Article Text

Abstract
Background The role of catheter angiography in the diagnosis and management of traumatic cerebrovascular injury has evolved rapidly with advances in CT and MR angiography and continued development of endovascular techniques.
Objective To identify the modern spectrum of traumatic arterial injury encountered during catheter neuroangiography and to examine current patterns of endovascular treatment.
Methods Records of trauma patients undergoing catheter neuroangiography over a 4 year period at two high volume centers were retrospectively reviewed. The sample comprised 100 separate arterial lesions that were classified according to mechanism, location, acuity, and endovascular treatment. Follow-up imaging and clinical notes were reviewed to identify procedural complications.
Results Of 100 arterial lesions, 81% were related to blunt trauma. Distribution of lesions by location was 42% intracranial, 39% cervical, and 19% extracranial. The most common injuries were pseudoaneurysm (38%), fistula (29%), and dissection (19%). In total, 41% of lesions underwent endovascular treatment, with trends favoring treatment of non-acute, penetrating, non-cervical, and high grade lesions. Therapy involved coil embolization for 89% of treated lesions. There were a total of two immediate neurovascular complications and one delayed neurovascular complication; one of these resulted in a permanent neurological deficit.
Conclusions Our experience in a large cohort of patients suggests that a relatively high proportion of traumatic arterial lesions identified by catheter angiography are treated by endovascular means, with a low rate of immediate and delayed neurovascular complications.
- Angiography
- Artery
- Trauma
- Brain
- Neck
Statistics from Altmetric.com
Introduction
Although still considered to be the gold standard for diagnosis of cerebrovascular injury following trauma, catheter angiography has been largely displaced as a screening modality due to increasing utilization of CT angiography (CTA) and MR angiography (MRA) as part of the initial trauma evaluation.1–9 At many institutions, catheter angiography is now used primarily when detailed interrogation of equivocal CTA and MRA findings is warranted or when the possibility of endovascular treatment is being entertained.1 ,2 ,8 ,10–16
In the current era of screening CTA and MRA, the makeup of cerebrovascular injuries that are ultimately identified and evaluated via catheter angiography is not well characterized. In this paper, we report the modern spectrum of post-traumatic craniocervical arterial injury identified at two high volume centers, each with widespread use of CTA and MRA. In addition, we investigate factors that influence the decision to undertake endovascular therapy, the choice of endovascular therapy, and the incidence of treatment related complications.
Methods
In patients with known or suspected traumatic cerebrovascular injury evaluated at each of two high volume metropolitan centers—one a level 1 trauma center and the other an established quaternary referral center—the need for catheter angiography was determined by the interventional neuroradiology service in consultation with neurology, neurosurgery, and/or trauma services. In each case, catheter angiography was preceded by CTA or MRA, performed as part of the initial diagnostic evaluation on the basis of neurological examination, injury mechanism, or imaging findings. Specific indications for screening CTA or MRA were: blunt injury with a Glasgow Coma Scale (GCS) score of <8; skull base fracture involving the carotid canal; cervical spine fracture involving the foramen transversarium, occipital condyle, or C1–C3; greater than 30% subluxation of a vertebral body at or above C5–C6; penetrating head injury with GCS<13; penetrating neck injury; or clinical signs of carotid or vertebral dissection (eg, carotidynia, posterior circulation ischemia). Each patient selected for catheter angiography had abnormal CTA or MRA. Complete diagnostic cerebral angiography was performed in each case by an experienced interventional neuroradiologist, and the decision to pursue endovascular treatment was made in collaboration with the primary service based on standard indications such as lesion severity, radiological progression, or associated symptomatology.
The most recent 4 years of available angiographic data from each institution, spanning 2007–2011 at the trauma center and 2006–2010 at the referral center, were retrospectively reviewed following approval of the local institutional review board. Patients with unknown trauma mechanism were excluded from the study, yielding a total of 52 patients (39 men, mean age 36 years) representing 100 distinct angiographically evident arterial lesions.
Lesions were classified by mechanism of injury (blunt or penetrating), location (intracranial, extracranial, or cervical), acuity (0–14 days, 14–30 days, or >30 days), and endovascular treatment strategy. Lesions were classified as cervical if they involved the common carotid artery, cervical portion of the internal carotid artery, or any of the first three segments of the vertebral artery. Lesions of the external carotid artery or more distal branches, excluding the middle meningeal artery, were considered extracranial. The remaining lesions were considered intracranial. The occurrence of immediate or delayed procedural complications was assessed by comprehensive review of all available neurological imaging and clinical notes from the time of presentation to October 2011. Statistical analysis was performed using Barnard's exact test within the MathWorks MATLAB R2010a software package.17 ,18 A significance level of α=0.050 was considered to be the threshold of statistical significance.
Results
Spectrum of injury
A total of 100 arterial lesions were identified using catheter angiography during the review period. These lesions represented a wide range of post-traumatic arterial injuries (table 1), including pseudoaneurysm (38%), arteriovenous fistula (29%), dissection (19%), transection (9%), occlusion (3%), and thrombosis (2%).
Number (and number treated) of each type of arterial injury
A blunt mechanism of injury (vehicular accident, fall, assault, or crush injury) was responsible for 81% of these lesions, with the remaining 19% of lesions secondary to penetrating trauma. Arterial injury was well represented in all three anatomical compartments—51% of lesions were intracranial, 10% were extracranial, and 39% were cervical in location. Lesions of the posterior circulation accounted for 32% of arterial injuries.
Decision to treat
The overall endovascular treatment rate of all arterial lesions identified by catheter angiography was 41% (table 1). In order to identify factors influencing the decision to pursue endovascular treatment, treatment rate for each type of lesion was subcategorized according to mechanism of injury, acuity, and location.
Endovascular treatment was performed in 37% (30 of 81) of cases of blunt injuries compared with 58% (11 of 19) of penetrating injuries. Although the trend suggested a higher rate of treatment for penetrating lesions, this difference did not attain statistical significance (p=0.070).
The endovascular treatment rate for acute lesions less than 14 days after the date of trauma was 34% (24 of 71), compared with 57% (eight of 14) for subacute lesions between 14 and 30 days old and 60% (nine of 15) for chronic lesions greater than 30 days in age. The difference in treatment rate between acute and non-acute lesions was statistically significant (p=0.012).
Classified by location, the rate of endovascular treatment was 47% (24 of 51) for intracranial lesions, 50% (five of 10) for extracranial lesions, and 31% (12 of 39) for cervical lesions. Although there was a trend towards not treating cervical injuries, the endovascular treatment rate for cervical lesions was not significantly different than for other locations (p=0.070). Similarly, the endovascular treatment rate of 43% for lesions of the anterior circulation was not significantly different than the endovascular treatment rate of 38% for lesions of the posterior circulation (p=0.347).
Propensity to treat also varied by lesion type. The rate of endovascular treatment of arterial dissections was 11% (two of 19), which was significantly lower than for other lesion types (p=0.002). In contrast, the rate of treatment for pseudoaneurysms was 61% (23 of 38), which was significantly higher than for other lesion types (p=0.001). Grouped by Biffl classification, grade I and II injuries (dissection and thrombosis) were significantly less likely to be treated than grade III, IV, and V injuries (pseudoaneurysm, occlusion, and transection) (p=0.00005).
Choice of endovascular treatment
Isolated coil embolization was by far the most common endovascular treatment, being used in 68% (28 of 41) of all treated lesions (table 2). Coils were used in conjunction with stents or particulate embolic agents in an additional eight cases, raising to 89% (36 of 41) the proportion of interventions in which coils were used.
Endovascular treatment of each type of arterial lesion
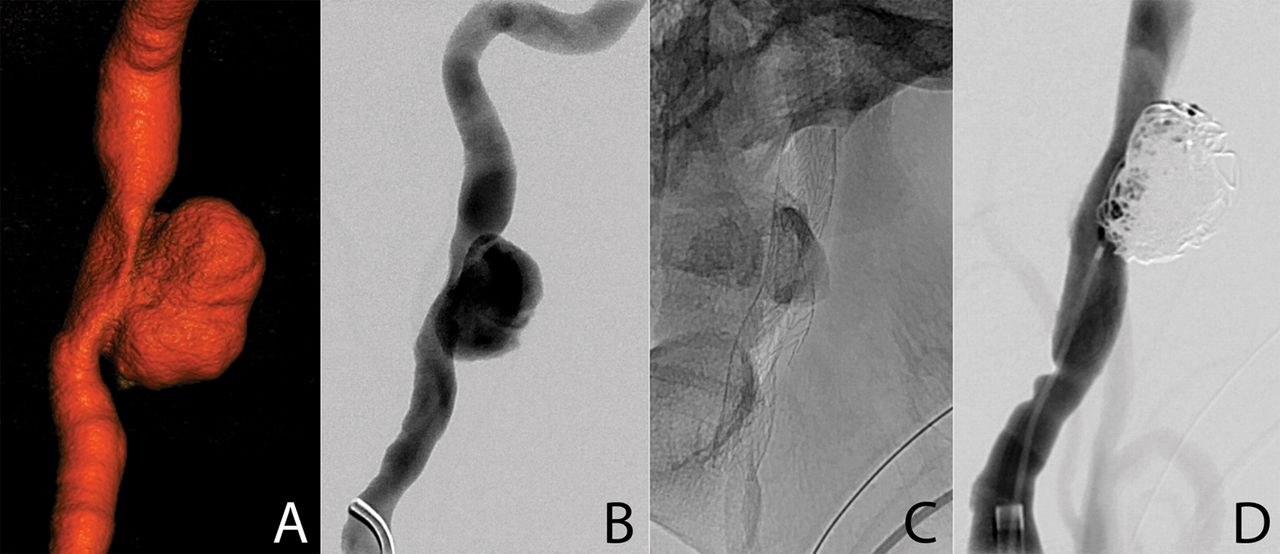
Uncovered stents were used as part of treatment in 20% (eight of 41) of lesions. Stent assisted coil embolization was used to treat five pseudoaneurysms (figure 1), while isolated stent placement was even less common, used to treat only two dissections and one occlusion. No covered stents were used.
{kind=link}
A 37-year-old patient who was referred to our institution with an expanding neck mass 26 days following a motor vehicle collision. Three-dimensional (A) and planar (B) digital subtraction angiography demonstrate a pseudoaneurysm arising from the cervical portion of the internal carotid artery. The patient was treated by stent placement (C) to assist coil embolization (D) of the pseudoaneurysm with parent vessel preservation, followed by initiation of dual antiplatelet therapy with aspirin and clopidogrel. The patient was doing well 6 months after treatment, at which point clopidogrel was discontinued.
The use of particulate and liquid embolic agents was limited to branches of the extracranial carotid artery. Particle embolization with polyvinyl alcohol particles ranging from 350 to 500 μm in size was used in 10% (four of 41) of interventions. Only one of these cases, a pseudoaneurysm of the internal maxillary artery, was treated with isolated particle embolization. Combined coil and particle embolization was used to treat the remaining three lesions, including two arteriovenous fistulas and one pseudoaneurysm, all affecting the middle meningeal artery. A liquid embolic agent (Onyx) was used in only a single case, a pseudoaneurysm of the superficial temporal artery.
Complications and retreatment
In the entire cohort of 52 patients studied with catheter angiography, two (3.9%) immediate neurovascular complications related to the procedure were encountered: one was an iatrogenic dissection of the internal carotid artery requiring endovascular stent placement with no adverse clinical outcome and the other immediate complication was herniation of a coil from a posterior inferior cerebellar artery pseudoaneurysm into the parent vessel itself, resulting in cerebellar infarction with a small but fixed residual deficit.
Of the 41 lesions treated by endovascular means, delayed neurovascular complications related to treatment occurred in one (2.4%) case over a mean period of follow-up of 4.9 months (range 1 day–30 months). This delayed complication arose in a patient who underwent endovascular coiling of a high risk direct carotid–cavernous fistula and presented 47 days after treatment with intraparenchymal hemorrhage in the ipsilateral frontal lobe, likely due to fistula recurrence with drainage into a frontal cortical vein. There were no permanent neurological deficits following resolution of the acute hemorrhage.
Five (12.2%) of the initially treated lesions, including the previously mentioned carotid–cavernous fistula, ultimately required repeat endovascular treatment. All repeat interventions were performed in cases that were initially treated by coil occlusion. Repeat treatment was successful in all five cases, without additional complications or the need for a third treatment in any case.
Discussion
In recent years there has been considerable interest in defining a reasonable screening algorithm to identify post-traumatic craniocervical vascular injuries as early detection and treatment of these lesions has been shown to reduce the incidence of secondary neurological injury.7 ,19 While there is significant disagreement about the optimal screening program,20–22 there has been a consistent trend away from the use of catheter angiography as a primary method of diagnosis and towards CTA and MRA for this purpose. In addition to being non-invasive, CTA and MRA have the advantage of being less time and labor intensive than catheter angiography.
This movement away from diagnostic catheter angiography has been partially offset by the increasing role of angiography in the context of therapy. Endovascular treatment is now indicated in the treatment of a wide range of arterial injuries,2 ,9–14 ,16 ,22–24 and in many cases is the preferred mode of intervention due to the relative safety of catheter angiography.25 Moreover, ongoing development of devices and techniques continue to expand the role of these minimally invasive interventions.
Despite these advances, endovascular intervention may be an unattractive choice in some patients. Contraindications to anticoagulation and antiplatelet therapy in the setting of unresolved multiorgan injury impose an important constraint on the implementation of endovascular therapy.26 The inability to use agents such as heparin and clopidogrel in these patients, combined with the tendency for small acute lesions to heal without intervention, likely accounts for the relatively higher rate of treatment of non-acute and penetrating lesions in our sample. These same contraindications interfere with the use of stents,27 ,28 making endovascular coiling a much more appealing and common treatment option when possible.
In institutions such as ours that routinely use CTA and MRA, patients at low risk for traumatic craniocervical arterial injury or with low grade lesions are less likely to require evaluation with catheter angiography. The spectrum of angiographic lesions we report includes a far lower number of dissections and other low grade lesions than reported in publications preceding the proliferation of CTA and MRA.19 Our data indicating a higher rate of treatment for high grade lesions reflects a growing trend to treat low grade lesions by medical means, typically intravenous anticoagulation or oral antiplatelet administration in suitable patients.24 ,26 ,29 ,30
An important limitation of this study is the limited availability of clinical data, both at the time of presentation and at subsequent follow-up. In particular, patient information at each of the two institutions included in this study was only partially contained in a searchable electronic medical record system, with additional clinical data contained only in paper form that limited assessment of long term neurological outcomes. We instead constrain ourselves to reporting only the rate of complications. Another limitation of this study pertains to an undesirably high rate of patient non-compliance with scheduled clinical, radiographic, and angiographic follow-up. Unfortunately, these problems are not unique to our study but reflect broader factors that particularly affect those patients most susceptible to traumatic injury.
Conclusion
Strategies for diagnosis and treatment of traumatic cerebrovascular injury continue to evolve, particularly with regard to the role of catheter angiography. We have reported the modern spectrum of arterial injuries identified by catheter angiography, defined factors that influence the decision to treat traumatic arterial lesions, and indicated the types of treatments used. Our experience suggests that a relatively high proportion of traumatic arterial lesions identified by catheter angiography are treated by endovascular means, with a low rate of immediate and delayed neurovascular complications.
Acknowledgments
Hugh McSwain, Warren Kim, and Charles Stout participated in the care of the study subjects.
References
Footnotes
-
Contributors APK, RMS, JDE, MRA, and SWH: conception and design. APK, RMS, JDE, CFD, VVH, RTH, and SWH: acquisition of the data. APK: analysis and interpretation of the data. APK and SWH: drafting the article. APK, RMS, JDE, DLC, MRA, CFD, VVH, RTH, and SWH: critically revising the article.
-
Competing interests None.
-
Ethics approval The study was approved by the UCSF Human Research Protections Program.
-
Provenance and peer review Not commissioned; externally peer reviewed.