Article Text

Abstract
Background Numerous large randomized trials have shown a significant morbidity and mortality benefit with the transradial approach (TRA) over the transfemoral approach (TFA) for endovascular procedures. However, this technique is routinely avoided or aborted due to unfamiliarity with the technique and the associated anatomical difficulties that may be faced in this approach. The objective of this review is to identify both the common and uncommon challenges that may be encountered during a transradial approach for cerebrovascular catheterization and to provide tips and tricks to overcome the transradial learning curve.
Method A careful review of the literature and of all our transradial cases was carried out to identify the common challenges and complications that are encountered when using TRA for diagnostic cerebral angiography and neurointerventions.
Results A stepwise approach is provided to prevent and manage common challenges including radial artery access failure, radial artery spasm, radial artery anomalies and tortuosity, radial artery occlusion, radial artery perforation and hematoma, subclavian tortuosity and anomalies, and catheter knots and kinks.
Conclusion The ability to recognize and navigate anatomical variations and complications unique to TRA will accelerate learning, decrease unnecessary morbidity and mortality, and further advance the neurovascular field.
- angiography
- technique
- artery
- catheter
- complication
Statistics from Altmetric.com
Introduction
The transradial approach (TRA) has been widely adopted for coronary, peripheral, and cerebrovascular endovascular procedures due to the overwhelming evidence demonstrating a reduction in access site complications, in addition to improved patient preference and cost compared with traditional transfemoral access (TFA).1–9 Led by the interventional cardiology community, large randomized multicenter trials such as the Radial versus Femoral Access for Coronary Angiography and Intervention in Patients with Acute Coronary Syndrome (RIVAL) and Minimizing Adverse Haemorrhagic Events by Transradial Access Site and the Systemic Implementation of AngioX (MATRIX) studies, with over 7000 patients each, have reported a greater than 60% reduction in vascular complications as well as significant decreases in all-cause mortality and net adverse clinical events with TRA.10 11 Further well-described advantages of TRA include immediate ambulation as opposed to bed rest after femoral procedures, reduced post-procedure nursing care, reduced hospital stay—and therefore cost—with an overwhelming patient preference for transradial angiography.12
However, TRA comes with a significant learning curve similar to any new surgical technique. A study of 942 new radial operators for percutaneous coronary intervention found a threshold of 30–50 cases at which time improvements in procedural metrics began to flatten.13 14 Our center has undergone an extensive exploration into transitioning our practice from TFA to TRA for the majority of our procedures.15–19 While we encountered many challenges common to all radialists, we also encountered challenges specific to TRA for neurointervention that have not been previously explored in the literature.
We sought to report here on the totality of challenges and complications that one can expect to encounter when transitioning to the radial approach for neurointervention. This includes the access of the radial artery itself and also challenges relating to performing the full range of neurointerventional procedures via TRA. In this review we provide a stepwise description of complications and challenges that may be encountered during TRA for neurointervention with a focus on prevention and management.
Radial artery access failure
For interventionalists who have used the femoral artery for the vast majority of their training and practice, TRA represents a significant change in the size of the artery to be cannulated. There is no question that it is more challenging to catheterize. Failure to access the radial artery is typically due to puncture error or radial artery spasm (RAS). These two reasons for failure are intimately linked as failed attempts at piercing the radial artery quickly result in RAS, which in turn results in even greater difficulty in accurately puncturing and cannulating the small artery in spasm.
During our initial experience with TRA, access times were considerably longer than TFA, spasm was frequent, and conversion to femoral access was not uncommon. However, two specific changes to our practice essentially eliminated radial access failures. The first was adoption of the double wall puncture technique. Bernat et al found that the double wall technique was significantly faster and more likely to successfully cannulate the artery after a first-pass attempt compared with the single wall puncture technique.20
The second change was the universal use of ultrasound to guide cannulation of the radial artery. The routine use of ultrasound for radial artery puncture nearly eliminates access failure and improves efficiency. In a randomized multicenter trial of 692 patients, ultrasound guidance resulted in a significantly reduced number of attempts (mean 1.65±1.2 vs 3.05±3.4, p<0.0001) and time to access (88±78 s vs 108±112 s, p=0.006), as well as improved first-pass success (64.8% vs 43.9%, p<0.0001).21 This reduction in attempts is important in decreasing the likelihood of RAS as well as preventing patient pain, swelling, and hematomas at the access site.
Of note, when radial artery access failure occurs distally, attempts to cannulate the radial artery more proximally can be done prior to conversion to TFA. The entire length of the radial artery distal to the brachioradialis muscle (in which the artery dives below the fascia) is easily accessed and associated with minimal risk.
Radial artery spasm (RAS)
While RAS most commonly occurs at the beginning of the case precluding access, it may also manifest later in the procedure as forearm pain or resistance while manipulating the catheter. This is more commonly seen with large-bore catheters and repetitive manipulations of the guide catheter, resulting in friction on the radial artery endothelium. While rates of up to 30% have been reported for RAS, various strategies can be employed to significantly reduce this.
First, adequate sedation is paramount. In a randomized study of 2013 patients, Deftereous et al reported a threefold decrease in the risk of spasm in patients who received pre-procedural opioid and benzodiazepine compared with those who did not (2.6% vs 8.3%, p<0.001).22 The high vasospastic potential of the radial artery is due to its muscular media and high density of alpha-adrenergic receptors. Catecholamine release from pain and anxiety can lead to contraction of the artery, resulting in difficulty with accurate puncture and subsequent cannulation with the sheath and catheter. Thus, in our center, all patients undergoing awake diagnostic cerebral angiography via TRA receive conscious sedation with midazolam and fentanyl prior to puncture. We also apply topical 2.5% lidocaine/prilocaine cream to the radial artery area in the wrist and forearm, covered by an adhesive for 15–30 min prior to the start of the procedure, followed by subcutaneous injection of approximately 2 mL 1% lidocaine without epinephrine.
Second, in order to prevent RAS with catheter introduction, for all TRA cases we infuse prophylactic vasodilators after placement of the vascular sheath. A meta-analysis found that the combination of verapamil (2.5 mg) with nitroglycerin (200 μg) had the lowest rates of RAS.23 Additionally, the use of a longer vascular sheath (25 cm vs 10 cm) may be useful in preventing repetitive friction along the radial artery, as does the use of hydrophilic coated sheaths. Finally, preoperative planning with appropriate selection of catheter systems can minimize catheter exchanges and manipulation, thus reducing the risk of RAS.
If RAS is encountered later during the case, the first maneuver is administration of more antispasmolytics (nitroglycerin and verapamil) through the guide or the sheath if there is sufficient space. In addition, increased sedation can assist dramatically as previously mentioned. In extreme cases, if the patient is awake and the catheter becomes impossible to remove due to RAS, general anesthesia can be employed. Additional techniques to combat RAS include: warm compresses that cause vasodilation, ulnar artery compression that results in compensatory radial artery dilatation, and subcutaneous injection of local spasmolytic into the periarterial space.24
There have been rare case reports of severe spasm resulting in catheter entrapment, where retraction of the catheter becomes very difficult. Forceful rapid retraction of the catheter in this scenario will result in worsening spasm and has been reported to cause external intussusception of the artery and even radial artery rupture.25 In our experience, very slow and steady withdrawal of the catheter in combination with the abovementioned maneuvers will typically resolve catheter entrapment. However, last resort invasive techniques include regional nerve blocks and surgical endardarectomy for removal of entrapped catheters.
Finally, patient selection should always be considered. Patients of short stature, low body mass indices, young age, and small wrist circumferences should be identified preoperatively as carrying a higher risk of small radial artery diameters as well as RAS.26 Operators should be aware of sheath diameters and match sheath size and radial artery size to avoid spasm, occlusion, and pain.27 28
Radial artery anomalies and tortuosity
Navigation of the catheter through the radial artery into the brachial artery is usually straightforward, but operators can encounter anatomical variants or anomalies that can complicate the navigation. In a large study of 1540 patients undergoing transradial coronary procedures, radial artery anatomical anomalies such as high-bifurcation radial origins, full radial loops, and radial tortuosity were relatively common, occurring in 13.8% of patients. Patients with these anatomical variants had a higher rate of procedural failure than those who did not (14.2% vs 0.9% in non-anomalous radial arteries).29
A high-bifurcating radial origin is defined as bifurcation of the brachial artery into the radial and ulnar arteries proximal to the intercondylar line of the humerus, a fixed line representing the proximal border of the antecubital fossa (figure 1). This variant is associated with a slightly higher procedural failure rate due to a longer length of the smaller diameter radial artery that can contribute to RAS. In the setting of a high bifurcation, a longer vascular sheath may be considered or ulnar access depending on the size of the radial artery and the desired case to be performed.
Radial artery anatomical variant: high radial bifurcation.
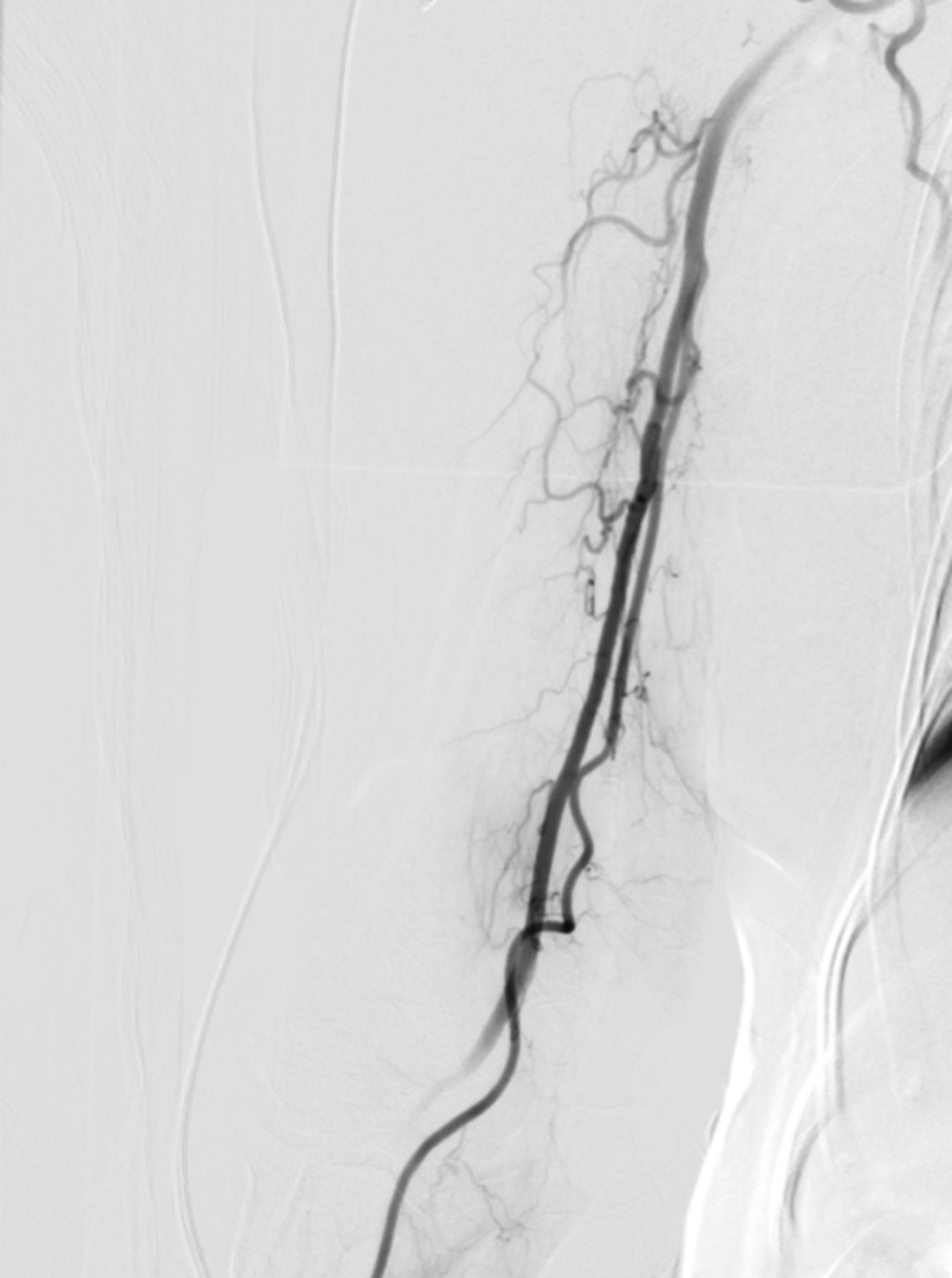
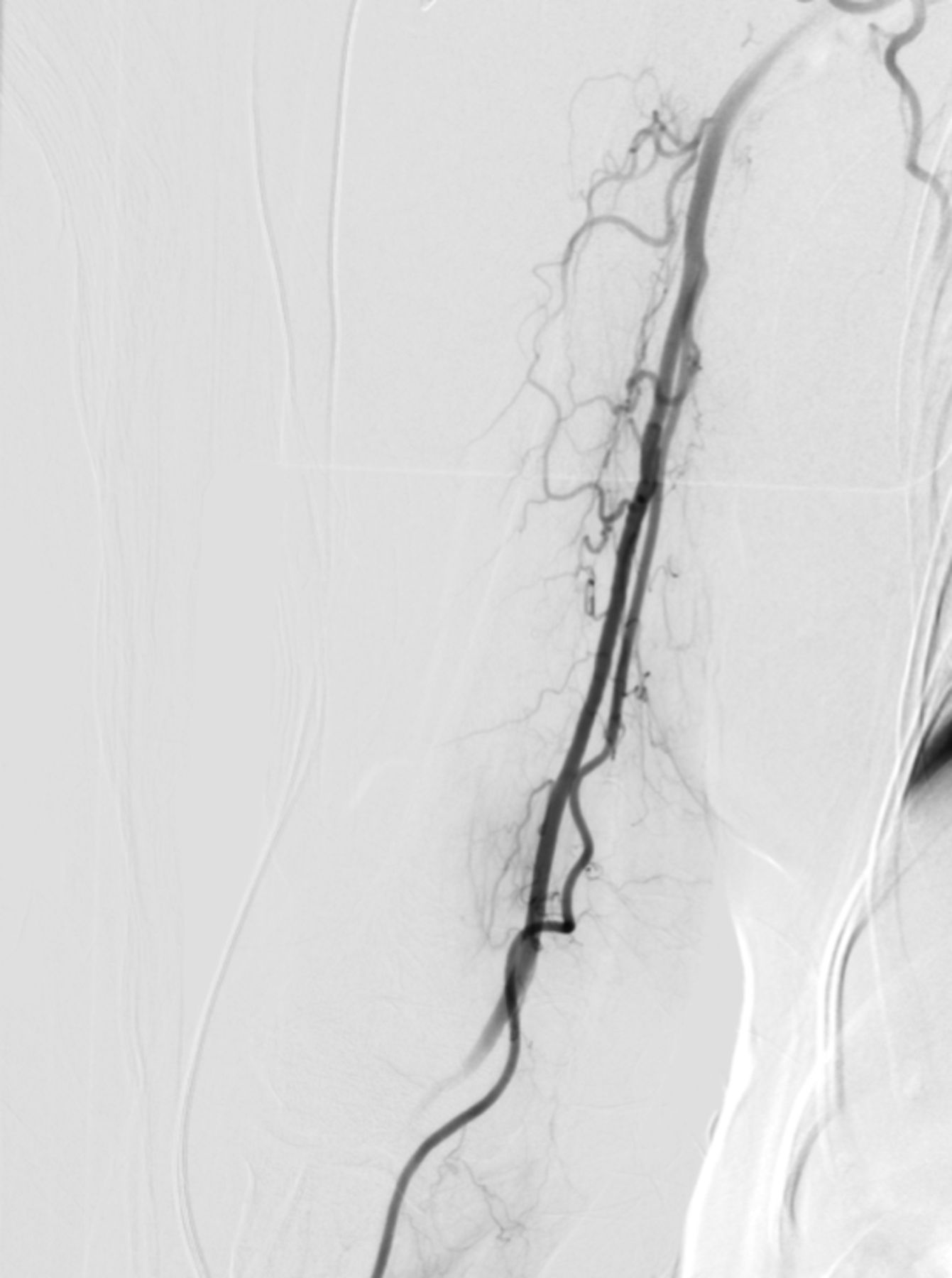
Radial artery loops are a significant challenge that generally require reduction of the loop in order to complete the procedure transradially. A radial artery loop consists of a 360° retrograde bend of the radial artery before joining the ulnar artery in the forearm. Further complicating this tortuosity is the frequent finding of the recurrent radial artery branch at the apex of the loop (figure 2).29 The loop tends to deflect straight tipped wires into this small side branch, which runs parallel to the brachial artery. Without proper identification on a radial artery angiogram and selection of the brachial artery, the patient is at risk of spasm, perforation, or even avulsion of the recurrent branch. Thus, for the routine use of radial artery angiograms and roadmaps, we advocate identifying radial artery tortuosity prior to wire passage. A recent study found that routine preprocedural radial artery angiography is associated with a lower rate of access site bleeding complications, reduced overall procedural time, and TRA crossover rate.30
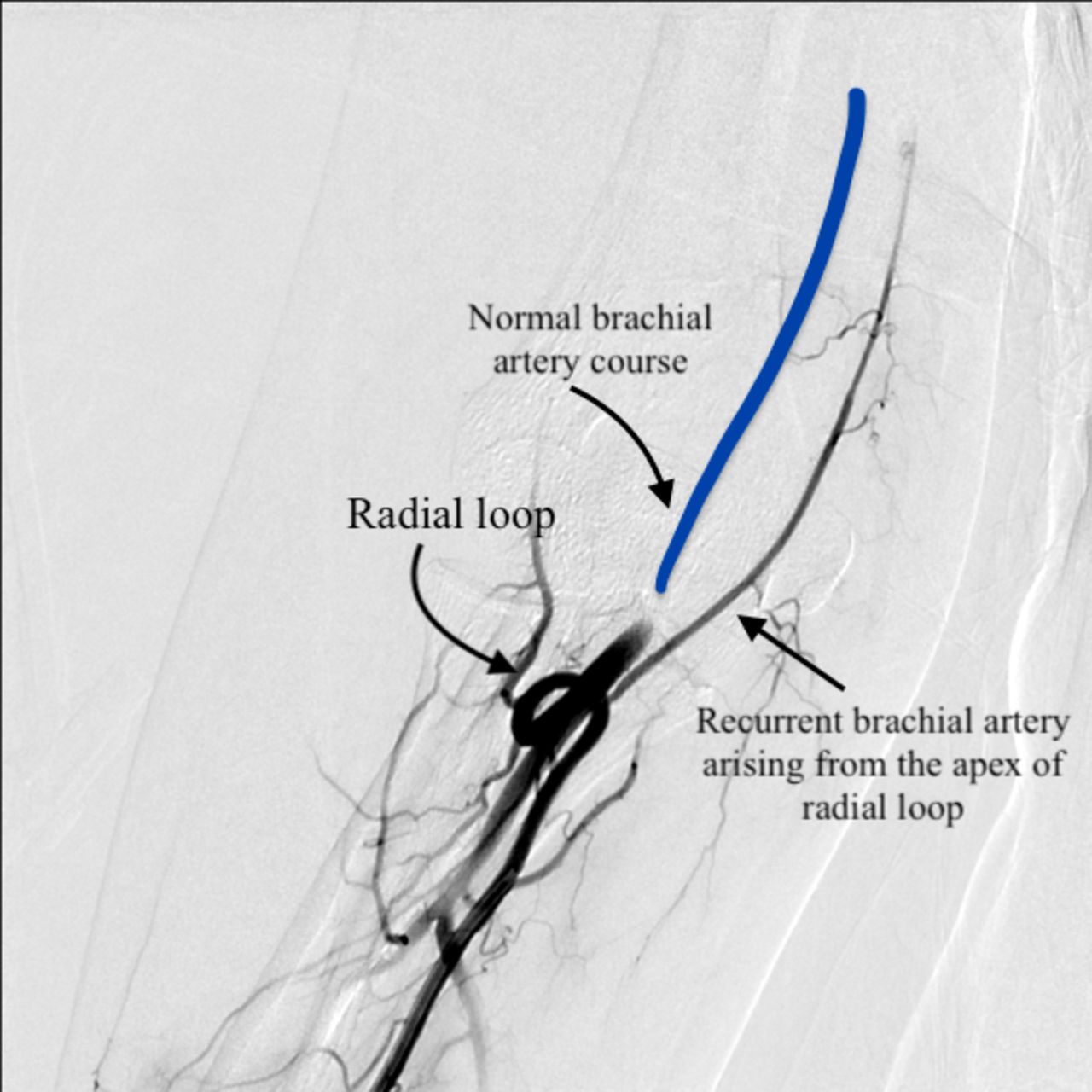
Radial artery anatomical variant: radial artery loop with recurrent radial artery arising from the apex of the loop.
There are many techniques for navigating radial loops and tortuosity. Often, just advancing a soft-tipped 0.035 inch hydrophilic guidewire or 0.014 inch microwire in the radial artery will straighten it out. However, another useful method is the balloon-assist tracking technique (BAT).29 The diagnostic catheter or guide catheter is loaded with a standard non-compliant balloon, which is positioned slightly protruding beyond the tip of the catheter over a microwire. Inflation of the balloon subsequently eliminates the ledge effect of the catheter and facilitates wire and catheter passage around the loop or tortuosity.31 32 Another useful technique if the artery cannot be navigated with a 035 glidewire is to place an SV8 018 wire inside a 027 microcatheter inside the diagnostic catheter. Once the SV8 is sufficiently distal, it provides enough support to track the diagnostic catheter around the loop. Once the catheter tip is sufficiently around the loop, the SV8 and 027 microcatheter can be removed and the 035 glidewire introduced. Distal position of the 035 wire in the brachial and even subclavian artery will allow enough support for the diagnostic system to track and the loop to reduce. Operators must remember that attempts to straighten a 360° loop, however, are often associated with patient discomfort and greater radiation exposure and contrast volume.33
Radial artery perforation and hematoma
While extremely rare with a reported incidence of only 0.1%, radial artery perforation can occur from forceful pushing of the guidewire into radial artery side branches. This complication needs to be identified and managed immediately as it can result in forearm hematomas and even a forearm compartment syndrome. Abandoning the procedure and applying immediate hemostatic compression over the perforated area is the preferred approach of most operators. However, some experienced radial operators advocate continuing the procedure by carefully advancing the catheter past the perforation site, thus using the catheter as an internal hemostatic device and sealing the perforated segment by the time the procedure is completed.24 34
While arteriovenous fistula and pseudoaneurysm formation are more commonly associated with TFA, rare case reports of radial arteriovenous fistulas and pseudoaneurysms have been reported after TRA procedures. The natural history of these iatrogenic radial arteriovenous fistulas and pseudoaneurysms is benign and they tend to resolve spontaneously. Initial management involves bandage compression and arm elevation for 12–24 hours, which typically results in complete resolution. Persistent or symptomatic pseudoaneurysms or fistulas should be referred to vascular surgery.35
Radial artery occlusion
The most frequent complication of radial procedures is radial artery occlusion (RAO), with a reported incidence of 1–6%. RAO is almost always asymptomatic due to the ulnar–palmar collateral vascular blood supply of the hand. However, persistent RAO precludes the use of radial artery access in any future interventions. Procedural duration, sheath size, compression time and pressure all have been shown to be risk factors for RAO.36 Saito et al showed that the incidence of RAO increased from 4% to 13% if the radial artery internal diameter to sheath outer diameter ratio was <1.0 compared with >1.07.27
However, one of the advantages of TRA is the superficial location, which allows for safe and effective patent hemostasis. The technique of patent hemostasis has been found to significantly reduce RAO at 30 days and should be standard practice.37 This method consists of applying compression to both the radial and ulnar arteries and observing the disappearance of the plethysmography signal. The radial artery compression is slowly released until the return of the plethysmographic signal or bleeding is noted. We maintain this pressure in the transradial band for 30 min, at which time air is released and the access site is monitored for any bleeding.
Prophylactic procedural heparin has also been shown to significantly reduce rates of RAO, with a linear relationship observed between heparin dose and rate of RAO.38 Most commonly, 5000 IU heparin or 70 IU/kg is administered intra-arterially via the radial sheath or intravenously, with no difference in RAO whether given intra-arterially or intravenously.39
More recent data show that the addition of prophylactic simultaneous ipsilateral ulnar artery compression reduces RAO. In a randomized controlled trial of 3000 patients undergoing diagnostic angiography with 5F sheaths, ulnar compression reduced 30-day RAO from 3.0% to 0.9% compared with maintenance of patent hemostasis (MOPH) alone (p=0.0001), without evidence of hand ischemia.40 In another randomized controlled trial of 240 patients undergoing diagnostic or interventional procedures with 6F sheaths, ipsilateral ulnar compression reduced RAO from 5% to 0% compared with MOPH alone (p=0.01).41
Subclavian tortuosity and anomalies
Severe subclavian-innominate artery tortuosity is present in approximately 6–10% of patients.42 Severe tortuosity of the right subclavian artery is associated with difficulty catheterizing the great vessels due to a loss of translational force around the turns of the loops and the lack of specifically designed transradial cerebral catheters. This can result in prolonged manipulation of the catheter, increased radiation, as well as increased risk of thromboembolism, catheter kinking, and vessel dissection (figure 3). In many cases the right subclavian artery can be negotiated with deep inspiration, leftwards rotation of the head, and upward chin tilt.43 A standard 0.035 inch guidewire may straighten out the loop; however, it should be noted by the operator that significantly more support will be required to navigate a system into the cerebrovasculature and catheter length will be shorter than anticipated. Additional techniques to navigate the loop and advance a large system include introducing a parallel wire (0.014 inch) and BAT. In cases of subclavian tortuosity during diagnostic cerebral angiography, we prefer to use a 5F Terumo Simmons 1 catheter (Terumo, Somerset, New Jersey, USA), which can be easily formed and tracked and is less prone to knotting or kinking. While the Simmons 1 tail is sometimes too short to catheterize the left vertebral artery, adequate left vertebral artery angiography can almost always be obtained with a Simmons 1 catheter by timing the inflation of a sphygmomanometer cuff on the left arm with contrast injection in the proximal left subclavian artery.

Oblique view of the aortic arch showing a patient with severe right subclavian tortuosity which presented a significant challenge including kinking of 088 guide catheter while catheterizing the left internal carotid artery.
Arteria lusoria is a congenital aberrancy of the right subclavian artery wherein the right subclavian artery originates separately from the aortic arch as the fourth branch distal to the left subclavian artery. Repeated entry of the guidewire and the catheter in the descending aorta should raise the suspicion for the presence of arteria lusoria. In our experience, only the left and right vertebral arteries can be catheterized in the case of arteria lusoria. Angiography of the carotid arteries will likely require transition to TFA.
In the presence of proximal left common carotid tortuosity or steep angulation of the left common carotid artery origin, navigation of the Simmons catheter in the left internal carotid artery can be difficult as the system is prone to herniate in the aortic arch. This difficulty can be overcome by different techniques including using a stiffer glidewire or by slowly and repeatedly balancing wire advancement and catheter advancement.16 19
Catheter kinks and knots
Simmons shaped catheters are used to select the great vessels during TRA procedures with a contrast ‘puffing’ technique. However, without the guidewire, the Simmons shape has the potential to form a hinge point that can predispose to kinking or knotting with catheter manipulation, particularly in cases of a tortuous subclavian artery. Kinks typically occur with counterclockwise rotation when trying to engage the right common carotid artery. Refraining from rotating the catheter more than 180° to prevent build-up of torque proximally that is not transmitted to the catheter tip can prevent knotting.44
When dealing with a kink or a knot in the catheter, a stepwise approach should be tried starting with simple methods. First, attempt to insert the guidewire and advance to the catheter tip to straighten the catheter kink. However, this is not effective for complete knotting and carries a theoretical hazard of perforating the catheter or blood vessel. A second strategy is to try to untwist the catheter with clockwise or counterclockwise rotations in the opposite direction to the initial torque while simultaneously advancing a hydrophilic guidewire. Third, application of external fixation over the catheter by inflating a sphygmomanometer cuff to above 200 mm Hg can allow more effective untwisting.45
If these methods fail, encasing the knot with a larger sheath is possible. The proximal portion of the kinked catheter is cut outside the skin with a scalpel or scissors and the original vascular sheath is retracted over the cut catheter. A long sheath is then advanced over the cut catheter, while holding the latter steady, until the kink is reached. It is important to use a long sheath and to advance the sheath to the knot and not to pull the knot toward the wrist, which will eliminate other options such as distal extraction with snaring if this technique fails. Under fluoroscopy, advance the long sheath to the kink and then gently pull the kinked catheter back, unraveling the kink, until the catheter can be completely withdrawn into the sheath.46
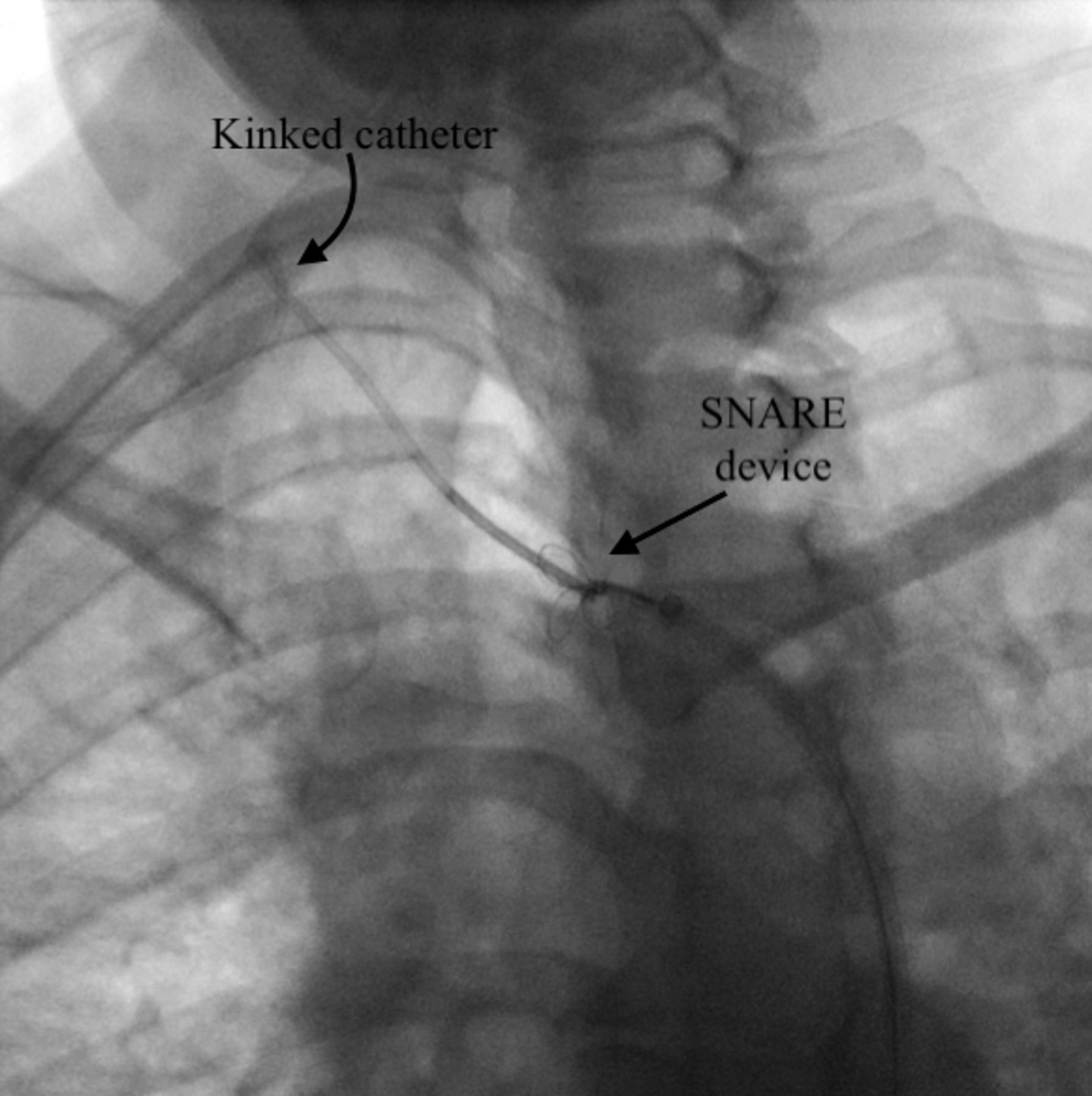
Finally, capturing the kinked/knotted catheter from a femoral approach is another useful maneuver. If all other methods fail, it is very important not to pull the catheter toward the wrist into the radial artery as the kink/knot can damage the artery and make it much harder to snare the catheter in the smaller radial artery. Instead, keep the catheter tip in the axillary or subclavian artery. Obtain femoral access with a 6F shuttle sheath and advance it to the beginning of the descending aorta. Then use an appropriately sized Amplatz GooseNeck Snare (ev3) through the shuttle to capture the distal end of the kinked catheter. When the distal end of the catheter is secured in the Snare, the proximal end is cut at the wrist and the catheter is pulled inside the shuttle from the femoral access (figure 4).46 47
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Snaring technique of a kinked Simmons 2 catheter via a femoral approach.
Conclusion
The feasibility and safety of TRA for cerebrovascular angiography and intervention has led to increasing adoption of this technique by neurointerventionalists. However, complications and perceived barriers may cause new operators to abandon this approach. An ability to recognize and navigate anatomical variations and complications unique to TRA will accelerate learning, decrease unnecessary morbidity and mortality, and further advance the neurovascular field.
References
Footnotes
Contributors M-CB, SHC, ECP: Substantial contributions to the conception or design of the work and the acquisition, analysis, and interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ECP: Stryker Neurovascular: Consultant; Penumbra: Consultant; RIST Neurovascular: Stockholder; Medtronic Neurovascular: Consultant; Cerenovus: Consultant.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.