Article Text

Abstract
Objective Multiple intracranial aneurysms are common. While sequential clipping of multiple aneurysms during a single open surgical procedure has been reported, the same is not true for endovascular coiling. We present our experience describing the safe coiling of multiple aneurysms in the same setting.
Methods Retrospective review of our coiling log between 2006 and 2009 showed six cases in which multiple aneurysms were coiled in the same session.
Results All patients were coiled using the same microcatheter. Distal aneurysms were coiled first. Good occlusion rates were achieved in all cases. There were no thromboembolic events or procedure-related rupture or mortality.
Conclusion In addition to safety and efficacy, cost savings are expected when coiling multiple aneurysms in the same procedure.
- Aneurysms
- angiography
- coil
- endovascular
- intervention
- multiple sessions
- single session
Statistics from Altmetric.com
Introduction
Intracranial aneurysms (IAs) affect up to 10% of the population worldwide.1 2 It is the risk of rupture, resulting in subarachnoid hemorrhage (SAH) with its associated morbidity and mortality that gives them such importance.3 Thus, once ruptured, they should be secured by either endovascular coiling or clipping.4 5 It has been established that history of SAH increases the risk of re-rupture as well as rupture of other aneurysms.6 7
While treatment of the culprit aneurysm in patients with SAH is straightforward, it is not known when would be the best time to address the remaining aneurysms in those with multiple aneurysms. Multiple IAs account for 15%–33.5% of all cases.8 It is reasonable to treat these aneurysms in the same session, if feasible. There are series describing the safety of clipping multiple aneurysms in the same surgery as well as coiling followed by clipping.9–11 However, the literature lacks data about simultaneous coiling of multiple aneurysms.12 We present here our experience of the safety and efficacy of coiling multiple aneurysms in the same setting.
Methods
At our institution, endovascular coiling is usually pursued if the aneurysm is amenable to this approach. If the aneurysm is not amenable to coiling or it has an unsuitable morphology such as a broad-based neck, then clipping is the next option. Retrospective review of the coiling log (2006–2009) at our institution was performed. Multiple IAs that were treated by endovascular therapy either as an emergency or on an elective basis were identified. Both coiling and stent-assisted coiling were included. We excluded cases in which the other aneurysm and/or aneurysms were clipped unless there were at least two aneurysms that were coiled.
Criteria for coiling multiple aneurysms
The decision on how many aneurysms should be treated was based on the following criteria:
Ease of access,
Short duration of anesthesia,
Symptoms being attributable to their anatomical location,
Saccular morphology,
Aggregation of risk factors such as smoking, poorly controlled hypertension and family history or previous medical history of aneurysms/aneurysmal SAH.
Procedure variables
Details of the sequence of coiling, types and numbers of guide catheters and microcatheters were collected. Intraoperative as well as postoperative complications were recorded.
Variables
The outcome was measured using the Raymond classification to define technical success (table 1). Follow-up angiogram was scheduled for every patient, 2–3 months after the interventional procedure. Also, the first clinical follow-up was arranged a month after the procedure. Costs for aneurysmal treatment in one session versus multiple sessions were compared using the Medicare Severity-Diagnosis Related group (MS-DRG) national average for 2010. We used MS-DRG 27 corresponding to endovascular intracranial procedure without complication and MS-DRG 22 corresponding to intracranial vascular procedure with a principal diagnosis of hemorrhage without complications. These codes were used to simplify comparison as payments differ by region, location and teaching status.13 Also, it is difficult to account for different costs of materials, anesthesia time, angiography suite time and personnel. We also calculated length of stay for each of these cases and compared the mean with the average length of stay of uncomplicated and complicated aneurysmal cases at our institution.
Raymond classification
Results
A total of six cases of multiple IAs undergoing coiling in the same setting were identified (table 2). All patients were female with ages between 44 and 66 years. The total number of aneurysms was 18 (per patient range 2–5). Sixteen aneurysms were considered for treatment of which only three were clipped because they were not suitable for coiling (table 3). Only two patients presented with SAH. The other aneurysms were incidental. Presenting symptoms included: headache (four), dizziness (three) and nausea (one).
Characteristics of patients
Aneurysm characteristics and outcome
In case 3, which presented with SAH, all aneurysms (two) were coiled. However, in case 5, which also had SAH, only two out of three aneurysms were coiled while the third was clipped because it was not suitable for coiling. In the remainder of the cases, the decision on how many aneurysms should be treated was based on multiple factors: ease of access, duration of anesthesia, being possibly symptomatic and patient wishes.
The highest number of aneurysms treated in a single session was three while the remainder of our cases had two aneurysms coiled in the same procedure (table 3). In all cases, the distal aneurysm was coiled first followed by the next one. Coiling was performed using the same microcatheter. Complete occlusion was seen in eight aneurysms (62%) while the remaining aneurysms (five aneurysms) had subtotal occlusion on the immediate postintervention angiogram. There was no procedure-related rupture, morbidity or mortality. None of the patients had thromboembolic events. Follow-up angiogram was available to all patients except for two who were lost to follow-up (table 3). Follow-up averaged 16.7 months (range 10–29 months). Only two aneurysms on the last follow-up angiogram became subtotally occluded. Length of stay ranged between 2 and 11 days (average 4.6 days).
MS-DRG 27 and 22 national average for 2010 was US$14 842 for uncomplicated aneurysms and US$33 160 for complicated aneurysms, respectively.14 Thus, the expected cost of single-session coiling in our series of two cases of SAH and four cases of elective coiling was US$66 320 (2×$33 160) and US$59 368 (US$4×14 842), respectively, with a total cost of US$125 688.
Case illustration
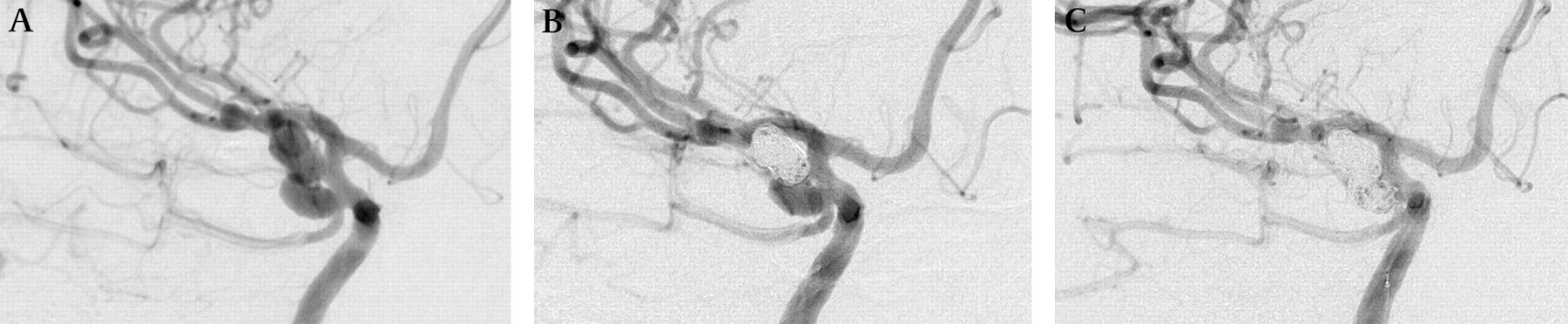
An African American woman presented with severe headache. Emergent head CT showed SAH in the right perimesencephalic cisterns with extension into the Sylvian fissure. Head CT angiogram showed multiple IAs: posterior communicating artery (PCOM) bilobed aneurysm and left middle cerebral artery (MCA) aneurysm. Diagnostic cerebral angiogram was performed emergently and showed right PCOM aneurysm (6×4×3 mm), right anterior choroidal artery (7×4×2.5 mm) and right MCA bifurcation aneurysm (3.5×3×3.5 mm). Only the first two aneurysms (figure 1) were coiled in the sequence anterior choroidal aneurysm followed by PCOM aneurysm. The intervention was performed using the same catheter. The first aneurysm was completely occluded. Only a small residual neck was seen on the PCOM aneurysm (figure 1). There were no thromboembolic events, rupture or procedure-related mortality. The right MCA aneurysm was not treated in this case because it was unruptured.
{kind=link}
Lateral anterior oblique head digital subtraction angiogram showing right posterior communicating artery and right anterior choroidal artery aneurysms. (A). Precoiling. (B). Status post coiling of right anterior choroidal artery aneurysm, (C). Status post coiling of right posterior communicating artery aneurysms.
Discussion
One advantage of surgical clipping over endovascular coiling is the ability to clip multiple aneurysms as long as they are within reach of the neurosurgeon.12 15 However, there is no reason why this is not achievable by the endovascular method. Procedural success in coiling is based on the percentage of occlusion of the aneurysm after the coils are deployed. Once the coil is detached within the confines of the aneurysmal cavity it remains stable allowing treatment of other aneurysms.4 5 16
An important benefit of managing multiple aneurysms simultaneously in patients presenting with SAH is avoiding the higher rupture risk of the remaining aneurysms associated with delayed treatment. It is known that the presence of a history of SAH increases the cumulative 5-year rupture rate to 1.5% and 3.4% for aneurysms <7 mm in the anterior and posterior circulation, respectively.7 However, it should be mentioned that those aneurysms are usually treated in short follow-ups within several months. Therefore, the actual risk of rupture is low but definitely higher than unruptured aneurysms. Further, there are reports in the literature of coiling followed by clipping of multiple aneurysms with good outcome.10 12
Additionally, there is the benefit of avoiding general anesthesia (GA) for multiple procedures. Total 30 day perioperative deaths were reported as ∼1 in 200 elective cases. GA-related death was 1 in 50 000 cases. Aspiration and cerebrovascular accident were reported at 1 in 3000 and 1 in 100, respectively.17 However, it should be mentioned that coiling multiple aneurysms would prolong the time in which patients remain under GA thus slightly increasing the complication rates.17 However, they are still lower than those associated with multiple surgeries.
Cost savings are also expected. Instead of treating the patient in multiple sequential procedures, treatment can be performed in one setting. Savings include GA, cost of operating the angiographic suite, intensive care unit and regular ward bed stay.13 The interventionalist's expenses are not saved because they can bill for each aneurysm separately. Unfortunately, quantifying the exact amount saved is not practical as payments differ by location, region and teaching status. This is also complicated by the presence of SAH as well as complications and comorbidities. Thus, we decided to use the MS-DRG national average for 2010. Thus our combined cost of treating multiple complicated and uncomplicated aneurysms in a single setting was US$125 688. On the other hand, coiling each aneurysm separately would cost US$66 320 for two ruptured aneurysms and US$163 262 for 11 unruptured aneurysms with a total cost of US$229 582. Thus, the expected savings in our series would total US$103 894. Further, there was no difference in length of stay when comparing this series with aneurysms of similar characteristics coiled at our institution (range 3–10 days, average 4.8 days).
All of our cases were coiled using the same microcatheter. It was our preference to start coiling the distal aneurysm first. We wanted to avoid potential technical difficulties that would not allow us to go distally, mainly coil prolapse. In our case series, six patients were treated in the same session. Our results compare well with those reported in the literature.18–20 There were no thromboemblic events or procedure-related rupture or mortality.
Conclusion
Addressing multiple aneurysms in the same session is as safe and as effective as consecutive treatment. In addition, cost savings are expected.
Key messages
Multiple intracranial aneurysms are frequent.
There are limited data in the literature about the safety and efficacy of coiling multiple aneurysms in the same session.
Coiling multiple aneurysms in the same session is safe and effective similar to multiple sessions.
Additional benefits include cost savings and avoiding the risks and complications of repeated general anesthesia.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.