Article Text

Abstract
Objective To analyze outcome and its predictors after endovascular treatment (ET) in stroke patients suffering from large vessel occlusion with large pre-treatment infarct cores defined by an Alberta Stroke Program Early CT Score (ASPECTS) <6.
Methods We analyzed data from an industry-independent, multicenter, prospective registry (German Stroke Registry – Endovascular Treatment) which enrolled consecutive patients treated by ET (June 2015–April 2018) with different devices. Multivariate logistic regression analyses identified predictors of independent outcome (IO) defined as a modified Rankin Scale (mRS) 0–2, and mortality at 90 days in patients with ASPECTS <6.
Results Of 1700 patients included in the analysis, 152 (8.9%) had a baseline ASPECTS <6. Of these, 33 patients (21.6%) achieved IO, and 68 (44.7%) were dead at 90 days. A lower age, lower baseline National Institutes of Health Stroke Scale (NIHSS) score, and successful recanalization (defined as modified Thrombolysis in Cerebral Infarction Score, mTICI 2b/3) were predictors of IO. Successful recanalization had the strongest association with IO (OR 7.0, 95% CI 1.8 to 26.8). Pre-treatment parameters predicting IO were age <70 years (sensitivity 0.79, specificity 0.69) and NIHSS <12 (0.57 and 0.94). A higher age, a pre-stroke mRS score >1, and failed recanalization were predictors of death.
Conclusions A substantial proportion of stroke patients with an ASPECTS <6 can achieve independence after thrombectomy, in particular, if they are younger, have only moderate baseline stroke symptoms, and no relevant pre-stroke disability. These results may encourage considering thrombectomy in low ASPECTS patients in clinical practice until randomized trials are available.
- stroke
- thrombectomy
- angiography
Statistics from Altmetric.com
Introduction
Recently, multiple clinical trials demonstrated that endovascular thrombectomy (ET) improves functional outcome in patients suffering from acute ischemic stroke caused by anterior circulation large vessel occlusion (LVO).1 Patients with large pre-treatment infarct cores, who are potentially prone to harm with a higher hazard of poor outcome and a higher risk for symptomatic intracerebral hemorrhage (sICH),2 were excluded from enrolment in most of these trials. Correspondingly, the benefit of thrombectomy in patients with low Alberta Stroke Program Early CT Score (ASPECTS) is uncertain1 and, thus, ET is not generally recommended for these patients.3 4
Previous studies reported controversial findings with regard to ET in patients with low ASPECTS. Whereas some studies demonstrated barely beneficial effects of ET in patients with large infarction before treatment,5 other studies showed that a good outcome can also be achieved after successful recanalization in this group of stroke patients.6–8 In line with this, an updated analysis from the HERMES collaboration demonstrated a clear benefit for patients with an ASPECTS 3–5, but not 0–2,9 after including additional data, while in the original HERMES analysis no treatment benefit was observed for patients with an ASPECTS 0-5.1 Owing to these contrary findings, no consistent conclusion exists whether ET should be applied or withheld in patients with large pre-treatment infarcts and, thus, no clear therapeutic recommendations are currently available for ET in patients with low ASPECTS.
However, in clinical practice, neurologists and neuroradiologists are daily confronted with the decision to treat or not to treat patients with large pre-treatment infarct cores who are admitted to hospital in the recanalization time window with a reachable thrombus for ET. Therefore, information on clinical factors associated with a favorable outcome after ET in this subgroup of patients may inform interventionalists in their decision to select adequate patients for ET.
The purpose of the present study was to study the outcome of ET in patients with an ASPECTS <6 and to identify predictors of independent outcome in these patients.
Methods
Patient population and data collection
The patients analyzed in the present study are derived from the German Stroke Registry – Endovascular Treatment (GSR-ET; ClinicalTrials.gov, identifier: NCT03356392). The study design has been described in detail elsewhere,10 and primary findings have been reported recently.11 Briefly, GSR-ET is an ongoing prospective, multicenter registry including consecutive patients suffering from acute ischemic stroke treated by ET in participating sites in Germany. For the present analysis, all patients enrolled between June 2015 and April 2018 at 25 sites, comprising both university and community hospitals, were included. The patients were at least 18 years of age. The treatment decision was made interdisciplinary between a vascular neurologist and an interventional neuroradiologist on a case-by-case basis. Factors that were taken into account for treatment decision included the elapsed time from symptom onset, stroke severity assessed by the National Institutes of Health Stroke Scale (NIHSS) on admission, site of vessel occlusion, the ASPECTS which was adjudicated by the interventional neuroradiologist of each participating center either on CT or MRI, and the pre-stroke disability measured by the mRS and extended imaging with CT-perfusion or MRI to identify potentially salvageable brain tissue, in particular, beyond 6 hours of symptom onset or if symptom onset time was uncertain. Intravenous thrombolysis therapy (IVT) was applied prior to ET, if appropriate, according to national and international guidelines. Different devices were used according to the preference of the interventional neuroradiologist. Follow-up brain CT scans were obtained 24 hours after intervention. In this subgroup analysis we included data of patients with anterior circulation stroke, with available 90 days' follow-up assessments, and baseline ASPECTS.
Ethics approval
The study was approved by the responsible ethics committees of all participating sites. Written informed consent was obtained from the patient or the proxy. Consent was waived if patients died before consent could be obtained or lacked the capacity to give consent and no proxy was available.
Statistical analysis
Standard descriptive statistics are reported as median and IQR for continuous variables, and numbers and percentage for categorical variables. For between-group comparisons of categorical variables, χ2-tests or Fisher exact tests were used, as appropriate. Mann–Whitney U tests were employed for continuous variables.
Logistic regression analysis was applied in the subgroup of patients with an ASPECTS <6 to identify predictors of an independent outcome (defined as mRS 0–2) and predictors of death 90 days after stroke. The variables sex, concomitant IVT, direct referral to a comprehensive stroke center (mothership) or transfer from a primary stroke center (ship), side of vessel occlusion (right/left), successful recanalization (defined by modified Thrombolysis in Cerebral Infarction Score, mTICI 2b/3), and pre-stroke mRS (categorized to 0–1 and 2–5) were considered as dichotomous independent variables, whereas age, baseline NIHSS, and the time from symptom onset to recanalization were considered as continuous independent variables.
Multivariate logistic regression analyses were applied, employing a stepwise backward selection method containing predictor variables in the final model displaying P-values <0.05. Logistic regressions were run on data sets in which missing data were estimated by multiple imputation, employing a fully conditional specification approach. Of the analyses on multiple imputed data sets, the pooled results are reported. OR with 95% CIs and P-values are presented.
Receiver operating characteristic (ROC) analyses were performed on the status variable mRS 0–2, reflecting independent outcome, using age and baseline NIHSS as test variables, to identify best predictors of independent outcome. Areas under the curve (AUC) were computed and tested for significant deviations from AUC=0.5 (under H0). Cut-off values were determined for both test variables by determining the maximum Youden index across the data value ranges.
All analyses were considered exploratory and adjustments for multiple testing were therefore not applied. Two-sided P-values <0.05 were considered statistically significant. All statistical analyses were performed using SPSS (Version 25.0; IBM, Armonk, New York).
Results
Patients’ characteristics and between-group comparison (ASPECTS <6 vs ASPECTS ≥6)
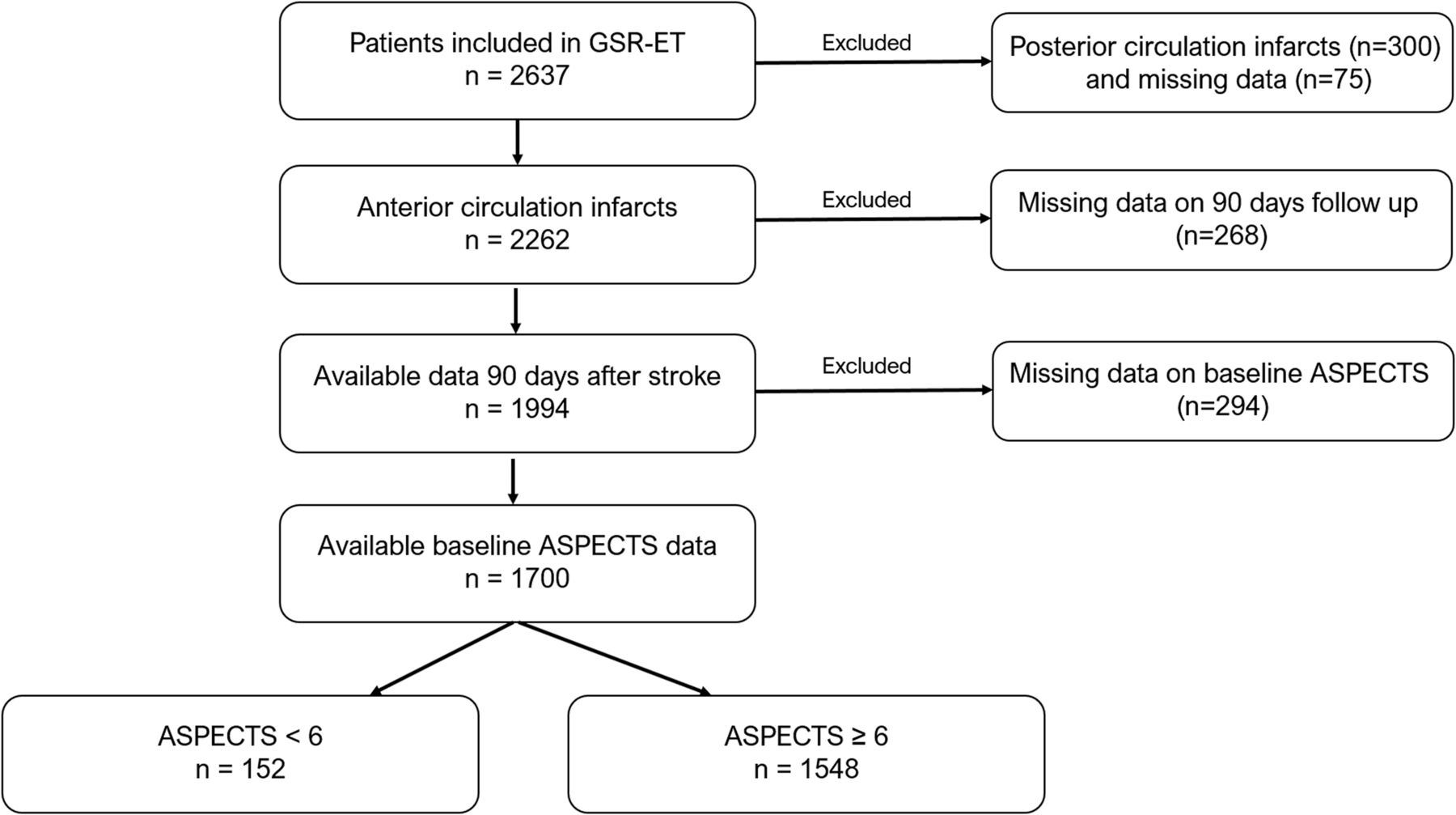
Of 2637 patients enrolled in the registry, 1700 patients met the criteria for the current study. Of these, 152 (8.9%) patients had an ASPECTS <6 (see figure 1). In 1576 patients the ASPECTS was determined by CT, in 116 patients by MRI. In eight patients the imaging modality, in which the ASPECTS was adjudicated, was not documented.
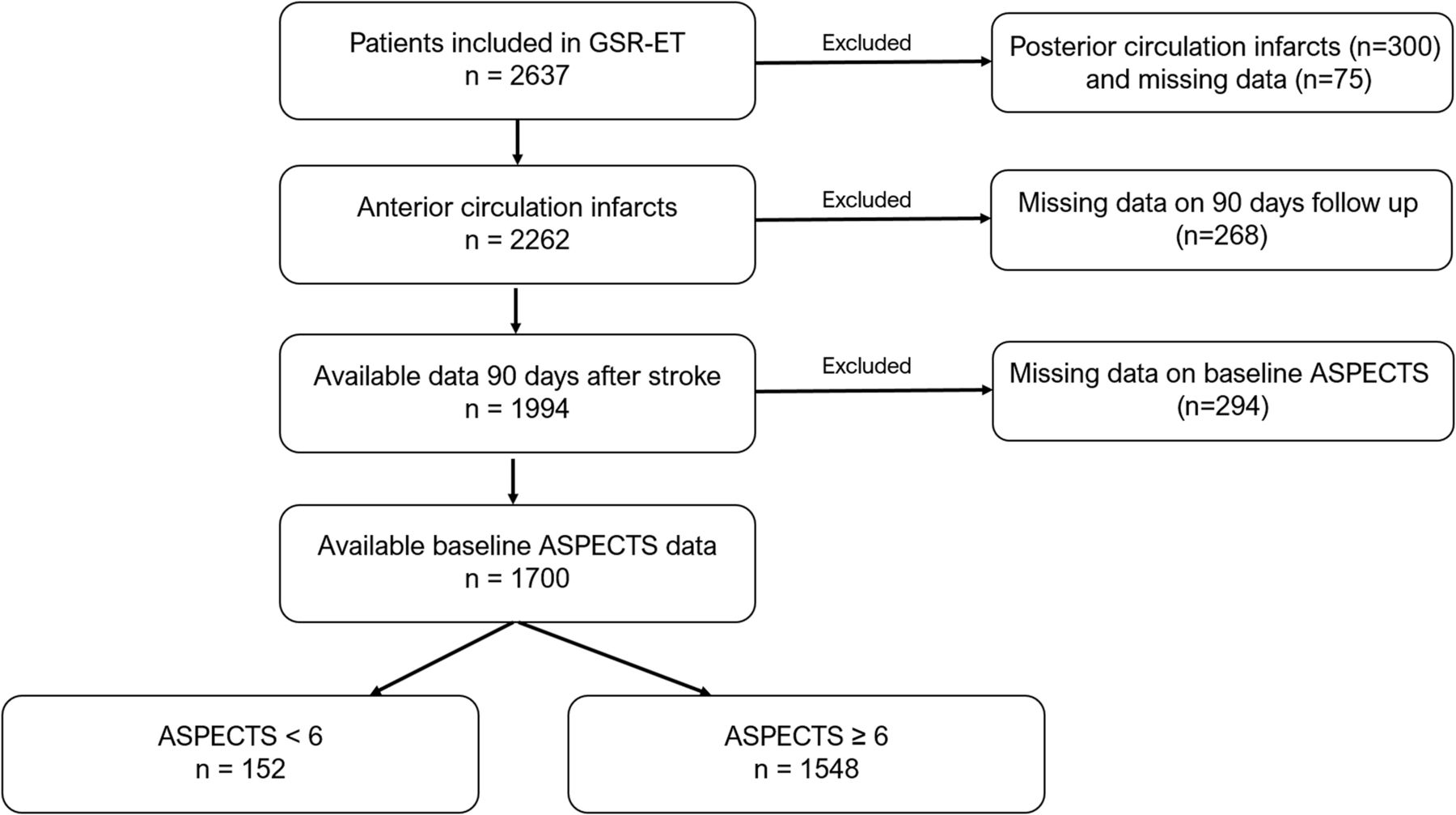
Flowchart of patients included in this subanalysis of the GSR-ET.
The results of group comparison between patients with ASPECTS <6 and ≥6 are displayed in table 1. Patients with an ASPECTS <6 were significantly younger (73 vs 76 years; P=0.041), had higher NIHSS score values on admission (17 vs 15; P<0.001), received less frequently concomitant IVT (47.4% vs 57.3%; P=0.020), and achieved less often a successful recanalization (74.3% vs 83.0%; P=0.010). They also suffered more frequently from right-hemispheric stroke (58.6.4% vs 47.4%; P=0.011). The time elapsed from symptom onset to groin puncture and flow restoration was longer in the group of patients with a larger pre-treatment infarct core (212.5 min vs 192 min, P=0.023; 264 min vs 241 min, P=0.032, respectively).
Baseline characteristics, procedural and outcome parameters according to the subgroups of patients, ASPECTS <6 versus ASPECTS ≥6
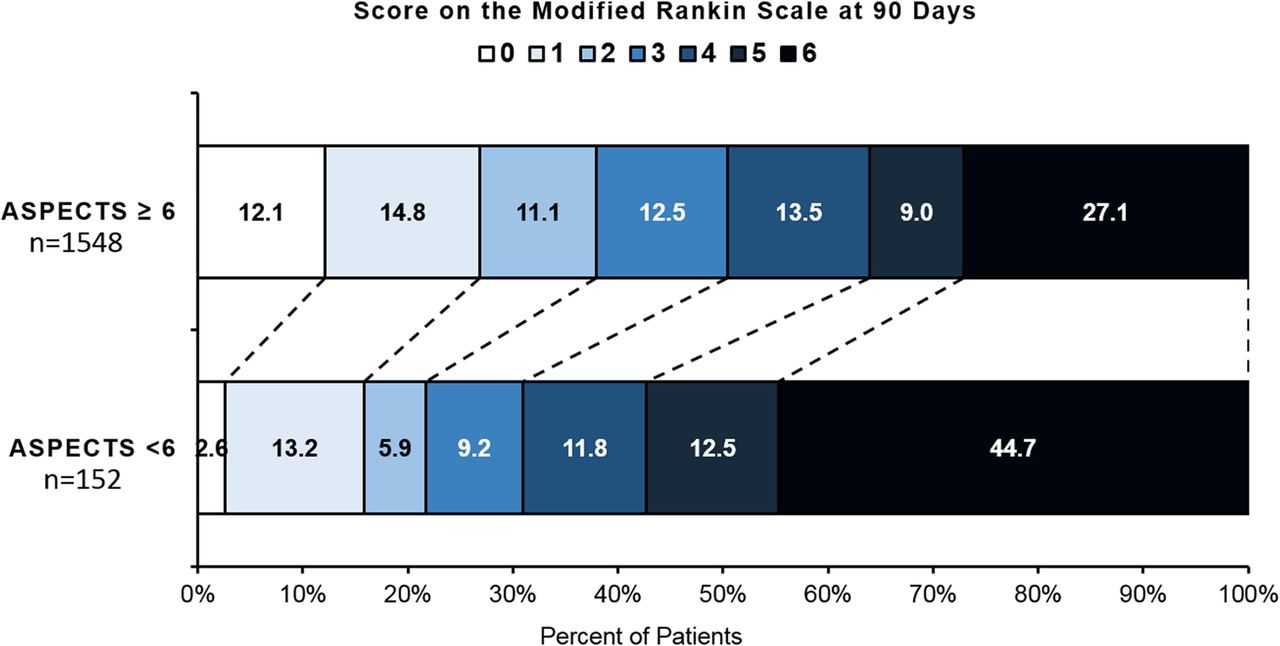
Patients with an ASPECTS <6 suffered more frequently from any ICH, which was detected on follow-up CT within 24 hours after treatment (22.4% vs 14.1%; P=0.012). They also had lower rates of independent outcome (21.7 vs 38.0, P<0.001) and higher rates of death (44.7% vs 27.1%, P<0.001) or death and dependence (57.2 vs 36%, P<0.001) at 90 days than patients with ASPECTS 6–10. The distribution of the mRS scores at 90 days in both subgroups of patients is displayed in figure 2.

{kind=link}
{kind=link}
The distribution of the mRS scores at 90 days according to the subgroups of patients. GSR-ET, German Stroke Registry – Endovascular Treatment; mRS, modified Rankin Scale.
Predictors of independent outcome
Results of the multivariate logistic regression analyses are shown in table 2A. In the group of patients with an ASPECTS <6, age, baseline NIHSS score, and successful recanalization were independent predictors of independent outcome. Successful recanalization was associated with independent outcome with an OR of 7.0 (95% CI 1.8 to 26.8).
Multivariate logistic regression analyses in the subgroup of patients with an ASPECTS <6
Cut-off values for prediction of independent outcome
ROC analysis identified a cut-off value of <70 years of age (sensitivity 78.6%, specificity 69.4%, positive predictive value (PPV) 42.3%, negative predictive value (NPV) 91.9%) and <12 points on the NIHSS (sensitivity 57.1%, specificity 93.9%, PPV 72.7%, NPV 88.5%) as best predictors of independent outcome. Increasing the NIHSS cut-off to <16 resulted in enhanced sensitivity with the trade-off of lower specificity (sensitivity 71.4%, specificity 75.5%, PPV 45.5%, NPV 90.2%).
Predictors of mortality
Multivariate logistic regression analyses identified a higher age, a mRS score >1 before stroke, and failed recanalization as independent predictors of death at 90 days (table 2B). A pre-stroke mRS score >1 was associated with a 3.5-fold higher risk of death 3 months after stroke (OR 3.5, 95% CI 1.0 to 11.5, P=0.043), and failed recanalization was associated with an OR for death of OR 5.2 (95% CI 2.0 to 13.5, P=0.001).
Discussion
Whether patients with large baseline infarcts should be treated by ET still remains uncertain. Our study provides the results of ET in patients with low ASPECTS from a large, prospective, multicenter, industry-independent registry of consecutive patients treated with a large variety of approved devices. Therefore, our study provides important novel data of stroke thrombectomy in clinical practice, outside of randomized controlled trials (RCTs) in which substantial subgroups of patients were excluded. Moreover, the analysis of predictors of independent outcome in patients with a large pre-treatment infarct core provides new insights that may help in guiding endovascular treatment in clinical practice.
In our cohort of patients with anterior circulation stroke 8.7% treated by ET presented with an ASPECTS <6 on admission. As anticipated, these patients had a worse outcome 90 days after stroke than patients with small infarcts before interventional therapy. These findings are consistent with the results of previous studies, in which larger baseline infarcts were associated with poor outcome 90 days after stroke.1 12
In the present study sample, patients with an ASPECTS <6 were younger compared with those with larger baseline infarcts. This is most probably explained by a selection bias resulting from interventionalists’ tendency to be more aggressive in treatment decisions in younger patients.
In addition, we observed more frequently right-hemispheric infarctions in the group of patients with larger baseline infarct cores. One possible explanation is that the clinical symptoms in those patients are less obvious, such as extinction rather than aphasia and so on, so that admission to hospital is more delayed. In fact, this assumption is supported by our finding that the time elapsed from symptom onset to treatment was longer in this patient group. In line with this, concomitant IVT was most likely less frequently applied. Patients with ASPECTS 0–5 also had higher NIHSS scores on admission going along with larger infarct lesions.
With regard to procedural success, recanalization was achieved less frequently in patients with ASPECTS <6. Besides possible differences in underlying pathology or collateral supply, this may be attributed to the neuroradiologists’ decision to stop the intervention earlier owing to the large baseline infarct and the potential risk of complications.13 The 74% rate of successful recanalization in our cohort is similar to 70% successful recanalization reported in a recent registry study of ET in ASPECTS 0-5.13
Finally, patients with ASPECTS <6 suffered more frequently from any ICH within 24 hours after intervention and had a worse mRS score 90 days after stroke than those with ASPECTS 6–10 (22.4% vs 14.1%). However, the reason for the high incidence of any ICH in this subgroup of patients remains speculative. In total, 82.5% of the patients with an ASPECTS <6 and any post-interventional ICH had a successful recanalization, potentially indicating a reperfusion-related occurrence of ICH.
Nevertheless, despite already extended pre-treatment infarct lesions, about one in five patients (21.6%) with an ASPECTS <6 achieved an independent outcome in our study. This is in line with previous reports of ET in low ASPECTS patients that reported 25% achieving an independent outcome in a recent pooled analysis of seven prospective registries of treatment with the Solitaire FR stent retriever,13 and others.6 13–15 Moreover, in a multicenter prospective cohort study patients who were treated by thrombectomy achieved even a higher rate of independent outcome (31%) compared with patients with best medical treatment (31% vs 14%).16 Of note, in that study ET was associated with better functional outcomes, less infarct growth, and smaller final infarct volume than medical treatment. In addition, the updated HERMES meta-analysis including data from seven randomized trials showed a benefit of ET over standard medical care across a broad range of ASPECTS, including ASPECTS 3–5 with 31% of patients treated by ET reaching mRS 0–2 after 90 days as compared with 16% in the control group.9 Our results amend previous reports by including patients treated by a variety of approved devices in a large number of stroke centers at both university and community hospitals. Taken together with previous studies, our findings indicate that substantial proportions of stroke patients with LVO and ASPECTS <6 appear to benefit from ET.
As in virtually all studies of stroke thrombectomy, successful recanalization also was a strong predictor of better outcome in our cohort. Successful recanalization was associated with a seven-fold higher likelihood of an independent outcome. This confirms the findings from previous studies of ET in low ASPECTS patients that consistently identified successful recanalization to be one of the strongest predictors of good outcome in this important subgroup of patients.13 17 18
However, when facing the decision whether to perform ET in patients with already extended infarcts in clinical practice, information on pre-treatment factors associated with a higher likelihood of good outcome, may help in decision-making. In our registry study, a lower age and a lower baseline NIHSS were independent predictors of a better outcome in patients with ASPECTS <6. This is in line with previous reports of worse outcome after ET in older patients,19 20 most probably due to a higher risk of complications and decreased functional reserve.21 22 Higher NIHSS scores at baseline reflecting more severe strokes were also found to be associated with less frequent successful recanalization and consecutively worse outcome after ET in previous studies.23 Moreover, pre-stroke disability reflected by a mRS score >1 was associated with a 3.5-fold higher risk of death after stroke thrombectomy in our study, indicating that stroke patients suffering from LVO with a higher grade of pre-stroke disability are also less likely to benefit from thrombectomy.
Of note, the parameters' age, baseline NIHSS, and pre-stroke mRS scores are factors that are easily available in the emergency situation and may have an impact on treatment decisions. In our sample, an age of <70 years was the best cut-off to identify those patients with ASPECTS <6 who are most likely to achieve an independent outcome after thrombectomy. This finding adds to the results of previous studies,14 24 in which age-dependent thresholds of the ASPECTS for treatment decision were found. The same cut-off value of 70 years for treatment consideration was demonstrated and an age-adjusted stroke-volume threshold for ET decision was suggested with a lower stroke volume cut-off for elderly patients and, conversely, a higher cut-off volume for patients younger than 70 years in a previous study.24 In another study, a better outcome in stroke patients younger than 70 years with large baseline infarction treated by thrombectomy was reported.14
Best NIHSS cut-off values to identify patients likely to achieve an independent outcome showed a trade-off between sensitivity and specificity, with higher sensitivity but lower specificity for higher NIHSS cut-offs, and best predictive values for NIHSS cut-offs between 12 and 16.
Limitations
Our study has several limitations that have to be acknowledged. Our registry included patients treated by ET based on individual treatment decisions by local interventionalists. This may lead to a selection bias toward patients in whom ET was deemed to be successful. Furthermore, the ASPECTS was adjudicated by the interventional neuroradiologists of each participating center, instead of using an imaging core laboratory. As this was not a randomized controlled study and, thus, lacks a patient group that received best medical treatment instead of ET, we cannot judge the efficacy of ET.
Conclusion
Given that most RCTs excluded patients with large baseline infarcts, the effect of ET in this important subgroup of patients has not yet been established by RCTs. This study provides preliminary evidence that ET can be applied in patients with a baseline ASPECTS <6. Our findings underscore that ET is not unequivocally deleterious in patients with large pre-treatment infarct cores and rather advocate that these patients should be subjected to ET, in particular, if they are younger than 70 years, have only moderate to severe stroke symptoms at baseline, and no relevant pre-stroke disability. Successful recanalization is the strongest predictor of independent outcome in stroke patients with low ASPECTS. These results may encourage clinicians to consider thrombectomy in patients with low ASPECTS until results of randomized trials, such as the TENSION trial (ClinicalTrials.gov Identifier: NCT03094715)25 or the TESLA (NCT03805308), SELECT2 (NCT03876457), and RESCUE-Japan LIMIT (NCT03702413) trials, are available.
Acknowledgments
GSR-ET Steering Committee Investigators: Universitätsklinikum Hamburg-Eppendorf: Professor Dr C. Gerloff, Professor Dr J. Fiehler, Professor Dr G. Thomalla, Dr med. A. Alegiani; Klinikum rechts der Isar: Dr Boeckh-Behrens, Dr Silke Wunderlich; Uniklinik RTWH Aachen: Dr Arno Reich, Professor Dr Martin Wiesmann; Universitätsklinik Tübingen: Professor Dr Ulrike Ernemann, Dr Till-Karsten Hauser; Charité – Campus Benjamin Franklin und Campus Charité Mitte, Berlin: Dr Eberhard Siebert, Professor Dr Christian H. Nolte; Charité - Campus Virchow Klinikum, Berlin: Dr Sarah Zweynert, Dr Georg Bohner; Sana Klinikum Offenbach: Dr med. Alexander Ludolph, Dr med. Karl-Heinz Henn; Uniklinik Frankfurt/ Main: Professor Dr Waltraud Pfeilschifter, Dr Marlis Wagner; Asklepios Klinik Altona: Professor Dr Joachim Röther, Professor Dr Bernd Eckert; Klinikum Altenburger Land: Professor Dr Jörg Berrouschot, Dr Albrecht Bormann; Uniklinik Bonn: Professor Dr med. E. Hattingen, Professor Dr Gabor Petzold; Klinikum Hanau: Dr Sven Thonke, Professor Dr Christopher Bangard; Klinikum Lüneburg: Dr Christoffer Kraemer; Uniklinik München (LMU): Professor Dr Martin Dichgans, Dr Frank Wollenweber, Dr Lars Kellert, Dr Franziska Dorn; Georg-August. Universität Göttingen: Dr Marios Psychogios, Dr Jan Liman; Klinikum Osnabrück: Dr Martina Petersen, Professor Dr Florian Stögbauer; Uniklinik Würzburg: Dr Kraft, Professor Dr M. Pham; Bezirkskrankenhaus Günzburg: Dr med. Michael Braun, Professor Dr Gerhard F. Hamann; Klinikum Bremen Mitte: Professor Dr Andreas Kastrup, Dr Christian Roth; Universitätsmedizin Mainz: Professor Dr Klaus Gröschel, Dr Timo Uphaus; Kliniken Koeln: Professor Dr Volker Limmroth.
References
Footnotes
Contributors MD-C: Substantial contributions to the conception and design of the work. Acquisition, analysis and interpretation of data. Drafting the work and revising it critically for important intellectual content. HP, CB, JF: Analysis and interpretation of data. Revising the work critically for important intellectual content. FF, HL, GB, AA: Acquisition of data. Revising the work critically for important intellectual content. CG: Analysis and interpretation of data. Drafting the work and revising it critically for important intellectual content. GT: Substantial contributions to the conception and design of the work. Analysis and interpretation of data. Drafting the work and revising it critically for important intellectual content. All authors gave their final approval of the version published and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests AA reports honoraria as speaker from Bayer Vital. JF receives research support from the German Ministry of Science and Education (BMBF), German Ministry of Economy and Innovation (BMWi), German Research Foundation (DFG), European Union (EU), Hamburgische Investitions- und Förderbank (IFB), Medtronic, Microvention, Philips, Stryker; and serves as a consultant for Acandis, Boehringer Ingelheim, Cerenovus, Evasc Neurovascular, MD Clinicals, Medtronic, Medina, Microvention, Penumbra, Route92, Stryker, Transverse Medical. CG serves on scientific advisory boards for Bayer Vital, Boehringer Ingelheim, ActicorBiotech, Amgen, and Prediction Biosciences; has received funding for travel and/or speaker/ consulting honoraria from Bayer Vital, Boehringer Ingelheim, Sanofi Aventis, Amgen, EBS Technologies, GlaxoSmithKline, Lundbeck, Pfizer, Silk Road Medical, and UCB, and Abbott; serves on editorial boards for INFO Neurologie & Psychiatrie and Aktuelle Neurologie and as editor of the textbook Therapie und Verlauf neurologischer Erkrankungen; has received grants to supporting employees/ scientists of his clinic from Merz Pharmaceuticals, Allergan, Novartis, and NeuroConn; and receives research support from Deutsche Forschungsgesellschaft, the European Union, Wegener Foundation, Schilling Foundation, and Werner-Otto- Foundation. GT has received personal fees as consultant or lecturer from Acandis, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb/Pfizer, Daichi Sankyo, Stryker, and research grants from Bayer, Federal Ministry for Economic Affairs and Energy (BMWi), Corona-Foundation, German Research Foundation (DFG), Else Kröner-Fresenius Foundation, European Union (Horizon 2020), German Innovation Fund.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article.