Article Text

Abstract
Flow diversion for the management of intracranial aneurysms represents a paradigm shift in how aneurysms are managed. The Pipeline embolization device (PED) is, to date, the only flow diverter approved for use in the USA by the Food and Drug Administration. Limitations and complications with new treatment strategies are inevitable, and with the PED there have been reports of complications, most commonly with challenging deployments. Once deployment has been initiated, the device is ‘one-way’; it can only be deployed further or removed. Yet, situations arise in which the ability to recapture or reposition the device would be advantageous. A second-generation Pipeline has been developed that addresses these concerns. We report the first use in North America of this second-generation Pipeline device: the Pipeline Flex. We discuss our rationale for using the device, our impressions of its operation, and the relevant literature concerning the current state of flow diversion.
- Aneurysm
- Device
- Flow Diverter
Statistics from Altmetric.com
Background
We report the first use in North America of the Pipeline Flex in a woman presenting with an unruptured symptomatic large posterior inferior cerebellar artery (PICA) aneurysm.
Case presentation
A 49-year-old woman with no significant medical history experienced acute onset of severe headache. The investigation was negative for subarachnoid hemorrhage but identified a PICA aneurysm (figures 1 and 2). Her symptomatology appeared to represent a sentinel hemorrhage and she reported a family history of aneurysm rupture. Numerous treatment options were considered, including microsurgery, but we felt that she would benefit from the Pipeline Flex device. We received a compassionate use exemption from the institutional review board of the University of Tennessee and the Food and Drug Administration (FDA) and enrolled the patient in a pilot study using a vascular replicator to rehearse her procedure.
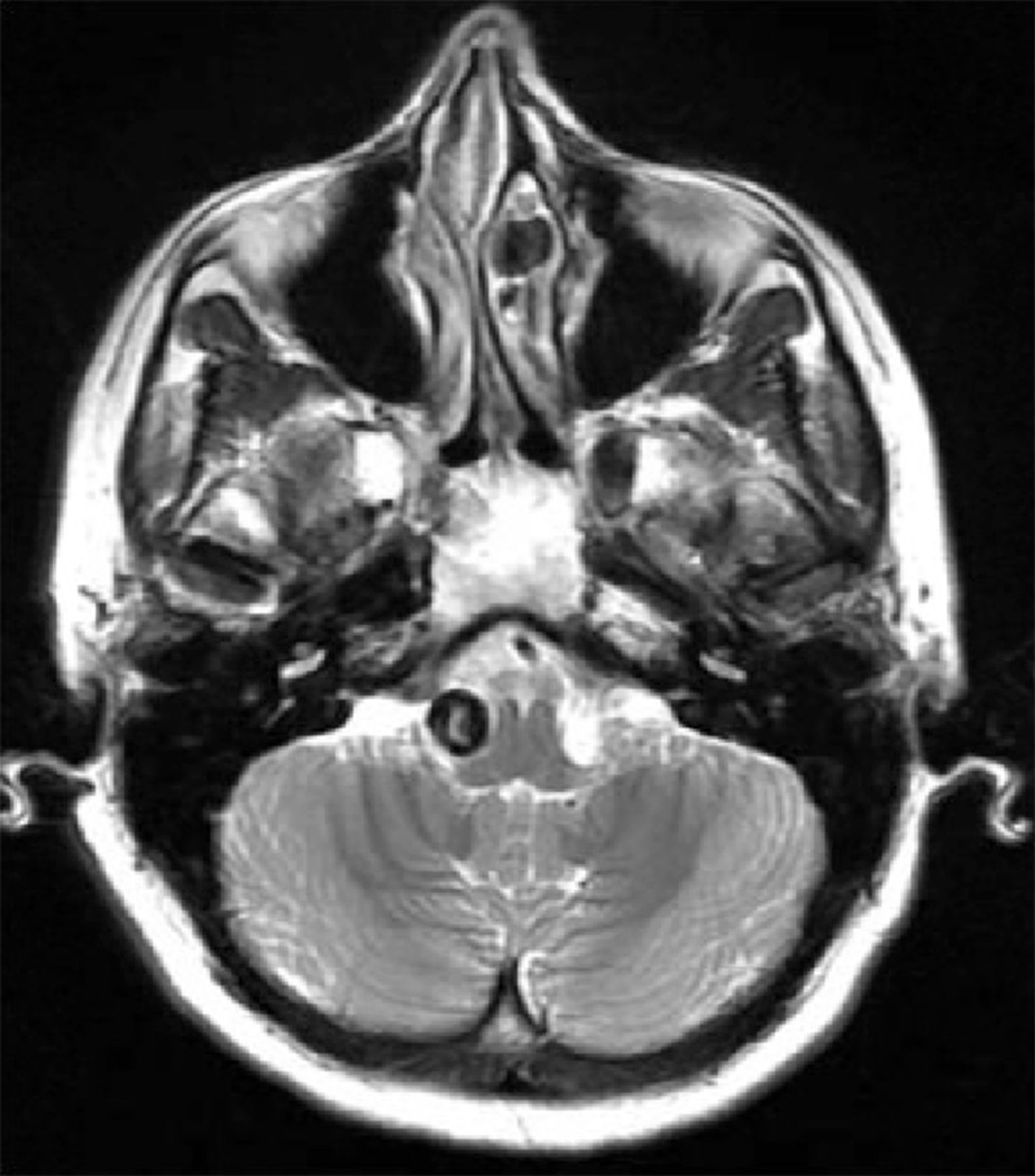
MRI showing vascular mass in the region of the posterior inferior cerebellar artery.

Initial angiogram in posteroanterior (A), lateral (B), and three-dimensional (C) projections. Characteristics noted were the close proximity of the posterior inferior cerebellar artery to the proximal neck of the aneurysm as well as the acute angle of the vertebral artery at the level of the aneurysm.
Treatment
In our patient the Pipeline Flex alone could have been considered, but cases of disastrous early aneurysm ruptures have been reported, especially for large and giant aneurysms treated with flow diversion alone.1–4 We therefore used both coils and a flow diverter due to the size of the aneurysm and symptomatic presentation, which would leave the patient more vulnerable to rupture. The ability to recapture and redeploy a flow diverter was felt to be critical because it would allow precise deployment in a position to protect the origin of the PICA while building a coil mass in the aneurysm.
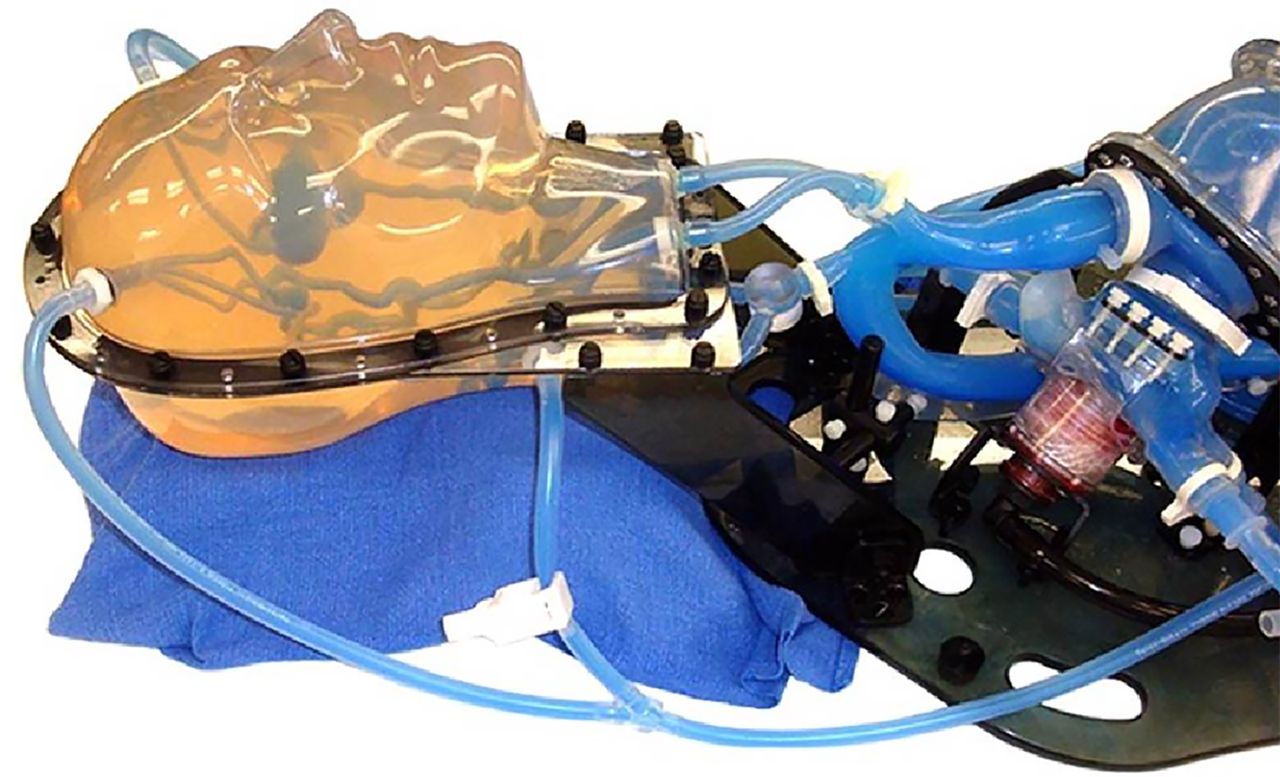
We rehearsed the procedure on a patient-specific Replicator system model (Vascular Simulations, Stony Brook, New York, USA) of the patient's cervical and cerebral vasculature (figure 3). The rehearsal confirmed our concerns about the difficulty of accessing the vertebral artery distal to the aneurysm; an ‘around the dome’ technique was required to gain microwire access to the distal parent artery.

Replicator system model used by the authors to rehearse the patient's specific procedure.
Loaded with dual antiplatelet medications and systemically heparinized, the microwire and microcatheter were positioned uneventfully. We then began flow diverter deployment. Our experience with the Replicator showed that this device could be deployed with more of an unsheathing maneuver compared with the pushing maneuver commonly associated with first-generation Pipeline embolization devices (PEDs). We deployed a third of the device and pulled the catheter and device proximally into position. We sought to create more metal coverage at the proximal neck of the aneurysm. A greater emphasis on pushing instead of unsheathing in the vicinity of the aneurysm neck allowed us to increase the density of the flow diverter. However, there was more foreshortening than anticipated so we resheathed the device and reattempted our compression maneuver. This second attempt was successful and we finished deployment of the initial framing coil (figure 4). We then deployed four additional coils with special attention directed towards avoiding encroachment of the coils at the origin of the PICA.
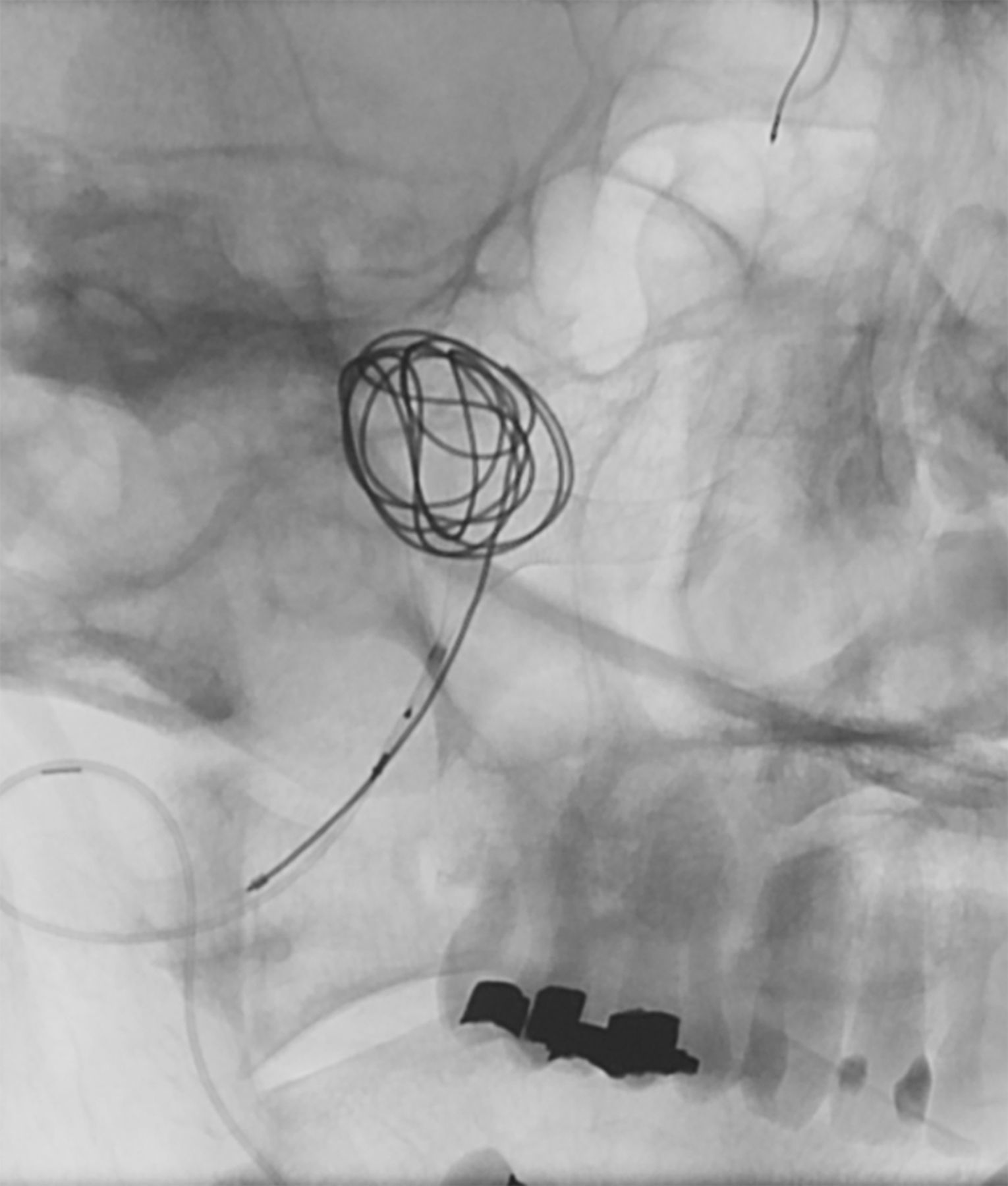
Unsubtracted working angle view of flow diverter in adequate position (about 75% open) prior to final deployment of the initial framing coil.
With a moderate coil packing achieved, the Flex was completely unsheathed. Immediate images demonstrated brisk filling and full patency of the PICA and progressive—albeit incomplete—occlusion of the aneurysm (figure 5). Cone beam CT angiography demonstrated excellent apposition of the device to the inner and outer curves of the vertebral artery, patency of the PICA, and no untoward findings (figure 6).
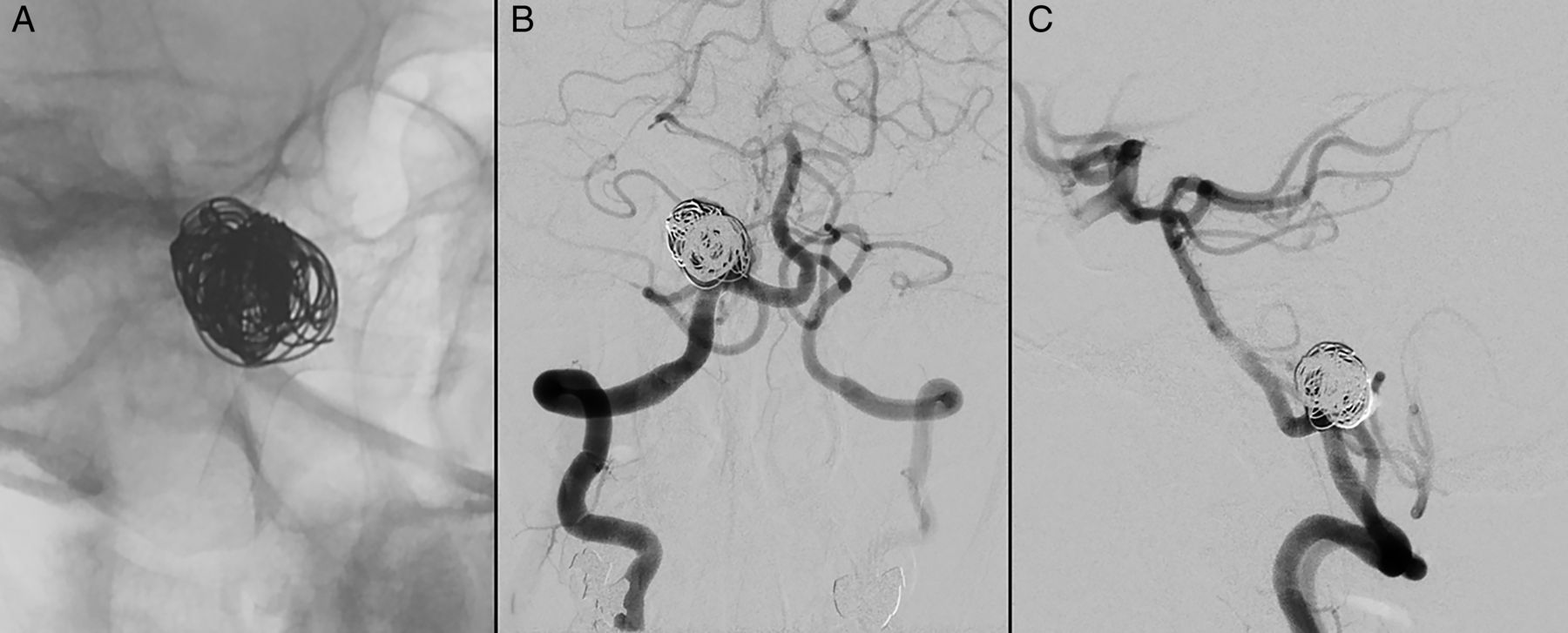
Unsubtracted (A) and subtracted (B and C) oblique views showing progressive, albeit incomplete, thrombosis of the aneurysm.

20-second rotational cone-beam CT angiogram demonstrating good apposition of the Pipeline Flex within the vertebral artery and patency of the posterior inferior cerebellar artery.
Outcome and follow-up
The patient reported intermittent headaches post-procedure, which were controlled with non-steroidal anti-inflammatory drugs. On follow-up, she was neurologically stable and returned to work within 2 weeks. Three months after the procedure we performed a follow-up cerebral angiogram which demonstrated almost complete thrombosis of the aneurysm and full patency of the Pipeline Flex embolization device (figure 7). A 1 mm neck residual proximate to the origin of the PICA was observed (figure 8). The patient remains on dual antiplatelet medication and will undergo another angiogram in 3 months’ time; discontinuation of the clopidogrel will be considered then.
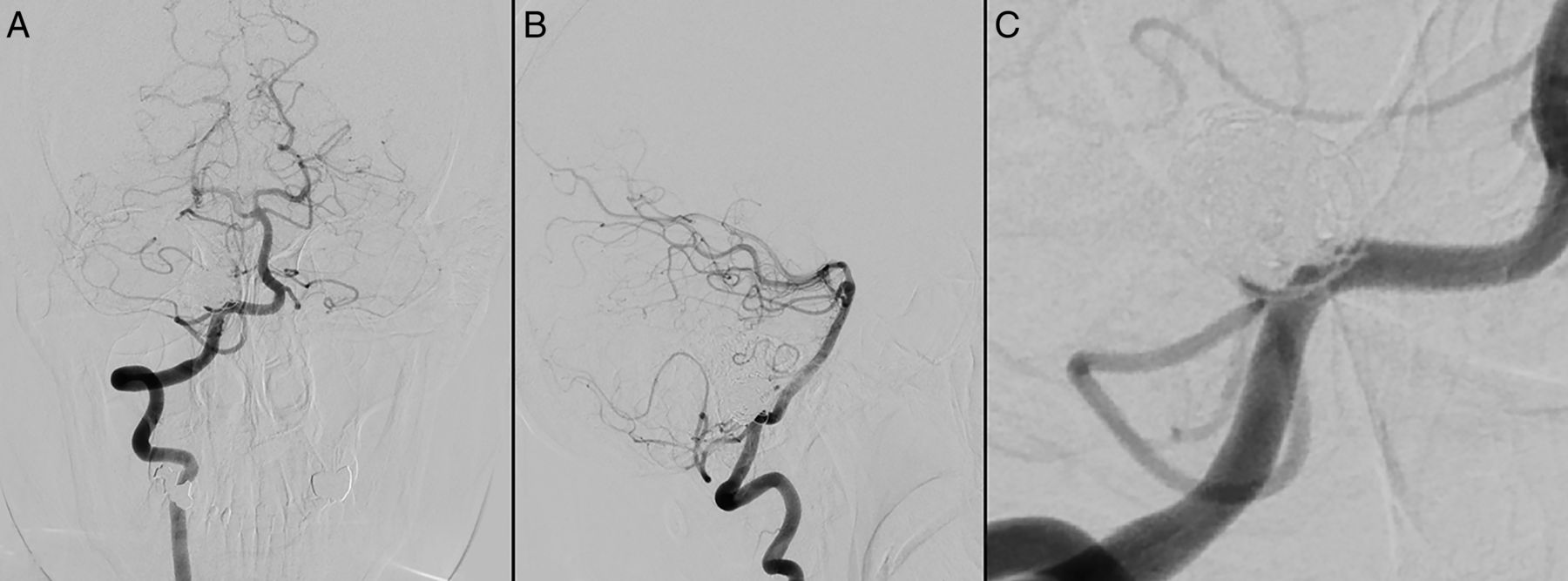
Posteroanterior (A), lateral (B), and oblique (C) angiograms at 3 months follow-up demonstrating minimal residual filling of the aneurysm and full patency of the vertebral and posterior inferior cerebellar arteries.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Dual-volume three-dimensional view angiogram at 3 months follow-up showing slight residual filling of the inferior portion of the dome of the aneurysm.
Discussion
As aneurysm treatment shifts toward minimally invasive approaches, increasingly complex aneurysms are treated endovascularly. However, simple coil embolization for wide-necked aneurysms can result in a higher rate of aneurysm recurrence.5 Early aneurysm rupture—especially large and giant aneurysms treated with flow diversion alone—is a dreaded complication.1–4
PEDs for large or giant wide-necked intracranial aneurysms have been shown to be successful in treating wide-necked intracranial aneurysms.2 ,4–6 Nevertheless, complications such as incomplete obliteration, early postoperative aneurysm rupture, thromboembolism, and intraparenchymal hemorrhage have been reported.1 ,4 ,7 ,8
A criticism of flow diversion has been deployment of the device, with reports of inconsistent deployment, misplacement, stent narrowing, and other difficulties related to device delivery. Based on these experiences, expectations have been high for a second-generation device with a more fool-proof delivery. In our patient, it was important to have the flow diverter form over the origin of the PICA, which took more than one try (as we expected). The one-way nature of the first-generation PED would not allow resheathing and repositioning. More importantly, reports exist in the literature regarding difficulties with deployment of the PED, especially with tortuous anatomy and longer devices, as in our case.6
The second-generation Pipeline Flex uses the same implant as the first-generation device but differs with respect to the delivery system. The distal detachment mechanism was redesigned and the new deployment mechanism depends on unsheathing two constraining flaps which flip 180° once the distal end of the implant is released, allowing for complete resheathing of the device. The resheathability of the redesigned distal detachment mechanism is the second advancement of the Pipeline Flex. The original Pipeline requires a process known colloquially as ‘corking’ in order to salvage an unfavorable deployment, a process that requires removal and wasting of the expensive implant (a technique with its own attendant risks). In our case, this feature allowed us to tailor the amount of ‘bunching’ of the PED over the origin of the PICA in order to realize our goals for deployment.
The final major way in which the newer device differs is with regard to the new pusher wire, which is stiffer and allows for easier navigability of tortuous intracranial curves and loops. Based on our single initial experience, the Flex allowed for more flexibility in repositioning a device deployment, a less problematic deployment, and safer bailout techniques in cases of unfavorable deployment.
Key messages
Many consider flow diversion to be a ‘game changer’ in endovascular treatment of intracranial aneurysms.
Our initial single case experience with the Pipeline Flex highlights several refinements made to the only currently FDA-approved flow diverter available in North America.
This second generation of flow diverters may represent an incremental but substantial advancement on this paradigm shift in our approach to intracranial aneurysm treatment.
Acknowledgments
The authors wish to thank Andrew J Gienapp for technical and copy editing, preparation of the manuscript and figures for publishing, and publication assistance with this manuscript.
Footnotes
Republished with permission from BMJ Case Reports Published 30 January 2015; doi: 10.1136/bcr-2014-011548
Competing interests DH has served as a consultant for Covidien. CJM has served as a consultant for Covidien Neurovascular and Codman Neurovascular. ASA served as a consultant for Covidien, Johnson and Johnson, Siemens, Stryker, and Terumo and received grants from Siemens and Terumo.
Patient consent Obtained.
Ethics approval Ethics approval was obtained from the UTHSC Institutional Review Board (#14-03293-EU).
Provenance and peer review Not commissioned; externally peer reviewed.