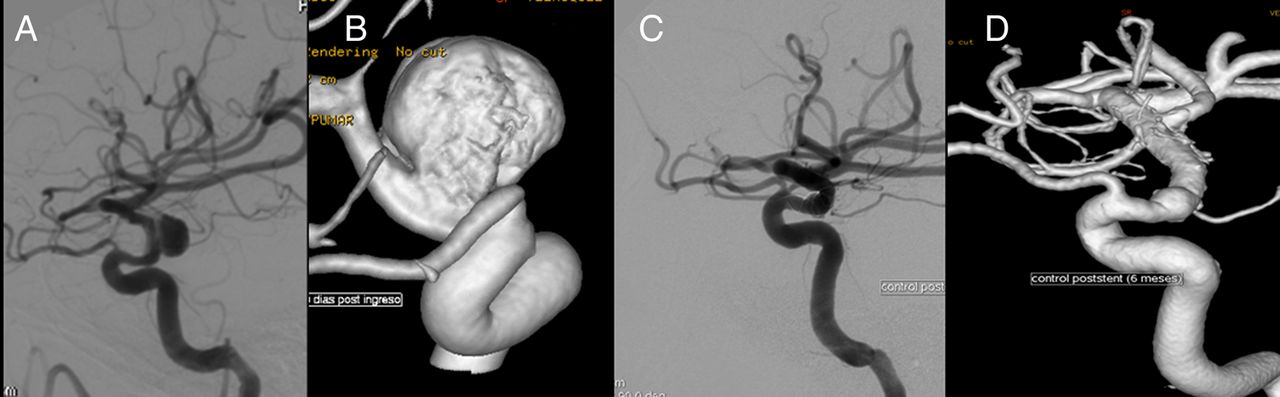
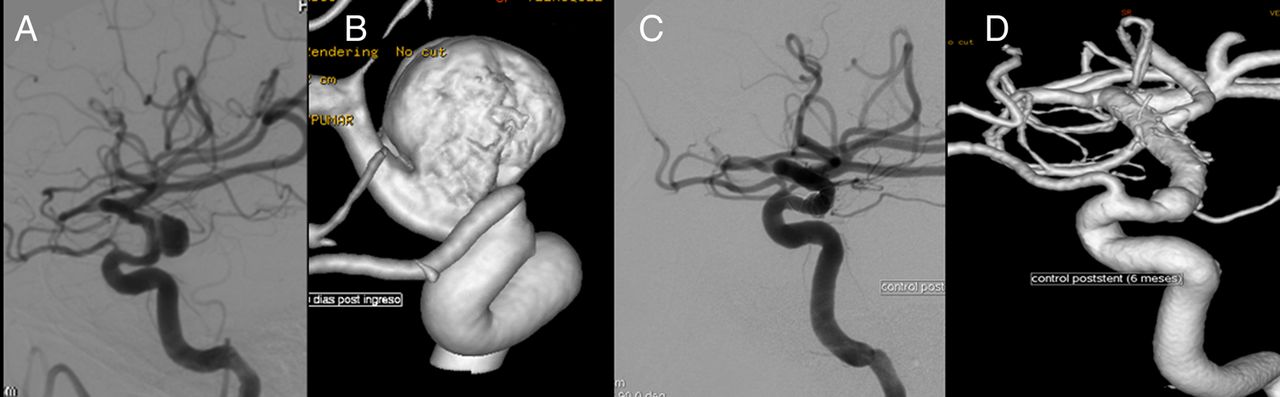
A man aged less than 40 years with a 15 day history of non-specific headache and ptosis in the right eye was admitted to our hospital. Neurological examination revealed ptosis, enlarged pupil, and abducens palsy in the right eye. Digital subtraction angiography findings revealed an irregular right carotid–ophthalmic artery aneurysm (figure 4A, B). The patient underwent reconstructive endovascular repair of the fusiform aneurysm by stent placement (4.5 mm/25 mm Leo Plus stent) across the aneurysm neck without complications. The 12-month follow-up angiogram showed anatomic reconstruction of the parent artery and aneurysm occlusion (figure 4C, D).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lateral angiogram of the right internal carotid (A) and three-dimensional rotational (B) angiogram showing an irregular carotid–ophthalmic artery aneurysm. Subtracted lateral angiogram (C) and three-dimensional rotational (D) projections from follow-up angiogram at 12 months showing anatomic reconstruction of the artery and aneurysm occlusion.
Discussion
Fusiform aneurysms are most frequently associated with compressive or ischemic symptoms, and intracranial hemorrhage is a less common clinical presentation.7 Similar to saccular aneurysms, successful treatment of fusiform aneurysms and their sequelae depends largely on the continued development of innovative therapeutic procedures which pose a challenge for both the neurointerventionalist and neurosurgeon. When deconstructive treatment is possible, various surgical and endovascular methods have been used to treat these aneurysms—that is, proximal occlusion of the parent artery, internal coil obliteration, or trapping of the fusiform segment. However, when deconstructive treatment is not recommended, the management of fusiform aneurysms is more complex. In these cases, relatively new therapies, such as the use of intracranial stents, seem to be promising.
Previous studies by Turjman et al8 and Szikora et al9 have demonstrated the feasibility of combining stents and coils for the EVT of experimental saccular aneurysms.
Imbesi and Kerber10 demonstrated in vitro the technical feasibility of treating experimental fusiform aneurysms with side branches or ‘perforators’ using a combination of endovascular stent implants in the parent artery and coil placement within the aneurysm sac, without obstructing the origin of side branches.
Initially described by Higashida et al11 and later by other groups,4 ,12 ,13 stent assisted coil occlusion of fusiform aneurysms has afforded patients a minimally invasive alternative to cerebral circulation vascular surgery.
The clinical experience in this setting has involved treating intracranial fusiform aneurysms with high porosity stents and then placing coils through the pores of the stent into the most dilated (pseudoaneurysmal) portion of the lesion. Fiorella et al14 found that this technique is safe and effective for the management of circumferential aneurysms that are not amenable to deconstructive embolization. However, the combined approach of stenting plus coiling is not always feasible or safe.
The use of stents in fusiform aneurysms has been shown to lead to aneurysm thrombosis while maintaining the integrity of the parent vessel lumen and that of ‘jailed’ brainstem perforating vessels in the stent treated portion of the vessel.14–17 Flow diversion arising from stent placement in the vessel lumen across the aneurysm may have major hemodynamic effects by redirecting much of the flow away from the lesion and back into the arterial lumen. This process diverts flow from the aneurysm and promotes thrombosis of the saccular or pseudoaneurysmal portion of the vessel. Therefore, intracranial stenting alone may be an alternative therapeutic option in such cases. Ever since Benndorf et al15 reported a case of total spontaneous occlusion of an intracranial aneurysm by overlapping stent placement (AVE S670; Medtronic), and Lylyk et al16 reported the first cases of spontaneous intracranial aneurysm thrombosis following Neuroform (Boston Scientific/Target) stent placement alone, an increasing number of cases of stent only therapy, including various types of intracranial stents (Neuroform 2, Neuroform 2 Treo, Leo Plus), have been reported, showing the feasibility and good clinical and anatomical outcome of this approach.5 ,17–19 In our study, the results with this technique confirm these findings.
Treatment of fusiform aneurysms is the most challenging. The difficulties result from the fact that despite the small dome to neck ratio, the perforator arteries, posterior cerebral arteries, and sometimes the superior cerebral arteries, may originate directly from the aneurysm base. Although in vivo research data with high porosity stents do not show occlusion of jailed smaller vessels, the potential risk of a stroke associated with perforating arteries being covered by stent struts should be considered. The introduction of newly designed stents with low porosity such as Pipeline (Covidien/ev3 Inc, Irvine, California, USA) and Silk (Balt) may help to overcome the limitations of a high porosity stent and play a pivotal role in the treatment of fusiform aneurysms. However, the low porosity of flow diverters theoretically increases their likelihood of occluding covered side branch arteries. The current study did not evaluate the use of flow diverting devices as a method of reconstructive EVT. This new technology appears promising, given its theoretical advantage in providing more physiologic and durable treatment of fusiform aneurysms. While initial studies are promising, complications are increasingly reported, and the long term safety and clinical efficacy of such devices are unknown.20–22
In our series, nine patients with implanted stents in the perforator-rich vertebrobasilar system showed no symptomatic perforator occlusion. In some cases, we observed angiographically asymptomatic slowing and flow reduction of small arteries partially covered by stent struts. These correspond with in vivo research data with high porosity stents and the hypothesis that if the pressure gradient across the perforators is maintained and the perforator is covered less than 50% by stent struts, the arteries will remain patent and will remodel around the struts.3 ,7 ,23
In our series, the LEO Plus stent with high porosity was used, although it was not specifically designed to alter intra-aneurysmal hemodynamics. However, the presence of the stent across the aneurysm may have modified the geometry of the parent artery/aneurysm and/or blood flow into the aneurysm favorably enough to induce thrombus formation. The relationship between stent geometric and structural parameters and the morphological characteristics of aneurysms undergoing treatment have yet to be elucidated.
Stent placement across a fusiform aneurysm must be performed with a higher degree of vigilance and accuracy than for saccular aneurysms as stent anchorage relies on a smaller surface area for contact with the parent artery at either end of the aneurysm. As the neck of a saccular aneurysm originates from a segment but not from the entire circumference of a parent artery, secure stent placement is achievable more often for a saccular aneurysm than for a fusiform aneurysm. If an expanded stent spanning a fusiform aneurysm is poorly anchored at either end of the aneurysm, then it may dislodge from the parent artery and migrate and embolize more distally or fall into the aneurysm sac, causing obstruction of the parent artery. These complications may occur especially during attempted manipulation of the tip of a microcatheter through the stent mesh and into the aneurysm sac. Therefore, care is necessary in choosing the correct length and diameter of a stent for any given fusiform aneurysm and in correct positioning of the stent across the aneurysm before deployment.
Conclusion
This series has shown that stent only therapy may prove useful for the future treatment of intracranial fusiform aneurysms in which parent artery occlusion or stenting–coiling is not feasible.
There are some limitations to consider when interpreting the results of the current study. First, the sample size was not sufficient to warrant statistical exploration of predictors of clinical response by regression analysis. Second, the use of flow diverting devices such as the EVT reconstructive methods was not evaluated. This innovative technology is promising given its advantage in providing more physiologic and durable treatment of fusiform intracranial aneurysms compared with existing reconstructive methods. Although initial studies are promising, the long term safety and clinical efficacy of such devices are unknown.
Footnotes
-
Contributors All authors contributed equally to this work. JMP, MB, FV-H and JAC-M followed the patients, jointly conceived the study, and prepared the manuscript. MA and AM wrote the main paper. SA and MR-Y analyzed and described the neuroimaging, and discussed the results. All authors made a substantial contribution to the conception and design of the paper, acquisition of the data, and analysis and interpretation of the data. All authors discussed the results and implications, and commented on the manuscript at all stages. All authors discussed and approved the final version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study was approved by the ethics committee of Hospital Clínico Universitario de Santiago de Compostela.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/