Article Text

Abstract
Background The embolization technique can have significant impact on the success of endovascular embolization.
Objective To evaluate the feasibility, embolization characteristics, and embolization extent with a newly developed extra-small micro-balloon catheter in an in vivo and in an in vitro embolization model in comparison with standard microcatheter embolizations.
Materials and methods Twenty-eight embolization procedures were performed in the porcine rete mirabile (RM) and in an in vitro embolization model, using either an extra-small (distal outer diameter 1.6 F) dual-lumen micro-balloon catheter or a standard microcatheter. Precipitating hydrophobic injectable liquid (PHIL) was used as embolic agent. Procedure times, number of injections, required volume of embolic agent, and embolization extent (percentage of embolized RM in postinterventional X-ray scans or number of filled sections of the in vitro model) were assessed. Histopathological analyses were performed.
Results Total procedure time was significantly shorter (in vivo: 123 s vs 615 s (medians), P=0.001; in vitro: 180 s vs 496 s (medians), P=0.001), number of reflux events was significantly lower (in vivo: 0 vs 9 (medians), P=0.001; in vitro: 0 vs 3 (medians), P=0.001), and embolization extent was significantly higher (in vivo: 96.9% vs 65.6% (medians), P=0.011; in vitro: 26 vs 18 filled sections (medians); P=0.041) for the micro-balloon catheter groups. There was antegrade movement of the PHIL cast after balloon deflation in one in vitro embolization procedure and spontaneous balloon deflation with subsequent reflux in one in vivo embolization procedure.
Conclusion Extra-small dual-lumen micro-balloon catheters can improve endovascular embolization in comparison with standard microcatheter embolization.
- arteriovenous malformation
- balloon
- catheter
- liquid embolic material
- fistula
Statistics from Altmetric.com
Introduction
Endovascular embolization can play an important role in the treatment of arteriovenous malformations (AVMs), dural arteriovenous fistulas (dAVFs), and hypervascular tumors.1–6 The established standard embolization method is to inject an embolic agent slowly through a catheter until the specific embolization endpoint is reached—for example, complete filling of an AVM or stasis in the vasculature of a hypervascular tumor.5 7 At some point during the embolization procedure, reflux of embolic agent back along the catheter may occur.7 8 Reflux bears the risk of closing access before completion of the embolization procedure, catheter entrapment (mainly for liquid embolic agents (LEAs)), and unwanted embolization of non-target arteries, eventually leading to complications and/or to treatment failure.7–9 In the case of reflux, the embolization is usually paused for a certain period of time until hardening of the embolic agent (for LEAs) or until deeper penetration of the embolic agent into the vascularity (mainly for non-LEAs), thus increasing procedure and fluoroscopy time. When using LEAs, the formation of a plug around the catheter tip, consisting of hardened LEA, resulting after several small-volume injections of LEA with a certain amount of intended reflux, is often a prerequisite for effective penetration and complete embolization.7 8 The treatment of cerebral AVMs represents a special challenge since feeding arteries of cerebral AVMs are often small and arteries supplying healthy brain tissue are often in close proximity, increasing the relevance of reflux.1 7
Different approaches for controlling reflux during embolization have been proposed.10–12 One option is to use a catheter with a balloon situated proximal to the catheter tip with two lumina, one for balloon inflation and one for injection of the embolic agent, so-called dual-lumen balloon catheters.8 13 14 For the treatment of complex pathologies with small target vessels, the currently available balloon catheters can be too large for navigation into these vessels and/or the risk of damage to these vessels, caused by balloon inflation, can be too high.8 13–15
The aim of this study was to evaluate the feasibility, embolization characteristics, and embolization extent with a newly developed extra-small micro-balloon catheter (MBC) in an in vivo and in an in vitro embolization model in comparison with standard microcatheter (SMC) embolizations. The rationale of the in vivo studies was to evaluate the embolizations under conditions that are similar to the clinical setting; the rationale of the in vitro studies was an additional evaluation with a high level of standardization.
Materials and methods
In vivo embolization model and animal procedure
The rete mirabile (RM), a fine vascular network, located bilaterally at the cranial base of pigs, which has been used as an endovascular embolization model by a number of investigators, was used as embolization model.16–20 State Animal Care and Ethics Committee approval was obtained. Anesthesia, sacrifice (2 hours after intervention), and histopathological investigation were performed as described previously.20 Sections were processed following routine protocols for hematoxylin and eosin and Elastica van Giesson staining. Histopathological evaluation was performed by AvD, who has 25 years of experience in neuropathology.
In vitro embolization model
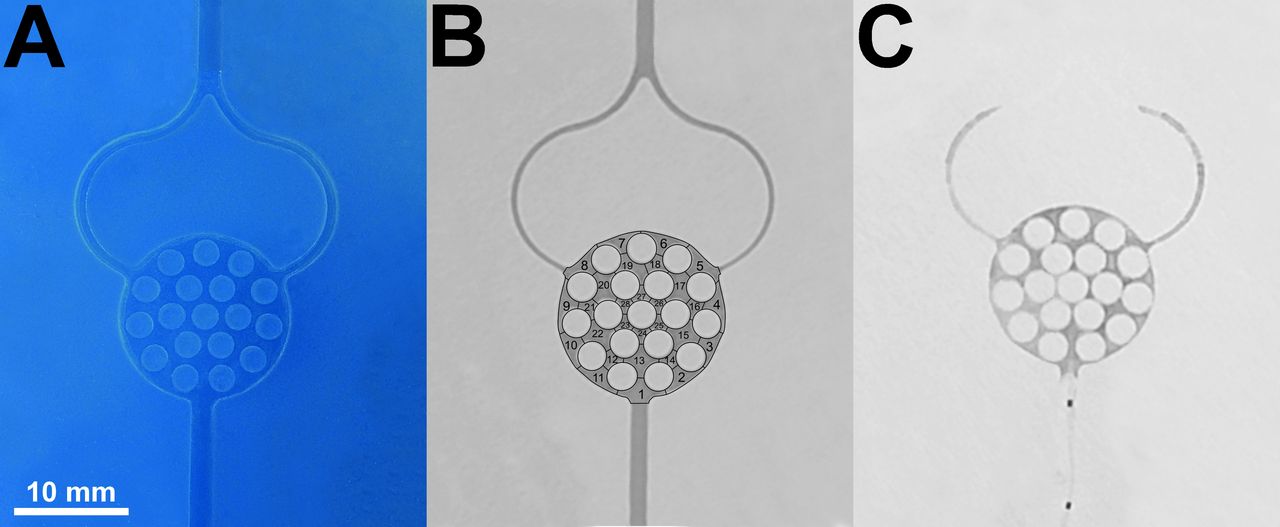
An in vitro endovascular embolization model was used according to the method of Vollherbst et al.21 The model, resembling an AVM, consisted of an afferent tube with a diameter of 2 mm, representing the feeding artery, supplying an artificial nidus: a round, flat, honeycomb-like three-dimensional space (subdivided into 28 honeycomb-like sections) and two efferent tubes each with a diameter of 2 mm, representing two draining veins. The embolization model was integrated into a circuit system with a constant flow of sterile 0.9% (weight/volume) sodium chloride solution at a flow rate of 120 mL/min.
Embolization technique
The microcatheter (MBC or SMC) was inserted coaxially through a guiding catheter. Subsequently, the catheter tip was positioned in the origin of the RM, defined as the first branching of the ascending pharyngeal artery (APA; in vivo) or in the origin of the artificial nidus (in vitro). After flushing the catheter with 1 mL of dimethyl sulfoxide (DMSO), embolization was performed by manual and pulsatile injection under fluoroscopy guidance (Artis zee; Siemens, Forchheim, Germany) using 1 mL DMSO-compatible syringes.
Precipitating hydrophobic injectable liquid (PHIL; MicroVention, Tustin, USA) was used as LEA. PHIL25, being the least viscous version, was used in order to achieve deep penetration and consequently maximal filling of the embolization models.
For each injection, a certain amount of reflux and distal embolization was tolerated, defined as 5 mm distance of the APA (in vivo) or of the feeding artery or the draining veins (in vitro). In the case of embolization of the distal or medial portion of the RM with imminent embolization of the brain or of the contralateral RM (in vivo) or in the case of reflux exceeding the limit of 5 mm (in vitro), the injection was stopped and paused for 60 s. In the case of complete embolization of the APA, embolization of the contralateral RM or the brain (in vivo) and in the case of reflux or draining vein embolization exceeding a limit of 15 mm (in vitro), the procedure was terminated prematurely.
All interventions were performed in the same way by two interventionalists (MAM and DFV) with 12 and 5 years of experience in endovascular therapies, respectively.
Balloon-assisted embolization
A newly developed DMSO-compatible dual-lumen MBC (MicroVention) was used. The design of the balloon and technical specifications are illustrated and described in figure 1. The MBC was used with a Traxcess 7 mini guidewire (MicroVention; outer diameter at distal tip: 0.007 in). To prevent damage to the balloon, the guidewire should not be advanced more than 5–6 cm distal to the tip of the MBC. Before insertion, the balloon-related catheter was flushed and filled with pure iodinated contrast agent, and subsequently, deflated in saline. The balloon tip does not need to be steamed owing to a self-sealing technology (steaming will damage the balloon). After confirmation of the adequate embolization position, the micro-balloon was slowly inflated with 0.02 mL pure iodinated contrast agent using a 0.25 mL syringe. According to the manufacturer’s information, the relation of inflation volume to balloon diameter is as follows: 0.01 mL/1.4 mm, 0.02 mL/2.0 mm (nominal inflation volume and diameter), 0.03 mL/2.3 mm and 0.04 mL (maximum injection volume)/2.6 mm. One minute after embolization, the balloon was deflated and the catheter was removed under fluoroscopy. After removal, the distal parts of the catheters were inspected and photographed to observe adherent LEA.

Specifications, illustration, and photograph of the micro-balloon catheter. A: working length, 165 cm; B: balloon length, 10 mm; C: distal tip, 2.5 mm; D: radiopaque marker bands; E: access to lumen for balloon inflation and deflation; F: access to working lumen (dead space: 0.44 mL). The catheter has an outer diameter of 2.8 F for the proximal shaft and 1.6 F for the distal tip, and an inner diameter of 0.0155 inch for the proximal and 0.0095 inch for the distal inner lumen. The hydrophilic coated balloon has a nominal diameter of 2.0 mm when inflated with a volume of 0.02 mL.
Standard embolization technique
Standard embolization was performed using a standard DMSO-compatible 1.3 F microcatheter (Headway Duo; MicroVention).
Study groups
In total, 28 embolization procedures were performed, 14 in the in vivo and 14 in the in vitro embolization model. Four study groups with seven embolization procedures per group were defined: group A (MBC, in vivo), group B (SMC, in vivo), group C (MBC, in vitro), and group D (SMC, in vitro). The results of four embolization procedures from group B (control group) were published previously with a different focus.20
Study goals
The aim of each embolization procedure was complete filling of the embolization model (the ipsilateral RM for the in vivo model). Total procedure time, median time per single injection, number of injections, and required volume of LEA for each procedure were measured. For the in vivo model, the number of events of reflux, embolization of the contralateral RM and of the distal portion of the RM was assessed. For the in vitro model, the number of events of reflux and draining vein embolization was assessed. For determination of the embolization extent, in the in vivo model the area of the respective side of the RM in the preinterventional posteroanterior angiogram was determined and related to the embolized portion of the RM in the X-ray scan.17 20 In the in vitro model, the embolization extent was graded according to the number of filled honeycomb-like sections of the artificial nidus.21
Statistics
Prism (version 7.02; GraphPad, La Jolla, USA) was used for data analysis. Quantitative data are presented as medians (lower quartile; upper quartile). To evaluate statistical differences between the study groups the Mann-Whitney test was performed with a P value of 0.05 as the threshold for statistical significance.
Results
All embolization procedures were performed as planned. In the in vivo model, the MBC could be easily navigated into the APA in all cases. In one in vivo embolization (group A), during embolization, there was minimal spontaneous deflation of the micro-balloon, leading to reflux of a small amount of LEA proximal to the balloon. After re-inflation, the embolization procedure could be continued without further complications. The remaining micro-balloons remained intact throughout all embolization procedures with no evidence of spontaneous deflation. In one in vitro embolization (group C), after deflation of the micro-balloon, there was antegrade movement of the PHIL cast by approximately 5 mm into the venous portion of the model, resulting in secondary deterioration of the embolization extent. No further complications, such as catheter occlusion, catheter entrapment, movement of the micro-balloon during embolization, or damage to the feeding artery, were observed. Inspection of the microcatheters showed no LEA on balloon surfaces or catheter tips.
Representative X-ray scans after embolization and an example of an analysis of the embolization extent are shown in figure 2 and figure 3. Embolization characteristics and embolization extent are summarized in table 1. The total procedure time was significantly shorter, the number of injections was significantly lower, the median time per injection was significantly longer, and the embolization extent was significantly higher for groups A and C. The number of injection stops due to reflux (for both models) and the number of injection stops due to distal or venous embolization (in vitro only) were significantly lower for the MBC groups. The required volume of LEA was significantly lower for the MBC group in the in vivo model only. The number of injection stops due to embolization of the contralateral RM did not differ significantly. The spread of the data was lower for the MBC groups (eg, IQR of the embolization extent 10% for group A versus 32% for group B in the in vivo model).

Preinterventional diagnostic angiography of the rete mirabile and postinterventional X-ray scans with an example analysis of the embolization extent. (A) In preinterventional digital subtraction angiography, the respective side of the rete mirabile was delineated. (B) Postinterventional X scan. (C) After deflation and removal of the micro-balloon catheter, the embolized portion of the rete mirabile was delineated. In this example, the delineated area was 1.25 cm² in the preinterventional angiogram and 1.18 cm² in the postinterventional X-ray scan, resulting in an embolization extent of 94%.

Illustration of the in vitro embolization model with an example X-ray after balloon-assisted embolization. (A) Photograph of the in vitro embolization model. (B) X-ray scan of the embolization model, filled with pure iodinated contrast agent for definition of the 28 honeycomb-like sections. (C) Example of an X-ray scan obtained after balloon-assisted embolization. Note the complete filling of the artificial nidus (28 of 28 filled sections) and the radiopaque markers of the deflated balloon in the afferent tube.
Embolization characteristics and embolization extent
Histopathological findings are shown and explained in figure 4. The size of the embolized blood vessels (80–400 µm) was similar for groups A and B. The vessels, especially the distal part of the RM, appeared more extensively filled in group A. However, no quantitative or qualitative analysis of the embolization extent was performed in histopathology since preparation artifacts (dissolving of LEA during histopathological investigation) preclude a meaningful analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Histopathological findings. Elastica van Giesson staining, 12x magnification (right) and 40x magnification (left). Example shown for group A. Precipitating hydrophobic injectable liquid (PHIL) was identified as amorphous material of white appearance within the blood vessels of the rete mirabile (black asterisks), accompanied by fibrin and thrombus, which was localized within and adjacent to the PHIL cast. In this acute setting, no signs of damage to the internal elastic membrane (white asterisk), and no extravasation of liquid embolic agent, hemorrhage, necrosis, or signs of inflammation were observed.
Discussion
In this study, balloon-assisted embolization and standard embolization were compared in an experimental in vivo and in vitro embolization model. Several advantages of balloon-assisted embolization over standard embolization were demonstrated. The embolization extent (as a marker of therapeutic efficacy in the clinical setting) was significantly improved. Furthermore, balloon-assisted embolizations were more effective, with a smaller number of injections and longer injection times. Procedure times were significantly shorter, an aspect which is highly relevant with respect to patient safety and the risk of complications.1–3 Also, the number of reflux events was significantly lower. As indicated above, every reflux event increases the risk of embolization of non-target arteries and of catheter entrapment.7–9 The required volume of LEA was lower for the MBC group in the in vivo model, which can be explained by LEA inside the APA in the SMC group, caused by reflux. The lower spread of the data (embolization characteristics and extent) for the MBC groups indicates a higher grade of reproducibility for balloon-assisted embolization. The lack of extravasation of PHIL and of LEA-induced damage to the vessel wall (disintegration, major inflammation or necrosis) in this acute setting is a relevant safety issue and is in line with previous studies.20 22
Different dual-lumen balloon catheters are commercially available. In the majority of published studies, the Scepter C or Scepter XC (MicroVention) catheter was used for the treatment of AVMs or dAVFs.8 14 23 For these catheters, feasibility, safety and efficacy of balloon-assisted embolization were demonstrated with lower fluoroscopy and procedure times, more efficient injections, and better embolization control.8 14 23 Another small balloon catheter on the market is the Eclipse 2 L (Balt, Montmorency, France). For this device, to the best of our knowledge, no data have been published on liquid embolization. To exemplify their size, these catheters have a distal tip outer diameter of 2.1 F (Scepter C and XC) and 2.0 F (Eclipse 2 L). The difference in size (of the catheter and also of the balloon) from the MBC investigated in this study, which has a distal tip outer diameter of 1.6 F, is comparatively high and may be crucial in special situations. As initially indicated, even though these catheters are considered to be relatively small, they can be too big for navigation into distal arteries, and inflation in these arteries may be too risky, especially in the treatment of complex cerebral AVMs and dAVFs with small feeding arteries and with a high risk of non-target embolization.8 14 15 In this context, extra-small dual-lumen MBCs can be advantageous or can make even difficult-to-treat or untreatable lesions treatable.
Despite the potential advantages of balloon-assisted embolization, this procedure has a risk of complications, which are not encountered in standard embolizations. The number of balloon-related complications was small in reported studies.8 11 13–15 23 Nonetheless, balloon-assisted embolization requires a high level of experience and expertise in neurointerventions and familiarity with the device which is being used.
Minor reported complications include proximal movement of the inflated balloon caused by high injection pressures, spontaneous deflation of the balloon during embolization, catheter entrapment, and catheter fracturing.13 23 24 Two major complications of balloon-related damage to the feeding artery have been described. In treating 20 patients with AVMs, Spiotta et al reported one case of rupture of the feeding artery on balloon inflation.23 Jagadeesan et al reported rupture of an A3 segment of the anterior cerebral artery caused by inadvertent balloon overinflation, which led to an intracerebral hematoma with subsequent permanent neurological deficit.8 Another possible balloon-related complication is early distal embolization, bearing the risk of embolic strokes and of premature closing of draining veins, potentially leading to a sudden increase of the intranidal pressure with subsequent bleeding.11 25 In this experimental study, distal embolization was not significantly more common when applying balloon assistance.
One case of spontaneous balloon deflation with subsequent reflux was observed in the in vivo setting of this experimental study. To prevent this complication, careful observation of the balloon during the embolization is mandatory. Furthermore, one case of distal migration of the LEA cast was observed in the in vitro setting, probably caused by incomplete precipitation of the cast. Solidification of precipitating LEAs results after dissipation of DMSO out of the cast into the blood. This can be reduced by a slowed or arrested blood flow, which results after balloon occlusion. This phenomenon might be of particular relevance when there is only a single feeding artery, as was the case in our in vitro experiment. To prevent this complication, the waiting time before balloon deflation should be long enough (considering the specific precipitation time of the LEA which is being used) and after deflation the LEA cast should be carefully observed for stability.
Our study had some limitations. First, the navigability of the MBC was not specifically investigated. This aspect should be investigated in further experimental studies and in the clinical setting. Second, the number of experiments was relatively small; however, the findings were consistent in the different groups. Third, transferability of experimental models to clinical practice is generally limited. Fourth, the creation of an AVF might have made the in vivo model more similar to an AVM. Fifth, only PHIL was used as LEA; other LEAs might have led to different results and should be tested in future studies.
Conclusions
Extra-small dual-lumen micro-balloon catheters can improve endovascular embolization in an in vivo and in vitro embolization model in comparison with standard microcatheter embolization. The specific features of balloon-assisted embolization have to be respected in order to prevent complications.
References
Footnotes
Contributors All listed authors contributed to the work. DFV, CMS, and MAM acquired, analyzed, and interpreted data for the work; designed the study; drafted the manuscript and approved the final manuscript. RO, TDD, and AvD acquired, analyzed, and interpreted data for the work; drafted the manuscript and approved the final manuscript. HUK and MB analyzed and interpreted data for the work; drafted the manuscript and approved the final manuscript.
Funding The study was technically supported by MicroVention (Tustin, USA) without any influence on data acquisition, analysis and writing of the manuscript.
Competing interests DFV: has received travel support outside this work from MicroVention and Stryker GmbH & Co. KG; HUK: reports grants, personal fees and non-financial support from Siemens, personal fees from Boehringer Ingelheim, personal fees and non-financial support from Bayer, personal fees from GSK, personal fees from Novartis, personal fees from Astra Zeneca, personal fees from Philips, personal fees from Bracco, outside the submitted work. MB: reports board membership: DSMB Vascular Dynamics; consultancy: Roche, Guerbet, Codman; grants/grants pending: DFG, Hopp Foundation, Novartis, Siemens, Guerbet, Stryker, Covidien; payment for lectures (including service on speakers bureaus): Novartis, Roche, Guerbet, Teva, Bayer, Codman; MAM: has received consulting honoraria, speaker honoraria, and travel support outside this work from Codman, Covidien/Medtronic, MicroVention, Phenox, and Stryker. All other authors have nothing to disclose.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.