Article Text

Abstract
Objective The gold standard for the diagnosis of intracranial atherosclerosis remains catheter based digital subtraction angiography (DSA). A symptomatic hemodynamically non-significant intracranial atherosclerotic lesion is described, whose underlying embologenic characteristics were not detectable by either DSA or three-dimensional rotational angiography (3DRA) but fully realized by C-arm cone beam CT (CBCT) angiography.
Clinical presentation A 73-year-old man presented with crescendo transient ischemic attacks consisting of right arm tingling and hand weakness despite long term dual antiplatelet therapy with aspirin and clopidogrel for coronary artery stent. DSA and 3DRA demonstrated a smooth benign appearing left cavernous internal carotid stenosis of <50%.
Intervention Given the incongruence of the lesion with the patient's symptoms and lack of response to aggressive medical treatment, a decision was made to obtain higher resolution imaging. CBCT angiography was obtained with injection at two contrast dilutions, which uncovered an underlying ruptured ulcerated calcific plaque with a small dissective component and overlying thrombus. The lesion was treated with anticoagulation followed by balloon mounted stent angioplasty, with symptom resolution and maintained patency at the 1 year follow-up.
Conclusion The superior spatial resolution and dynamic range characteristics of CBCT angiography provide added clinical utility in disambiguation of questionable intracranial atherosclerotic lesions which may be missed by conventional planar and rotational angiography. The additional information provided by CBCT angiography could be useful in lesion risk stratification and help refine indications for intracranial stent angioplasty given its recent documented shortcomings vis a vis medical management.
Statistics from Altmetric.com
Introduction
Intracranial atherosclerotic disease (ICAD) is associated with a 1 year risk of stroke that varies from 12.2%1 to 25%2 with medical treatment.3 ,4 The gold standard for diagnosis and evaluation of intracranial atherosclerosis has been based on stenosis severity using catheter based digital subtraction angiography (DSA).5 Increasingly, three-dimensional rotational angiography (3DRA) can also assist in the multiplanar volumetric evaluation of intracranial stenoses. More recently, C-arm cone beam CT (CBCT), initially touted for its ability to detect intracerebral hemorrhage during neurointerventional procedures, has gained increasing use in follow-up imaging of intracranial stent therapy6 for aneurysms and other vascular intracranial disease.7 CBCT has demonstrated increasing utility in cross sectional imaging of spinal8 and intracranial vascular malformations.9 Recently, CBCT also was shown to be useful in detecting the fistulous site in a traumatic carotid cavernous fistula.10
Here we describe additional utility of CBCT in the diagnostic workup of a patient with mild hemodynamically non-significant ICAD who had recurrent transient ischemic attacks despite dual antiplatelet therapy and medical optimization. The associated superior spatial resolution and dynamic range of CBCT were critical in establishing an elusive etiologic diagnosis with important clinical implications. Specifically, performance of CBCT angiography with two concentrations of contrast enabled the visualization of the blood compartment and calcific components of the symptomatic non-hemodynamic ICAD lesion, enabling the identification of an ulcerated ruptured plaque which was not detected on either conventional biplane or rotational angiography.
Case report
A 73-year-old, right-handed man presented to his primary care physician with complaints of right upper extremity tingling with decreased sensation and being unable to button his shirt. Admission medications included aspirin and clopidogrel for the treatment of coronary artery disease. The patient recalled an episode of being unable to sign his name a few days prior. He was sent to a local emergency department where symptoms resolved within 30 min of arrival and cardiac and stroke workups demonstrated no etiology for his symptoms. He was transferred to our institution for further workup. Intracranial MR angiography revealed an intracranial left-sided cavernous moderate stenosis which prompted cerebral angiography.
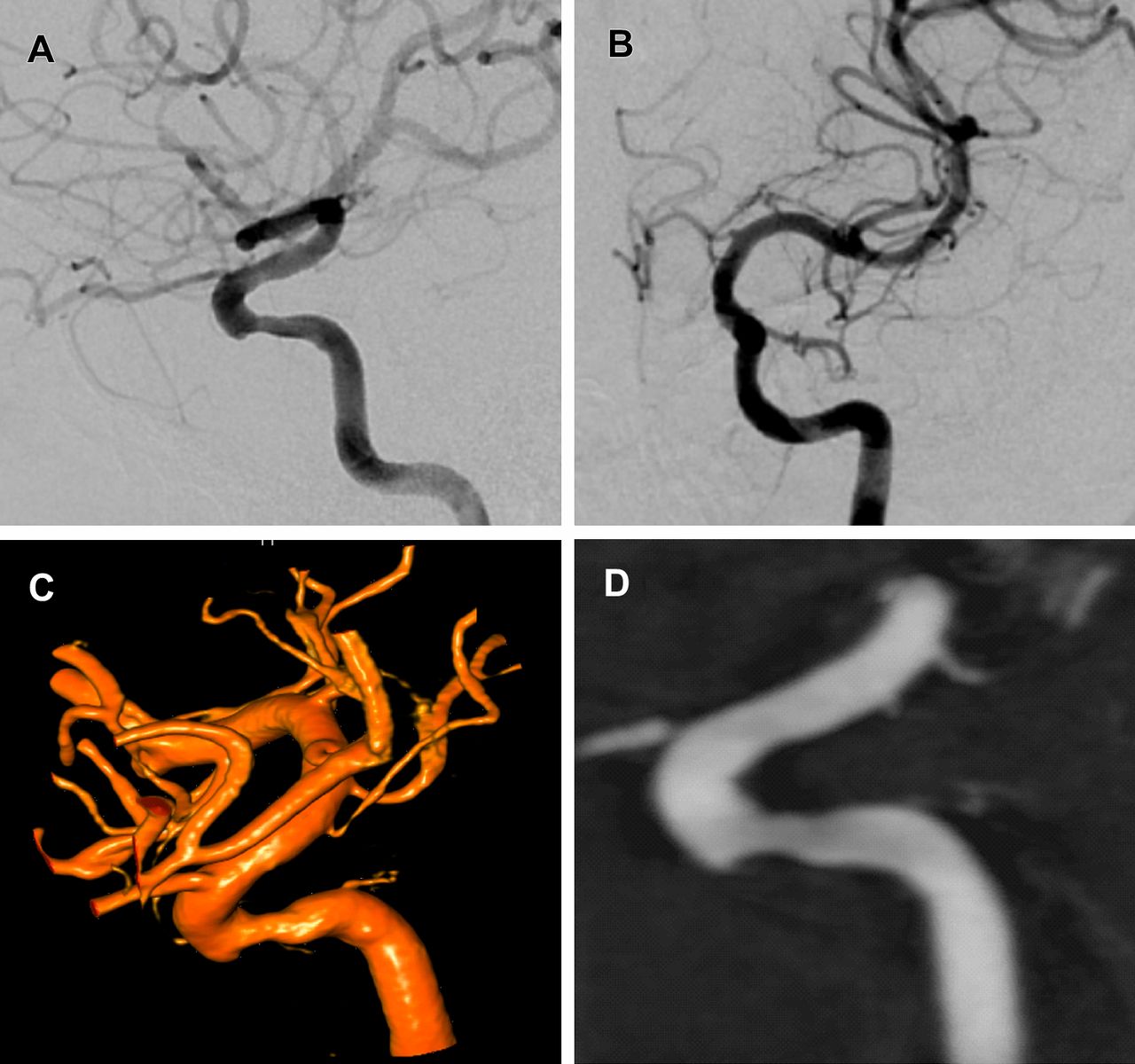
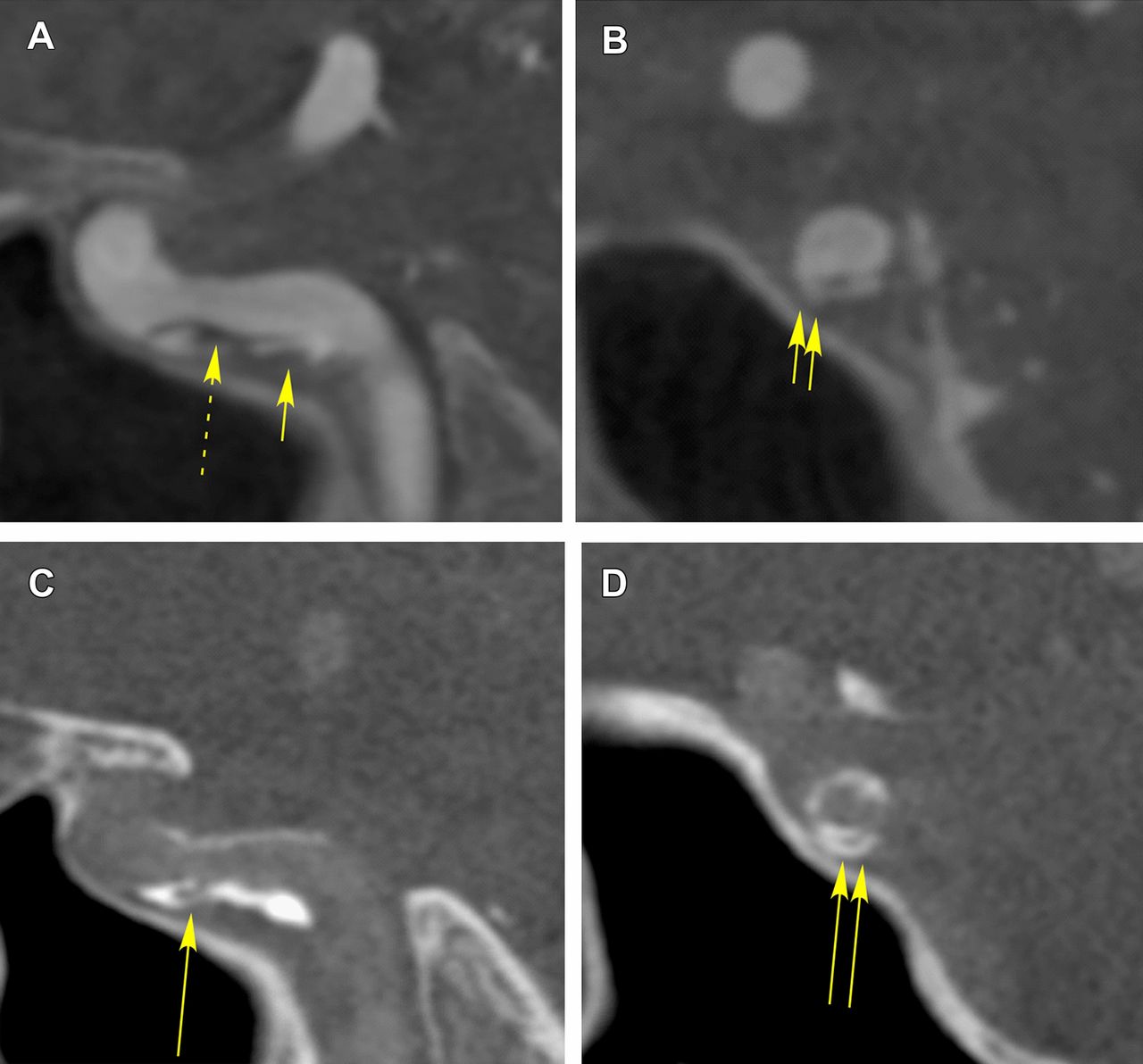
A diagnostic DSA was performed to better evaluate the severity of the stenosis and determine possible endovascular treatment given its lack of response to dual antiplatelet therapy. DSA demonstrated a mild 50% stenosis according to NASCET criteria with a relatively smooth contour and no evidence of flow limitation (figure 1). 3DRA was acquired concomitantly and reconstructed with both volume rendering and multiplanar maximal intensity projection both of which confirmed the moderate degree of stenosis seen on DSA without revealing a filling defect. At this point, the lesion was felt to be not hemodynamically significant enough to correlate to the patient's clinical presentation. In addition, the lesion was smoothly contoured on 3DRA and DSA. However, in light of the multiple recent episodes of transient ischemic attacks, a decision was made to acquire CBCT, with secondary reconstruction over the region of the stenosis (figure 2). CBCT was performed using the standard 20 s acquisition with a flat panel angiography system (Axiom Artis VB22N; Siemens AG, Forchheim, Germany) while injecting 1 ml/s of contrast (Isovue-250; Bracco Imaging SpA, Milano, Italy) during the first acquisition and 1:6 dilute contrast agent mixture with normal saline on a second, with x-ray duration of 22 s and an x-ray delay of 2 s. Dataset reconstruction was performed on the dedicated Leonardo/Syngo workstation. Multiplanar reconstruction imaging of the CBCT volumetric data revealed the presence of multiple embologenic features not seen on the other modalities, including a dissected ruptured plaque with contrast filling in the false lumen as well as an ulcerated focus and overlying thrombus.

Digitally subtracted angiogram of the patient in lateral (A) and anteroposterior (B) projections. Volume rendering of the three-dimensional rotational angiographic reconstructed dataset (C) and corresponding multiplanar reconstruction in the sagittal projection (D) reveal a smooth stenosis of approximately 50% without hemodynamic limiting features and no obvious irregularity.

C-arm cone beam CT (CBCT) angiography performed with injection of 1 ml/s of undiluted contrast (A, B) reveals the presence of an ulcerated ruptured plaque with contrast material entering into an intercalated ulcerating complex of channels seen in both sagittal (A, short arrow) and coronal (B, double short arrows) projections. The black overlying filling defect (broken arrow) represents thrombus overlying the ulcer. CBCT with 1:6 contrast (C, D) reveals the calcified ulcerative complex in sagittal (C, long arrow) and coronal (D, double short arrows) views.
The patient was initially treated with anticoagulation for the overlying thrombus. Given the thrombogenic calcific ulcer and complex appearance of the contrast intercalation within the ruptured ulcerated plaque that led to thrombosis despite dual antiplatelet therapy, a recommendation was made to tack down the ulcer using a balloon mounted stent to insure a smooth wall contour (figure 3). The patient underwent percutaneous transluminal angioplasty and deployment of a 3.5×12 mm Promus stent (Boston Scientific, Natick, Massachusetts, USA), with post-deployment CBCT demonstrating isolation of the ulcerated plaque from the lumen by the stent struts. The patient remained neurologically intact throughout his procedure with resolution of the transient ischemic attacks and returned for follow-up imaging at 3 and 12 months, confirming persistent stent patency without significant stenosis.

{kind=link}
{kind=link}
{kind=link}
Following anticoagulation, the lesion was treated using an over the wire balloon mounted stent angioplasty (A) with resolution of symptoms. C-arm cone beam CT volume rendering (B) and thin multiplanar reconstruction in sagittal (C) and coronal (D) views performed with 1:6 diluted contrast (B) reveals the relative position of the stent struts which now tack down the ulcerated irregular calcific wall (arrowheads) separating from the vessel lumen. Follow-up lateral digital subtracted angiography at 3 months (E) and 1 year (F) shows stable results in the patient who has remained asymptomatic since treatment.
Discussion
The use of CBCT within the neurointerventional suite is growing in acceptance and utility.11 ,12 CBCT has been noted for its higher spatial resolution in several cases,9 ,10 even being capable of assessing the position of stent struts within the lumen of intracranial vessels.6 As an imaging modality, CBCT has also found usefulness in the assessment of in-stent restenosis following treatment of intracranial atherosclerosis.7 ,13
The central finding in this case report is that the imaging acquired from DSA demonstrated a relatively benign appearing lesion while the imaging acquired from the CBCT enabled identification of a complex ulcerated plaque with dissection and overlying thrombus that enabled the determination of the etiology of the patient's symptoms. Given the mild <50% degree of stenosis, the lesion would not have met criteria for ICAD endovascular therapy had CBCT not been acquired. However, the greater spatial resolution of the CBCT enabled detection of the true nature of the lesion, including the overlying thrombus, which would have been missed with reliance on DSA and 3DRA alone in this case. With this understanding, acquisition of high resolution imaging provided by CBCT is recommended in cases where the appearance of the intracranial atherosclerotic lesion does not match the patient's clinical presentation. The information provided by CBCT had a significant beneficial effect on the therapeutic course of intervention and resulted in transient ischemic attack resolution and endovascular treatment. The patient had been on dual antiplatelet therapy for a period of >2 months for prior coronary stent angioplasty, making suboptimal antiplatelet inhibition unlikely as the source of his presenting symptoms. This is further supported by symptom resolution following stent angioplasty despite no change in medical regimen.
Previous work has highlighted the importance of atherosclerotic plaque irregularities and thromboembolism,14 and this may be important in certain cases where the degree of stenosis is not sufficient to be hemodynamically symptomatic. This was confirmed here thanks to the higher resolution of CBCT angiography. The use of two concentrations of dilute contrast enabled the separate characterization of the luminal component, including the filling defect corresponding to overlying thrombus, as well as the architecture of the underlying ruptured calcific ulcer.
In summary, the current case illustrates the utility of CBCT in identifying the fine resolution details of a symptomatic ulcerative intracranial lesion that was not identified on high resolution DSA and rotational angiography. Although a single case, the current report suggests CBCT could play a future role in refining criteria for recommending patients with certain subsets of ICAD for inclusion in medical versus endovascular treatment options given the recent results favoring medical therapy for ICAD.1
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was provided by Tufts Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.