Article Text

Abstract
Background The ‘balloon-then-stent’ method involves stent placement after completion of a balloon-assisted embolization. The drawback to this technique is that the coil mass achieved during balloon remodeling must be crossed prior to stent deployment. This additional maneuver introduces the potential risk of coil disruption. We describe the first report of a novel technique employing the ‘balloon-then-stent’ method.
Methods A 51-year-old patient with an unruptured right middle cerebral artery bifurcation aneurysm was treated with balloon remodeling employing a 4×10 mm Scepter C balloon catheter. Following coil embolization, a low-profile visualized intraluminal stent (LVIS) Jr 2.5 mm×16 mm was delivered via the coaxial balloon catheter and deployed across the aneurysm neck.
Results Follow-up angiograms demonstrated that the coil mass was well-seated within the aneurysm sac and the parent vessel was widely patent with satisfactory vessel wall apposition by the stent.
Conclusions We describe a technique for balloon remodeling followed by stenting for aneurysm coil embolization that incorporates the use of a coaxial dual-lumen balloon catheter system through which a novel self-expanding stent can be deployed. In the case described, we found this technique to be safe and feasible, reducing both the number of steps involved in this technique and the opportunities for mechanical coil-related complications.
- Stent
- Catheter
Statistics from Altmetric.com
Introduction
Since the emergence of endovascular coil embolization for the treatment of aneurysms,1 rapid advances in the field have secured its place along with microsurgical clipping as one of the two available methods of securing aneurysms. Two advances that have revolutionized the approach to the treatment of wide-necked aneurysms are the introduction of balloon remodeling and stent-assisted coil embolization. Balloon remodeling, first described by Moret et al,2 involves the temporary inflation of a balloon across the neck of an aneurysm allowing for coil deployment into aneurysms with unfavorable neck to dome ratios.3–10 The technique of stent-assisted coiling has also been widely adopted11–26 as a promising adjunct with potential mechanical, hemodynamic and biologic properties, imparting an advantage over coil embolization alone.27 Stent deployment provides mechanical support to prevent coil prolapse and compaction, may serve as a conduit to divert flow and provides a scaffold for endothelial growth and vessel healing.27–29 These two techniques may be used in combination to capitalize on the benefits that each affords.30 This ‘balloon-then-stent’ method involves stent placement after completion of a balloon-assisted coil embolization. The drawback to this sequential technique is that a 0.021 inch or 0.027 inch microcatheter system is required, and the coil mass achieved during balloon remodeling must be crossed prior to stent deployment. This additional maneuver introduces the potential risk of coil disruption, especially when there is coil loop prolapse or herniation into the parent vessel which may lead to thromboembolic complications. In addition, this step may add fluoroscopy and procedure time, in particular when access to the lesion is challenging.
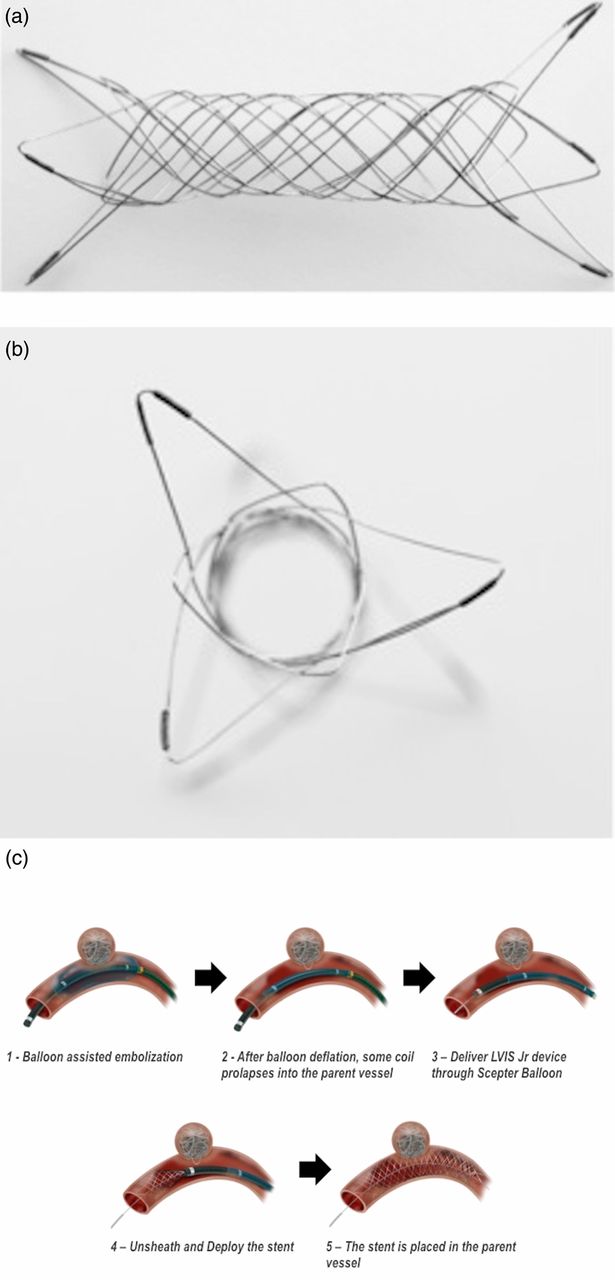
We describe the first report of a novel technique for the ‘balloon-then-stent’ method which incorporates the use of two novel devices. The Scepter C (MicroVention, Tustin, California, USA) is a new temporary occlusion balloon system that has a dual coaxial lumen catheter attached to a low inflation pressure compliant balloon. The design accommodates a steerable 0.014 inch guidewire. The LVIS (low-profile visualized intraluminal stent) (MicroVention) is a novel neurovascular self-expanding retrievable stent system which is composed of a single round wire braided nitinol and double helix tantalum strands in addition to radiopaque tantalum proximal and distal markers to assist full length visualization (figure 1). It is a compliant closed-cell system which is retrievable up to 80% deployment and provides 15–18% surface area coverage. In the USA the LVIS is currently available only in study protocols and is 0.021 inch microcatheter-compatible; however, an LVIS Jr stent has recently become available, also under study protocols, which is 0.017 inch microcatheter-compatible, allowing it to be delivered by the Scepter C balloon catheter system (‘monoaccess’). The LVIS Jr stent provides 13–15% surface area coverage.

(A, B) Photographs of the low-profile visualized intraluminal stent (LVIS) Jr. (C) Schematic step-by-step illustration of the technique for ‘balloon-then-stenting’ of intracranial aneurysms. Courtesy of MicroVention (Tustin, California, USA).
Case illustration
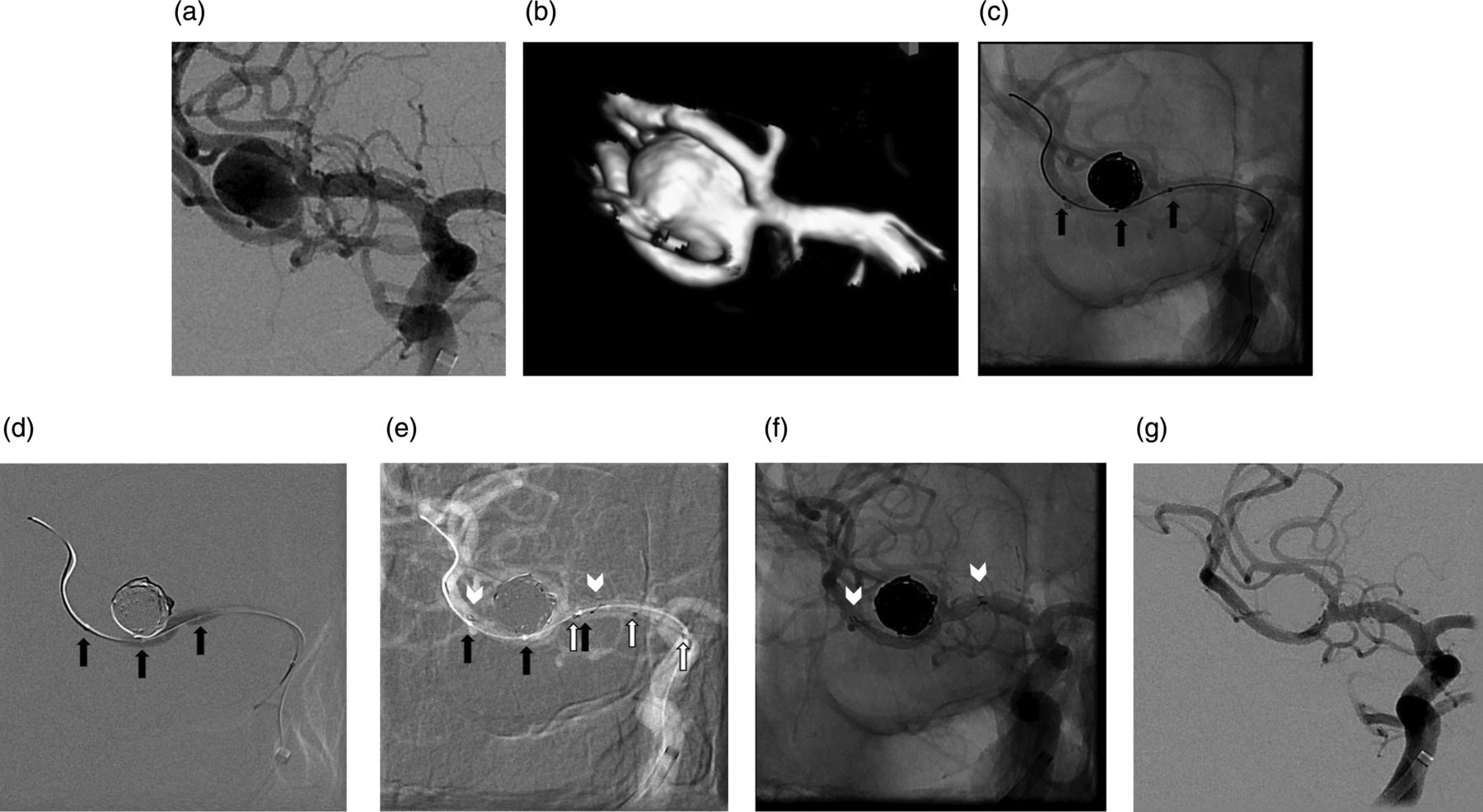
A 51-year-old patient with a significant smoking history was found to have an unruptured right middle cerebral artery bifurcation aneurysm on MRI investigation for bilateral hand tremors and headaches. Cerebral angiography demonstrated an aneurysm arising from the right middle cerebral artery bifurcation projecting laterally and anteriorly, measuring 8.3 mm in height, 7.3 mm in width at the dome with a 5.5 mm broad neck (figure 2). The aneurysm neck incorporated the origin of the inferior division M2 branch of the middle cerebral artery with more than 270° involvement. The patient was administered and maintained on aspirin and clopidogrel prior to the treatment procedure.
{kind=link}
{kind=link}
(A) Right middle cerebral artery bifurcation aneurysm that is broad-necked with incorporation of the inferior division branch. (B) Reconstruction from a three-dimensional rotational angiogram showing incorporation of the inferior middle cerebral artery division branch into the aneurysm neck with more than 270° involvement of the parent vessel. (C) Native view showing a coil mass within the aneurysm with a deflated Scepter C balloon spanning the aneurysm neck across the bifurcation (black arrows outline the tip of the balloon catheter and the proximal and distal balloon markers). (D) Negative roadmap control showing the inflated Scepter C balloon spanning the aneurysm neck across the bifurcation and a growing compact coil mass (black arrows outline the tip of the balloon catheter and the proximal and distal balloon markers). (E) Roadmap control image following LVIS Jr stent deployment by unsheathing it out of the Scepter C balloon catheter. The confines of the Scepter C balloon catheter before (black arrows) and after (white arrows) unsheathing the stent. The LVIS Jr stent confines are also visible (white arrowheads). (F) Post-treatment native view in the working projection showing a compact coil mass within the aneurysm and the confines of the LVIS Jr stent. (G) Subtracted view in the working projection following balloon remodeling and stenting of the aneurysm.
The patient was brought to the neurointerventional suite and placed supine on the angiography table under general endotracheal anesthesia. Using an 18G Cook needle, a 6F Pinnacle sheath was placed into the right common femoral artery. Intravenous heparin 5000 units and intermittent boluses were administered to maintain an activated clotting time 2–2.5 times the patient's baseline level. A 6F Neuron 070 guide catheter (Penumbra, Alameda, California, USA) with a 5F Berenstein diagnostic insert (Penumbra) was advanced into the aortic arch over a 0.038 inch Terumo glidewire (MicroVention) to select the distal petrous segment of the right internal carotid artery. Verapamil 8 mg was injected intra-arterially. Under roadmap guidance, a 4×10 mm Scepter C balloon catheter was advanced over a 0.014 inch Transcend EX platinum guidewire (Boston Scientific, Natick, Massachusetts, USA) into the inferior division branch and centered across the aneurysm neck. An SL-10 microcatheter (Boston Scientific) was advanced over a 0.014 inch Transcend EX platinum guidewire into the middle cerebral artery aneurysm. With intermittent balloon inflations lasting less than 5 min, the following Stryker coils (Boston Scientific) were introduced into the aneurysm and deployed: 9 mm×30 cm 360 soft, 8 mm×30 cm 360 soft, 7 mm×20 cm 360 soft, 7 mm×20 cm 360 soft, 6 mm×20 cm 360 soft, 3 mm×8 cm 360 ultrasoft and 2 mm×6 cm 360 ultrasoft. The microcatheter was removed. With the Scepter C balloon catheter kept in place, an LVIS Jr 2.5 mm×16 mm stent was introduced, centered across the aneurysm neck with the distal markers in the proximal M2 segment and the proximal markers in the mid M1 segment and the balloon catheter was withdrawn to unsheath and deploy the stent across the aneurysm neck and middle cerebral artery bifurcation.
Final follow-up control angiograms were performed in the anteroposterior, lateral and working projections which demonstrated the coil mass to be well-seated within the aneurysm sac and the parent vessel to be widely patent with satisfactory vessel wall apposition by the stent.
Discussion
The ‘balloon-then-stent’ strategy is employed to reinforce balloon-assisted coil embolization. The benefits of balloon remodeling, including high occlusion rates and increased packing density, are supplemented with a scaffold for endothelial healing and flow diversion properties that a stent provides, rendering this combination approach highly effective in the treatment of cerebral aneurysms.24 Balloon remodeling involves the temporary inflation of a balloon across the neck of an aneurysm. As coils are inserted, a stable three-dimensional coil structure ultimately forms, thereby holding the coil mass within the aneurysm. An advantage of coil introduction with adjunctive balloon use is that the microcatheter is stabilized, preventing premature kickback of the microcatheter as well as coil herniation. Once balloon-assisted embolization is complete, the balloon catheter is withdrawn and a stent delivery catheter must be navigated past the aneurysm in preparation for deployment of the stent across the neck. These added procedural steps—particularly the movement of a microwire and catheter back and forth across a broad aneurysm neck packed with coils—introduces the risk of mechanical complications such as inadvertently dragging coils into the parent vessel. It also adds to the procedure time and radiation dose.
We describe a ‘monoaccess’ technique for the ‘balloon-then-stent’ procedure which incorporates the use of a coaxial dual-lumen balloon catheter system (Scepter C) through which a novel self-expanding stent (LVIS Jr) can be deployed. In the case described we found this technique to be safe and feasible, reducing both the number of steps involved in the technique and the opportunities for mechanical coil-related complications. We anticipate the adoption of this technique to be a valuable tool in the armamentarium of the neurointerventionalist.
Footnotes
-
Contributors All authors contributed to the article and to its revision and gave their final approval for submission of the article to this journal.
-
Funding None.
-
Competing interests The following physicians have interest in speakers bureau or consultant: AT; Stryker, Codman, Microvention, Penumbra, and Pulsar Vascular. RT; Stryker, Codman, Penumbra, Microvention, and EV3. IC; EV3.
-
Ethics approval Ethics approval was obtained from the Medical University of South Carolina IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.