Article Text

Abstract
Background Optical coherence tomography (OCT) is a high-resolution, intra-vascular diagnostic technique widely used for the characterization of vascular pathologies and optimization of stent implantation during percutaneous coronary intervention. OCT was used to investigate the in vivo vascular response to a new phosphorylcholine surface modified flow diverter (sPED).
Methods In an in vivo rabbit aneurysmal model, we used two different types of flow diverters (classic Pipeline – cPED; and sPED) with or without dual antiplatelet therapy (four groups, n=10 per group). OCT cross-sectional area measurements were compared with histology in all animals. Neointimal hyperplasia (NIH) ratio was compared between OCT and histology at five different levels for each stent. The severity of NIH was also compared between the different stents, antiplatelet protocols, and vessel locations.
Results OCT was used to calculate in-stent hyperplasia in 227 different locations corresponding to histology sections. OCT measurement strongly correlated with gold standard histology (r2=0.83; slope=0.988; P<0.0001). sPED had significantly less in-stent NIH than non-treated flow diverters (mean percent of lumen reduction 5.7% for sPED versus 8.9% for cPED; P<0.0001). The NIH ratio was slightly higher with dual antiplatelet therapy (DAPT) (NIH ratio=7.9% with DAPT versus 6.8% without DAPT; P<0.05). Complete and near complete occlusion rates of the aneurysms were not different with the cPED or sPED.
Conclusion OCT is a promising technique for immediate and long-term evaluation of flow diverter stent treatments. In an animal model, phosphorylcholine surface modified flow diverters induces less NIH after stent implant without reducing aneurysm occlusion rates.
- Intracranial aneurysm
- flow diverter
- optical coherence tomography
Statistics from Altmetric.com
Introduction
Neointimal hyperplasia (NIH) is frequently depicted during the imaging follow-up of flow diverter treatment,1 and may lead to delayed ischemic strokes.2 Phosphorylcholine surface modified flow diverters (Pipeline Flex with Shield Technology, sPED) were recently developed and demonstrated reduced thrombogenicity both in vitro3 and vivo.4 We hypothesized that the improved thrombogenicity profile of the sPED5 may be associated with reduced NIH.
Optical coherence tomography (OCT) is an intravascular technique using near-infrared light reflection to generate cross-sectional, high-resolution images. It is widely used during percutaneous coronary intervention to explore atherosclerotic plaques and to optimize stent placement.6 7 Up to now, OCT has been rarely used in the neurointerventional field mostly because the design of the OCT catheter is not optimized for intracranial navigation. However, it has been recently demonstrated to be a valuable diagnostic assay for the characterization and development of novel neurointerventional devices.4 8 9 OCT has been demonstrated to strongly correlate with histology to evaluate neointimal coverage after coronary stent implantation.10 11 Flow diverters and coronary stents present very different designs. Indeed, the struts of flow diverters are thinner and the porosity is significantly reduced. We also evaluated the ability of OCT to characterize the vascular response to flow diverters compared with gold-standard histology.
Methods
Aneurysm creation and study design
After Institutional Animal Care and Use Committee approval, elastase-induced aneurysms were created in 40 New Zealand white rabbits at the origin of the right common carotid artery as previously described.12 A minimum of 3 weeks after creation, the aneurysms were screened with digital subtraction angiography (DSA)13 and randomized to one of the following treatment groups: classic Pipeline embolization device (cPED) with animal on dual antiplatelet therapy (DAPT); sPED with DAPT; cPED without DAPT; and sPED without DAPT. Animals assigned to DAPT received oral aspirin (10 mg/kg) and clopidogrel (10 mg/kg) beginning 5 days prior to flow diverter (FD) implant and continued for the duration of the study.
Flow diverter implant and OCT imaging
All procedures were performed under general anesthesia. First, the animals were pre-anesthetized by a subcuticular injection of atropine (0.01 mg/kg), followed by an intramuscular injection of a mixture of ketamine (35 mg/kg) and xylazine (5 mg/kg) for anesthesia induction. The animals were intubated and mechanical ventilation was maintained with 1%–3% isoflurane.
A 6Fr introducer sheath was inserted after surgical exposure of the right common femoral artery. A Navien 072 catheter was used to navigate the FD to the right subclavian artery. Both devices were sized based on the diameter of the brachiocephalic trunk proximal to the aneurysm and ranged from 3.75 to 4.5 mm. All devices were 16 mm in length. The FD was deployed under fluoroscopic guidance and implanted such that complete coverage of the aneurysm neck was achieved. Angioplasty was performed on all devices (HyperGlide 4 mm x 10 mm) to optimize apposition.
Thirty days after device implant, the animals were re-anesthetized and DSA was performed to assess the stent permeability and the aneurysm occlusion on a previously described 5-point scale.14 Then OCT imaging (Dragonfly Catheter, St Jude Medical, Westford, MA, USA) were acquired with a 10 mm/s pull-back speed through 54 mm length, generating 540 frames/pull-back. For sufficient blood clearance, iodinated contrast (Omnipaque 240, GE Healthcare, Malborough, MA, USA) was administered by a power injector at a flow rate of 4 mL/s for 4 s.
Tissue harvesting and histology
Intimal hyperplastic response in this animal model has been reported to reach a peak at 30 days.15 Therefore, following the 30-day imaging procedure, euthanasia was performed by an overdose of sodium pentobarbital (150 mg/kg). Transcardiac perfusion fixation was performed using heparinized saline (5000 U/L) followed by 4% paraformaldehyde under physiological pressure. The subclavian and innominate arteries were explanted then embedded in epoxy resin. The embedded vessels were then sectioned with a Buehler Diamond saw, lightly sanded, polished, and stained (1% toluidine blue). Seven histological sections were performed; one prior to the aneurysm; three at the neck level; one distal to the aneurysm; one at the origin of the vertebral artery; and a last one at the distal part of the stent (figure 1).
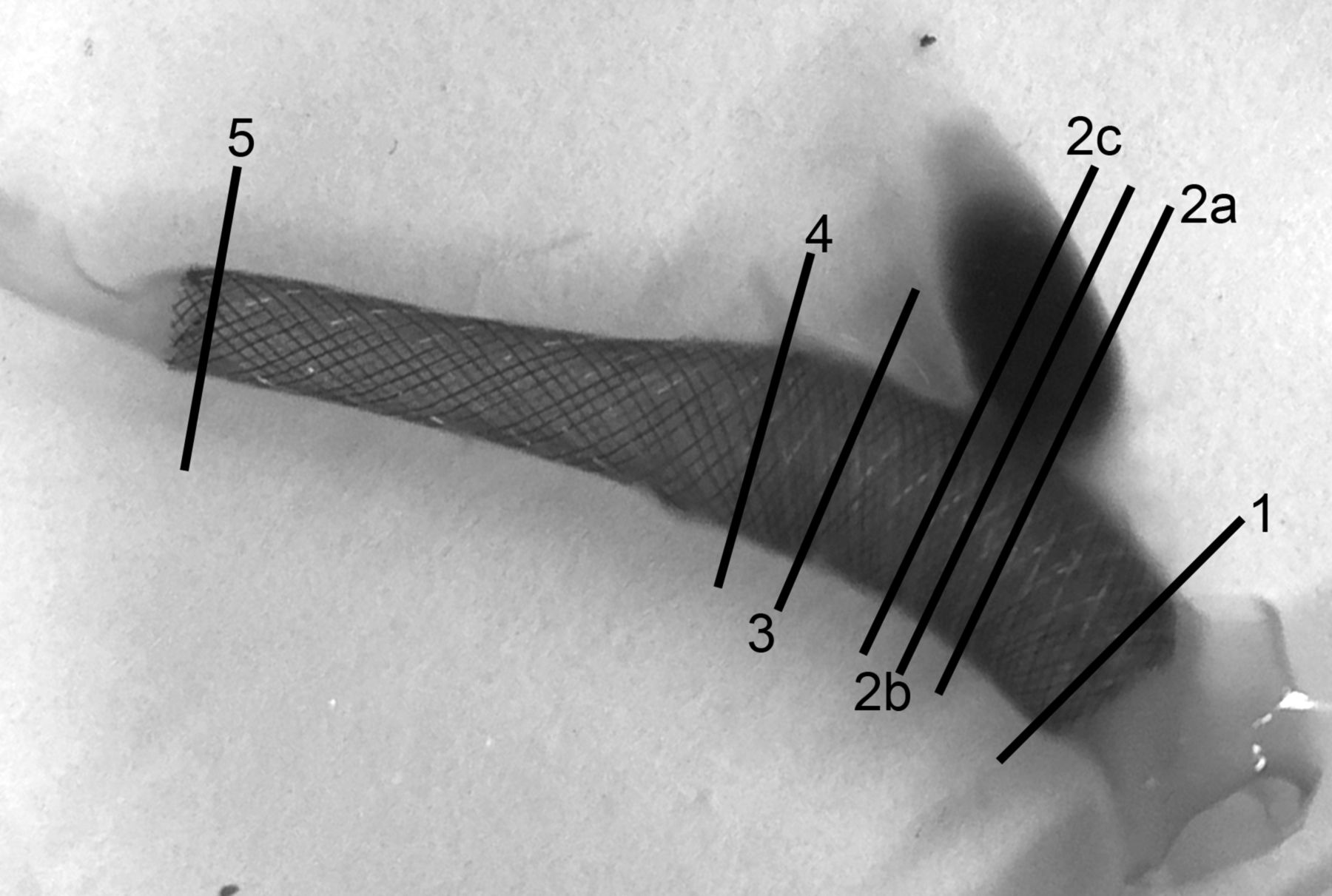
Photograph of the harvested implanted artery. Each line represents a section taken for histology. 1=proximal stent, 2a, b, and c=at the level of the aneurysm neck, 3=distal to the aneurysm, 4=at the origin of the vertebral artery, 5=at the distal part of the stent.
Images analysis
In each case, all 540 OCT images acquired were analyzed and seven cross-sections co-registered from the histology sections were selected (figure 2). In a blinded fashion, all histological and OCT images were used to measure the lumen area, the stent area (defined by the area limited by the struts of the stent), and the neointimal area (defined by stent area/lumen area), while the percent of lumen reduction related with NIH was defined as the NIH ratio (lumen area/stent area).
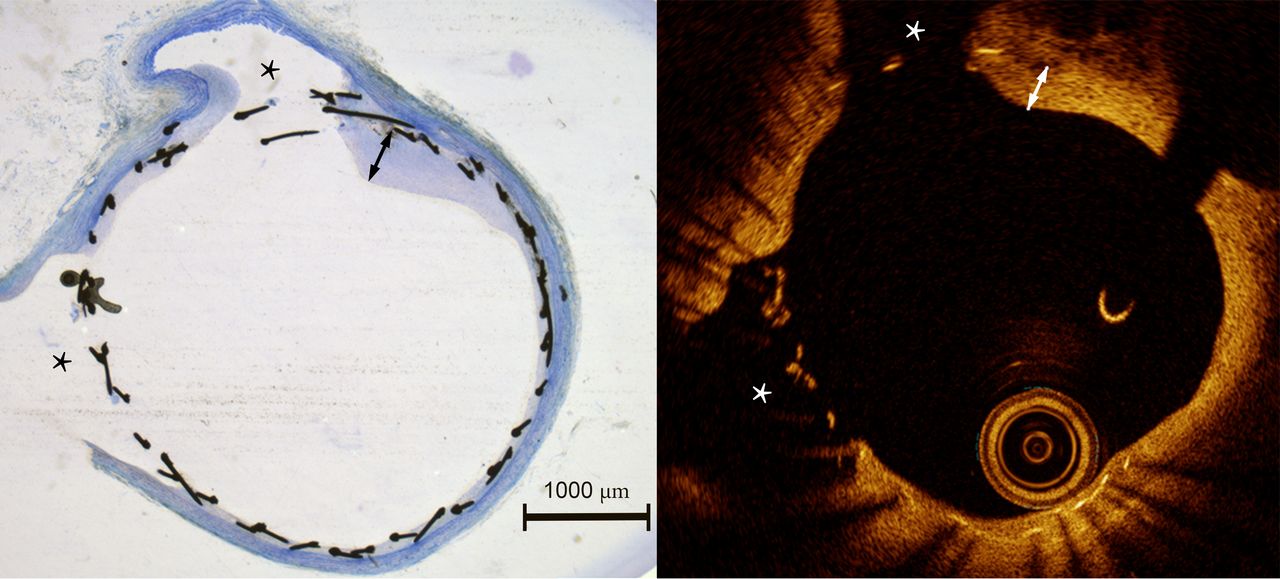
Histological (left), and OCT (right) cross-sections at the level of vertebral and internal thoracic arteries (*) demonstrating the correlation between the two techniques. Neointimal hyperplasia presents here an asymmetric pattern with a localized maximum thickness (line with arrows).
Over a theoretical number of 280 sections, 227 were analyzed. Some were missing either because of insufficient quality or because it was not possible to obtain three histological sections through the neck of the aneurysm or the distal landing zone did not extend beyond the vertebral artery.
Statistical methods
Statistical analysis was performed using R version 3.4.1 (R Foundation for Statistical Computing, Vienna, Austria). OCT and histology images were compared using linear regression and the Bland–Altman test. The NIH ratios were compared between the different types of stent, antiplatelet therapy protocol, and locations using two-way repeated measures analysis of variance (ANOVA). A Fisher’s exact test was used to compare the rates of occlusion. A P value of <0.05 was considered statistically significant.
Results
Histological and OCT correlation
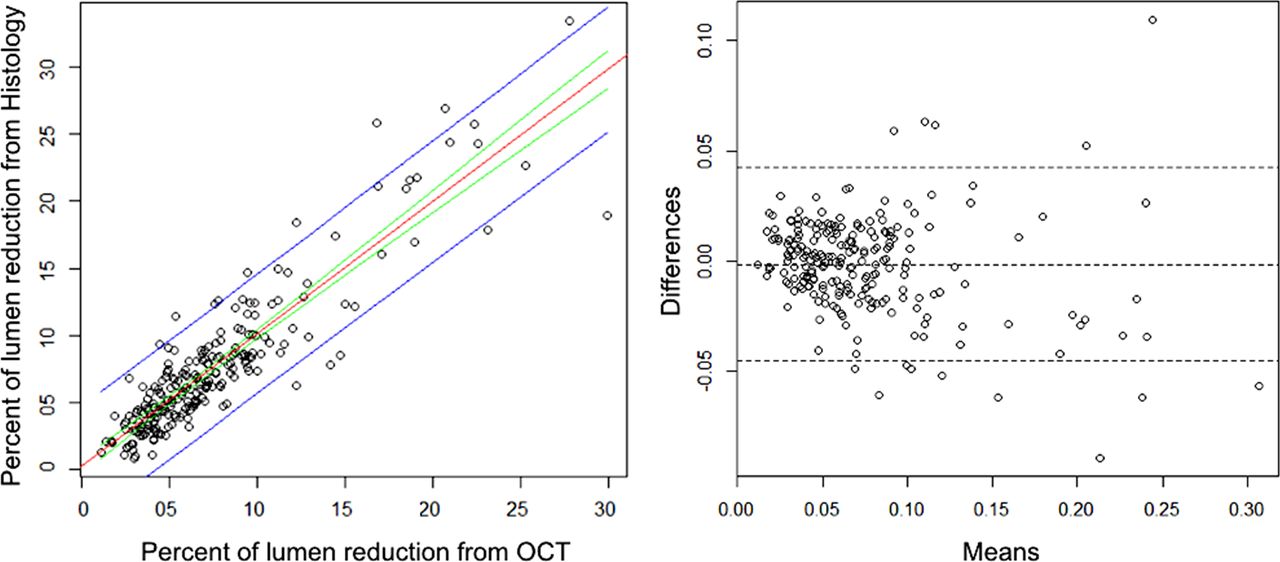
When compared by linear regression, OCT measurement strongly correlated with gold standard histology (r2=0.83; slope=0.988; P<0.0001). The Bland–Altman analysis showed that histology and OCT measurements are equivalent and free of systematic bias when measuring NIH lumen reduction (bias=−0.15%, SD of bias=2.2%, 95% CI –4.5% to 4.2%; (figure 3).

A. Comparison between histological and OCT measurements of the percent of the lumen reduction with linear regression analysis. The red line is the best fit line for the data, with r2=0.83; slope=0.988 (P<0.0001). The green lines indicate 95% CI for that given best fit line. The blue lines indicate 95% confidence of the prediction interval. B. Bland–Altman analysis showing a bias of −0.15% and SD of the bias of 2.2%.
To assess the intra-observer variability of the OCT measurements, we randomly selected 30 datasets and repeated the analysis. The mean absolute difference was 1.0% (CI 95%: −0.37;2.37).
Effect of phosphorylcholine surface modification
Phosphorylcholine surface modified flow diverters presented less in-stent NIH than non-modified flow diverters with an average 56% reduction in NIH ratio on OCT measurements (NIH ratio were 5.7% for sPED versus 8.9% for cPED; P<0.0001).
Effect of DAPT
The severity of NIH was slightly more pronounced with DAPT (mean NIH ratio from OCT measurements were 7.9% for with DAPT versus 6.8% without DAPT; P<0.05).
Effect of location
Location had a significant effect over the NIH. The more distal location (location 5) presented the maximum NIH ratio with an average lumen reduction of 14% and a significant difference with all other section locations (P<0.0001) (table 1).
Effect of section location on NIH as measured on OCT
Also, we found a linear relationship between the ratio of stent oversizing (FDS nominal size over vessel size from OCT measurement) and the NIH ratio (r2=0.46; P<0.0001) (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison between stent oversizing (flow diverter nominal size over vessel diameter from OCT measurements) and the percent of the lumen reduction with linear regression analysis. The red line is the best fit line for the data, with r2=0.46 (P<0.0001). The green lines indicate 95% CI for that given best fit line. The blue lines indicate 95 % confidence of the prediction interval.
Moreover, the sPED had significantly less NIH for all locations, except location 3, as compared with cPED (table 2).
Comparison of NIH ratio per section location
Occlusion rates
Occlusion rates were not different between the different stent types and use of DAPT (table 3).
Aneurysms' characteristics and occlusion rates at 30 days
Discussion
OCT validation
OCT has proven to strongly correlate with histology to evaluate NIH coverage after coronary stent implantation.10 11 However, we sought to validate those results specific to neurointerventional devices since flow diverter design differs substantially from coronary stents.16 Flow diverter struts are much smaller (~30 µm) than laser cut, coronary stents (~100 µm) requiring very high resolution to depict the device relationship with the wall. Flow diverters have a much higher metal density as well, which can induce significant optical artifacts.
In our study, OCT values correlate well with the gold standard histology (r2=0.83; P<0.0001). Recently, in a pig model, Matsuda and colleagues8 described good agreement between OCT and histology for imaging flow diverters. The data presented here are in excellent agreement and our quantitative analysis in a rabbit model further validate the use of OCT to characterize tissue response to flow diverters. Image co-registration between OCT and histological photomicrographs was done manually by visualization of anatomical landmarks. It is possible that this introduced some errors in comparing the measurements. However, from the Bland–Altman analysis, the average absolute difference between the measurements was close to zero, meaning that the NIH ratio value from OCT is reliable. We believe this is an important result, as OCT may play an important role in flow diverters implant optimization as the optical engine and catheter technologies improve.
Phosphorylcholine surface modification effect
The Pipeline embolization device with phosphorylcholine surface modification was recently developed in order to improve the hemocompatibility of this device, and reduced thrombogenicity has been demonstrated both in vitro3 and vivo.4 This surface modification has already demonstrated efficacy in reducing NIH on arterial grafts.5
Although the magnitude of the absolute difference in lumen reduction between the sPED and cPED was small, the average relative reduction of NIH ratio was 56% and statistically significant. Also, despite the relatively frequent presence of NIH following FD treatment, this rarely produces clinically significant sequelae.17 18 Some authors propose extending the indication of FD treatment to aneurysms beyond the circle of Willis.19 In those locations, bifurcation and large side branches are frequently covered by the stent. It has been shown that for bifurcation branches, at 3 months' follow-up, the percentage of ostium surface tissue coverage ranged from 80% to 98%.20 We assume that even a small decrease in the NIH amount at the level of the ostia could reduce the high rate of occlusion and flow modifications of those jailed branches.21
Also, these young and healthy animals generally do not have a pronounced response to the implant. So the reduction of the NIH ratio in the sPED group could be more pronounced in clinical practice.
Recently, Matsuda et al8 studied NIH evolution to flow diverters in a swine model and did not find any difference in the neointimal volume between cPED and sPED. However, in their study with variable anti-platelets, 100% of the cPED and 33% of sPED thrombosed at day 7 and were then reopened using mechanical thrombectomy. Thus, in-stent clotting and subsequent treatment may have modified the normal pathophysiology of NIH after flow diverter implant.
Aneurysmal healing
With flow diverters, the aneurysmal occlusion is obtained by both promotion of flow-diversion-related aneurysm thrombosis and from newly formed endothelial coverage over the device at the level of the neck.22 This second step is fundamental to permanently exclude the aneurysm from the circulation. A stent design that would prevent any neointimal formation would not serve the healing purpose. The goal is to ‘control’ a potential excessive and harmful proliferative response to the device, while allowing effective remodeling of the vessel.
Here in our study, from OCT images in the selected sections going thru the aneurysmal neck, we found that in a very limited number of cases (2.1%; 1/47) a NIH ratio of 1% or less (meaning that the NIH coverage is minimal). Furthermore, we did not find any difference in occlusion rates with 50% of complete or near complete occlusion for cPED and 45% for sPED (P=0.8).
The severity of neo-intimal hyperplasia was slightly more pronounced with DAPT with a 1.1% increased NIH ratio. NIH development is initiated by an endothelial damage during FDS implantation and angioplasty. Platelets adhering to the subendothelial surface participate in the NIH through platelet-derived growth factors inducing a vascular smooth muscle cell proliferation.23
Aspirin has proven to inhibit early platelet thrombus formation.24 While the interference with platelet function reduces intimal hyperplasia in human and primate studies, in rabbit models it has shown to fail to prevent platelets and fibrin deposition after wall injury,25 and also it may increase the NIH ratio.26 27 We selected a 10 mg/kg dose of aspirin based on prior literature;28 however, this dose represents an approximately 10-fold increase over the common dose used in humans. Future studies should evaluate the effect of aspirin dosing on NIH formation in this model. In some animal models, clopidogrel was sometimes found ineffective to prevent NIH,23 highlighting the role of other factors than platelets alone in NIH formation, such as leukocytes.29
From our data, we have showed that there is a linear relationship between the device oversizing and the amount of NIH. As the device radial force is low we suspect that the increased vessel metal coverage due to flow diverter oversizing would be responsible for higher NIH. This parameter should be taken into account when sizing flow diverters in situations where the distal and proximal vessel caliber are significantly different (ie, in case of dysplastic vessels or when the FDS has to be anchored in a smaller branch as the middle cerebral artery to treat siphon aneurysms).
Our model was limited to saccular aneurysms. Although it is true that we did not find any significant difference in aneurysm occlusion rates between the different groups, it would be of interest to repeat these experiments in different models, such as fusiform aneurysms.30 31
Our study has several limitations. To assess the margin of error of repeated OCT measurements, we did not perform multiple pullbacks since the contrast load would have been too great for 3 kg rabbits. In half of the cases we did not use DAPT in order to maximize the potential differences between the device types, but that does not correspond to the standard clinical practice. Moreover, the use of balloon angioplasty of FD is not clinical standard-of-practice and may alter NIH patterns. However, despite these departures from clinical routine to enhance NIH in this model we did not encounter a single stent occlusion and that may reflect some difference between human and rabbit biology. Thus, the effects of the phosphorylcholine surface treatment in flow diverters should be confirmed in human studies.
Conclusion
OCT is a promising technique for the immediate and long-term evaluation of flow diverter treatments. In an animal model, phosphorylcholine surface modified flow diverters (sPED) induces less NIH after stent implant without reducing aneurysm occlusion rates.
References
Footnotes
JC, TT and RMK contributed equally.
Contributors Study design: JC, RMK, ETL, JMW, FC, MM, MJG, and ASP. Data acquisition: JC, TT, RMK, ETL, FC, MM. Literature research: JC, RMK, MM, MJG. Data analysis and interpretation: JC, TT, RMK, PNL, FC, LS, MM, MJG, and ASP. Manuscript preparation: JC and RMK. Revision of manuscript for important intellectual content: FC, MM, MJG, and ASP. Approval of final version of manuscript: all authors.
Funding This work was supported by Medtronic Neurovascular. The content is solely the responsibility of the authors, and does not represent the official views of Medtronic. JC was supported by research grants from the Fulbright Program, the Philippe Foundation, and the French Society of Radiology.
Competing interests FC: Has been a consultant on a fee-per-hour basis for Medtronic, Balt Extrusion, Guerbet (paid lectures), and for Codman Neurovascular (Study core lab). ETL: Has been a consultant on fee-per-hour basis for R92M, Stryker Neurovascular, and The Stroke Project. JMW: Is employed by Medtronic Neurovascular. LS: Has been a consultant on fee-per-hour basis for Medtronic Neurovascular, Microvention, Stryker Neurovascular. MJG: Has been a consultant on a fee-per-hour basis for Codman Neurovascular, InNeuroCo, Medtronic Neurovascular, R92 Medical, Stryker Neurovascular, and the Stroke Project; holds stock in InNeuroCo; and has received research support from the National Institutes of Health (NIH), Anaconda, Codman Neurovascular, Gentuity, InNeuroCo, Microvention, Medtronic Neurovascular, MIVI Neurosciences, Neuravi, Philips Healthcare, InNeuroCo, Rapid Medical, R92M, Stryker Neurovascular, The Stroke Project, and the Wyss Institute. ASP: Has been a consultant on a fee-per-hour basis for Medtronic Neurovascular and Stryker Neurovascular; and has received research grants from Medtronic Neurovascular and Stryker Neurovascular. JC: Has received educational scholarships from Medtronic Neurovascular and Microvention/Terumo.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice Since this paper was first published online, a competing interest has been added for the author JC.
Presented at 14 Annual Meeting of the SNIS, Colorado Springs CO. July 26-28, 2017.