Article Text

Abstract
Background Currently, there are no large-scale studies in the neurointerventional literature comparing safety between transradial (TRA) and transfemoral (TFA) approaches for flow diversion procedures. This study aims to assess complication rates in a large multicenter registry for TRA versus TFA flow diversion.
Methods We retrospectively analyzed flow diversion cases for cerebral aneurysms from 14 institutions from 2010 to 2019. Pooled analysis of proportions was calculated using weighted analysis with 95% CI to account for results from multiple centers. Access site complication rate and overall complication rate were compared between the two approaches.
Results A total of 2,285 patients who underwent flow diversion were analyzed, with 134 (5.86%) treated with TRA and 2151 (94.14%) via TFA. The two groups shared similar patient and aneurysm characteristics. Crossover from TRA to TFA was documented in 12 (8.63%) patients. There were no access site complications in the TRA group. There was a significantly higher access site complication rate in the TFA cohort as compared with TRA (2.48%, 95% CI 2.40% to 2.57%, vs 0%; p=0.039). One death resulted from a femoral access site complication. The overall complications rate was also higher in the TFA group (9.02%, 95% CI 8.15% to 9.89%) compared with the TRA group (3.73%, 95% CI 3.13% to 4.28%; p=0.035).
Conclusion TRA may be a safer approach for flow diversion to treat cerebral aneurysms at a wide range of locations. Both access site complication rate and overall complication rate were lower for TRA flow diversion compared with TFA in this large series.
- aneurysm
- intervention
- flow diverter
- complication
- artery
Statistics from Altmetric.com
Introduction
The transradial approach (TRA) is increasingly utilized for access in neurointerventional procedures. Due to its superficial location, the radial artery is easily compressible, which ameliorates the risk of access site complications. Within the cardiology literature, large randomized trials have shown lower morbidity and mortality as well as higher patient preference and cost reduction associated with TRA.1–9 However, there have been only a very limited number of studies in the neurointerventional literature directly comparing complications rates.10–12 Reducing access site complications is particularly relevant to flow diversion for two reasons. First, flow diversion employs larger bore access systems, which may increase the likelihood of access arterial injury, bleeding or occlusion.13 14 Second, prolonged dual antiplatelet therapy (DAPT) is administered to patients undergoing endovascular flow diversion along with heparin, which increases the risk of access site bleeding. Additionally, the smaller diameter of the radial artery raises the question of whether a TRA approach is uniformly feasible for flow diverting procedures.
A limited number of case reports and series have reported the feasibility of flow diversion treatment via TRA, but large scale studies are necessary to compare the performance of TRA with the transfemoral approach (TFA) for flow diversion procedures.15–19 The present study aims to assess complication rates associated with TRA versus TFA flow diversion in a large, multicenter database derived from 14 centers.
Methods
Ethics approval
Each participating center obtained individual institutional review board approval for this study. Consent was waived due to the retrospective nature of the study.
Data collection
Participating centers included: Baylor College of Medicine, Baptist Memorial Hospital Memphis, Geisinger Health System, Thomas Jefferson University, Methodist University Hospital Memphis, Medical University of South Carolina, Mayo Clinic Rochester, Tulane University, University of Arizona, University of Miami, University of Virginia, University of Washington, Wake Forest University, and Washington University in St Louis. Each of the 14 participating centers retrospectively reviewed medical records of patients treated for cerebral aneurysms with flow diversion from 2010 to 2019. Collected data included patient demographics, comorbidities, clinical presentation, location and characteristics of the aneurysms, DAPT administration, arterial access site, coil usage, and procedure related complications. De-identified data from each center were pooled together and screened for errors. Uncertainties or ambiguities in the data were addressed by the contributing center. A total of 2311 patients who underwent flow diversion were analyzed. Twenty-six patients were excluded because they had incomplete records. Not of these patients were treated via a TRA and none had any complications. Final analysis included 2,885 patients of which 134 (5.86%) were treated with TRA and 2151 (94.14%) via TFA.Arterial access sites included TRA and TFA. The primary endpoint of this study was access site complications as reported by participating sites. The secondary endpoint of this study was all procedure-related complications.
Endovascular procedure
The choice of access approach was determined by the attending neurointerventionalist at each participating site based on operator expertise and patient-specific considerations. While several centers have begun to transition to a radial first paradigm due to the improved safety profile, additional patient factors that favor TRA include posterior circulation aneurysms, bovine/type II/III aortic arches, large body habitus, previous iliac stenting/bypass, and femoral artery occlusion. Reasons for exclusion often include patients with Raynaud’s syndrome, arteriovenous fistulas of the upper extremity, and reflex sympathetic dystrophy of the upper extremity.
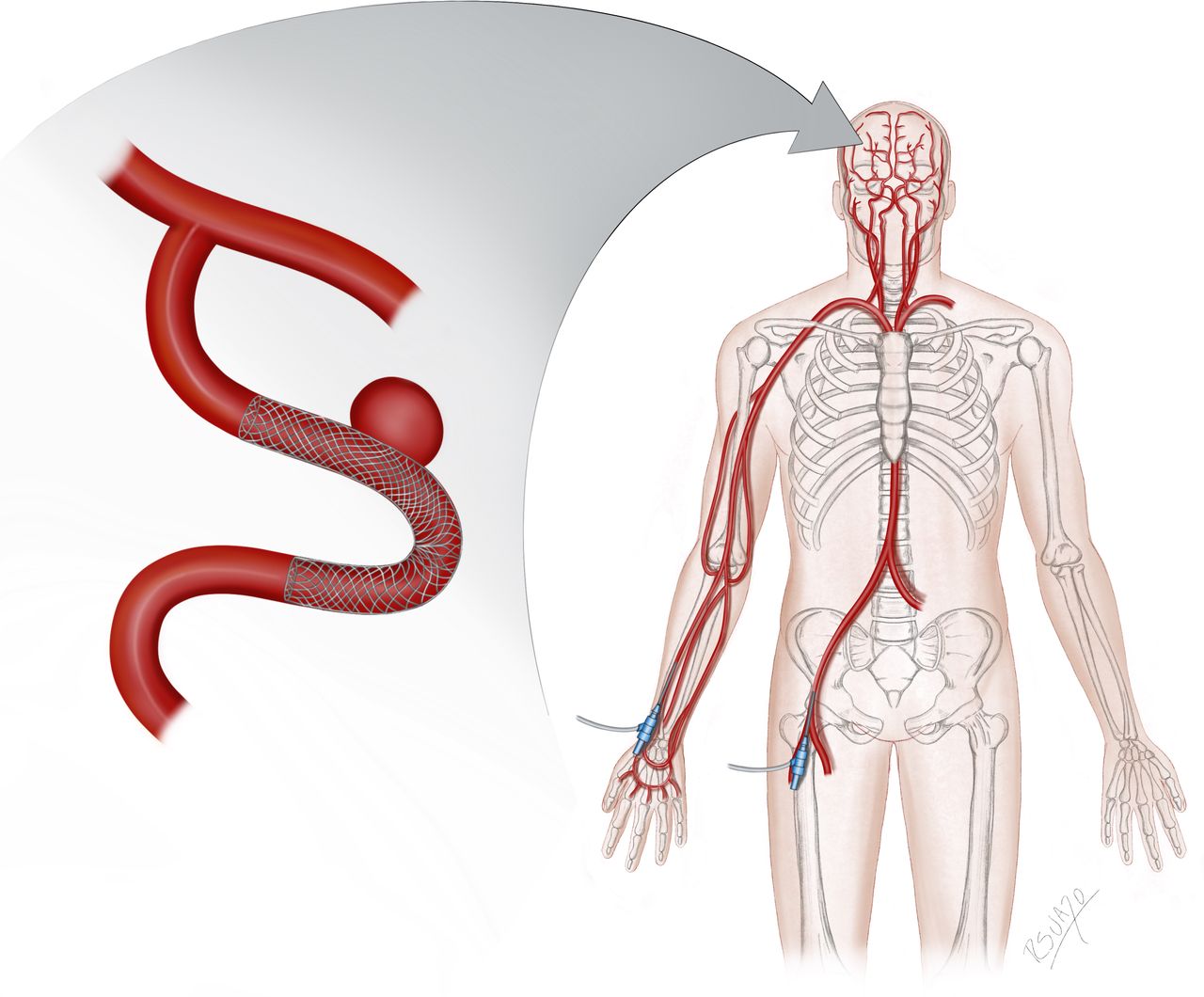
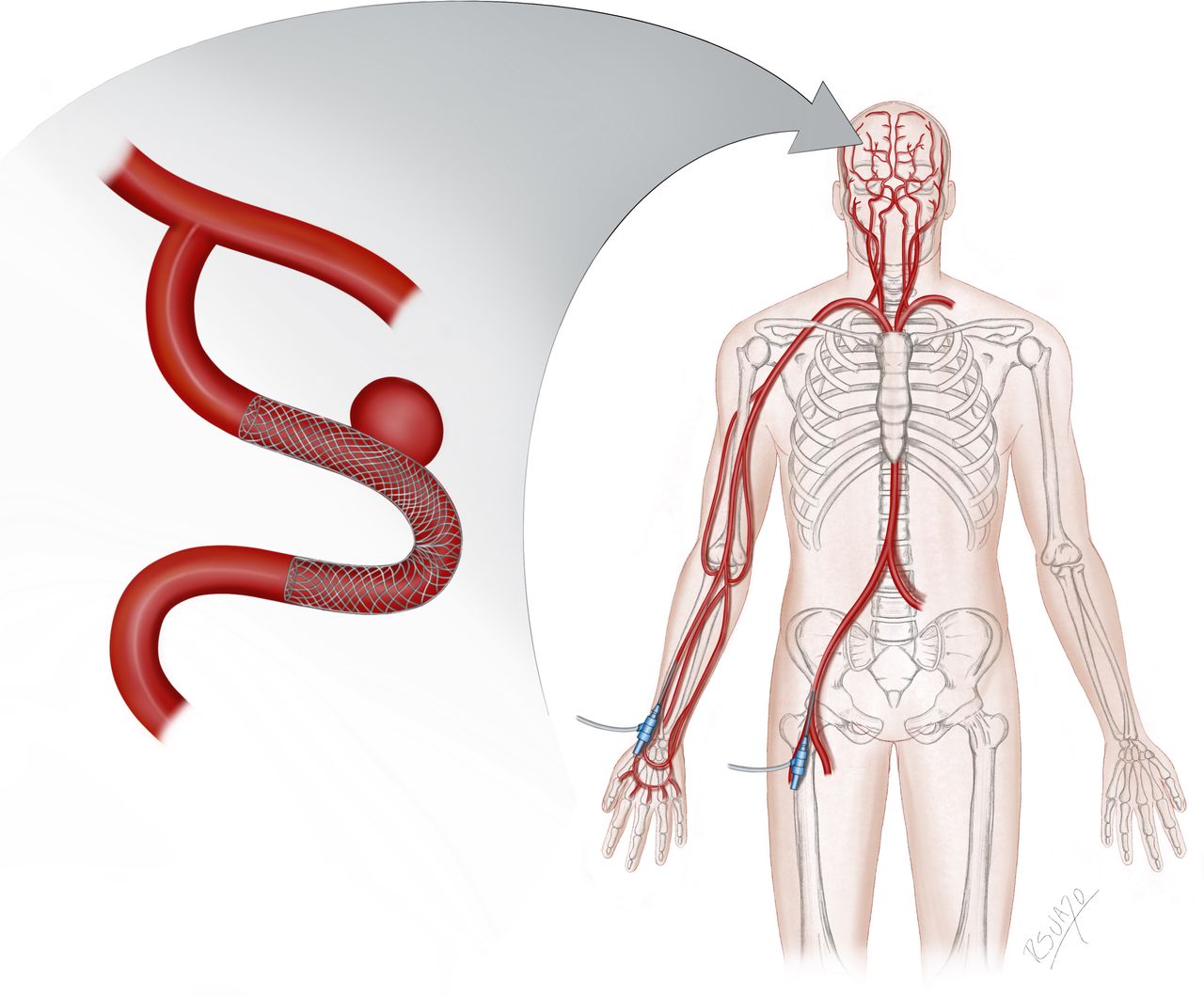
Endovascular sheaths, catheters and wires were selected at provider discretion under institutional protocol. The technical details of TRA flow diversion have been described previously.14 18 Briefly, radial access was obtained under ultrasound guidance from the proximal radial artery (2–3 cm proximal to the palmar wrist crease) or distal radial artery (anatomical snuffbox). After placing the introducer sheath, spasmolytic drugs were given via the sheath to reduce radial artery vasospasm. Activated clotting time was maintained between 250 and 350 with intravenous heparin to prevent radial artery occlusion. A variety of bi-axial or tri-axial catheter systems can be employed for flow diverting stent placement. Typically for radial artery diameters >2.5 mm, a tri-axial system was used with the radial sheath exchanged for a 0.088 inch guide catheter. For radial arteries <2.5 mm, bi-axial or tri-axial systems using a 0.070–0.071 inch guide catheter with a 6 French (6F) slender radial sheath in place or a sheathless system with a 0.070–0.072 inch guide catheter were used. The majority of the cases included in this study used the Pipeline Embolization Device (Covidien Neurovascular, Irvine, CA) for flow diversion; a small number used the Surpass Flow Diverter (Stryker Neurovascular, Fremont, CA). Figure 1 illustrates endovascular access via TRA and TFA for flow diverting stent placement.
{kind=link}
Endovascular access via transradial (TRA) and transfemoral (TFA) approaches for flow diverting stent placement.
Statistical analysis
Data are presented as mean and range with standard deviation for continuous variables, and as frequency and percentages for categorical variables. Pooled analysis rates were calculated for patient, aneurysm and treatment characteristics. Pooled analysis of proportions was calculated using weighted analysis with 95% CI to account for results from multiple centers. P values ≤0.05 were considered statistically significant. Statistical analysis was carried out with Stata 14.0 (College Station, TX) and SAS 9.4 (Cary, NC).
Results
A total of 2285 patients were treated for cerebral aneurysms with endovascular flow diverting stents at the participating centers during the 10 year study period; 1871 patients were female (80.96%) and the mean age was 56±14 years (table 1). In the overall cohort, 914 patients (41.62%) had a history of aneurysm rupture. Before flow diversion, 392 patients (19.54%) had received at least one other treatment such as coiling, clipping or previous flow diversion. The most common aneurysm location was the ophthalmic artery branching point of the internal carotid artery (ICA, 29.79%), followed by cavernous ICA (14.00%), posterior communicating artery (13.41%), paraclinoid ICA (11.48%), and superior hypophyseal artery (11.35%); 1717 aneurysms (74.30%) were saccular and 263 (11.38%) were fusiform. A summary of patient and aneurysm characteristics as well as procedure details is provided in table 1. The pipeline embolization device (Medtronic Neurovascular, Irvine CA) was used in 2292 patients (99.18%), and the surpass flow diverter (Stryker Neurovascular, Fremont, CA) was used in 19 patients (0.82%). DAPT was administered in 99.54% of the patients (table 1).
Summary of patient/aneurysm characteristics and procedure details (n=2311; percentage in parentheses)
Endovascular access was via TRA in 134 patients (5.86%) and TFA in 2151 patients (94.14%). The two groups shared similar demographic composition, comorbidities and clinical presentation, as well as aneurysm characteristics (table 1). For TRA flow diversion procedures, a 5F sheath was used for access in 2.56% of the patients, a 6F sheath in 62.39% patients, a 7F sheath in 11.97% patients, and a sheathless system with a 0.088 inch guide catheter was used in 23.08% patients. Crossover from TRA to TFA was documented in 12 (8.63%) patients due to radial artery spasm, vessel tortuosity or inadequate support.
A complication rate of 8.61% was observed in the total cohort (199 of 2311 patients). This included 53 access site complications, 46 bleeding events (1.99%; subarachnoid hemorrhage, intracerebral hematoma or subdural hematoma), 25 strokes with permanent deficit (1.08%), 47 strokes with temporary deficit or unspecified temporality (2.03%), 11 silent infarcts (0.48%), five new cranial nerve deficits (0.22%), and 29 other complications (1.25%, table 2).
Details of complications in overall cohort and by access type (percentage in parentheses)
Access site complications were more common during femoral access, occurring in 53 of 2151 cases (2.48%, 95% CI 2.40% to 2.57%) versus 0 of 134 for radial access (0%, p=0.039). There were four (0.19%) femoral arterial occlusions, 35 (1.63%) superficial hematomas/pseudoaneurysms, 13 (0.60%) retroperitoneal hematomas, and one (0.05%) arteriovenous fistula, with six (0.28%) patients requiring blood transfusion (table 3). There was one death resulting from a femoral access site complication. The overall complications rate was also higher in the TFA group (9.02%, 95% CI 8.15% to 9.89%) compared with the TRA group (3.73%, 95% CI 3.13% to 4.28%; p=0.035). Details of complications stratified by access type are summarized in table 2. A higher overall complication rate continued to be observed in the TFA group compared with TRA in the subgroup of procedures performed from 2016 to 2019 (p=0.031). Between the time periods 2010–2015 and 2016–2019 (corresponding pre-radial and radial eras in this study), there was no significant change in the femoral overall complication rate. There was also no significant trend in femoral overall complication rate by year.
TFA access site complication breakdown
Discussion
In this multicenter study, we compared the safety of TRA versus TFA flow diversion and demonstrated a lower access site (p=0.039) and overall complication rate (p=0.035) of TRA for flow diversion. This is the largest series to date comparing TRA with TFA for this type of neuroendovascular procedure.
The access site complication rate was 0% in the TRA flow diversion group and 2.48% in the TFA group. This is consistent with a previous study of 49 TRA flow diversion cases by Chen et al, who also reported a 0% access complication rate.18 Another study consisting of 18 TRA and 580 TFA flow diversion cases found access site complication rates to be 0% in their TRA group and 2% in the TFA group, which did not reach statistical significance.12 Access complication rates for cardiac procedures have been reported to be 0–0.3% via TRA and 2.0–2.8% via TFA.2 3 20 Occlusion of the radial artery (RAO) may occur in approximately 0.04–6% of cases after radial access.13 18 20–25 However, RAO is nearly always clinically silent due to collateral circulation from the ulnar artery, and for this reason patients are not routinely monitored postoperatively by Doppler ultrasound for RAO. In this study, there were no cases of symptomatic radial artery occlusion. Forearm compartment syndrome is also a very rare complication that was reported to occur with one case out of 9681 in a study of TRA interventional cardiology procedures.20 This complication can be avoided by puncturing the distal radial artery which is outside of the forearm compartments, or by avoiding puncturing the radial artery deep to the brachioradialis muscle.25
The risk of access site complications with TFA procedures has been generally considered acceptable as the rate is low. However, even uncomplicated access complications such as superficial hematomas can prolong hospital stay. Measures to manage access site complications range from assisted compression for superficial hematomas, to clotting agent injection for pseudoaneurysms, and to operative repairs in cases of occlusion, pseudoaneurysm and retroperitoneal hematomas. In addition, blood transfusion is often indicated if access site bleeding leads to hemodynamic instability. These interventions increase patient risk as well as healthcare cost.26–28 Specifically, in cases of flow diversion, hemodynamic instability and life-threatening hemorrhages may affect DAPT management. Halting DAPT therapy is associated with significant thromboembolic and stent occlusion risk, which can lead to devastating stroke.29 Furthermore, thrombolytics are often used to treat in-stent thrombosis. In our cohort, one TFA case was complicated by in-stent thrombosis. The patient was given intra-arterial tissue plasminogen activator, heparin and DAPT, but unfortunately developed a severe retroperitoneal hemorrhage and expired. In the MATRIX trial, a randomized controlled trial of 8404 patients undergoing TRA or TFA interventional cardiology procedures, the number needed to treat to prevent one death from TFA was 169.8 Thus, a very large patient cohort is necessary to evaluate a mortality benefit.
Early reports of TRA flow diversion beginning in 2013 were mostly on patients with challenging anatomy such as type III or bovine aortic arches.15–17 The expanded adoption of TRA as a mainstay approach for flow diversion is relatively new, as is reflected by the high ratio between TFA and TRA case numbers (2151:134) in the data pooled from 14 centers. Even though a large proportion of procedures in this study were performed via TFA, it was sufficiently powered to reveal a statistically significant reduction in access site complications and overall complications in the TRA group. All TRA procedures in this study were performed during the later portion of the study period, between 2016 and 2019. Theoretically, the improved technical familiarity with flow diversion and newer generations of devices during this era could have confounding effects on the overall complication rates. However, we did not observe any significant change in femoral overall complication rates between the pre-radial and radial eras. Furthermore, our subgroup analysis of procedures performed from 2016 to 2019 continued to show a lower overall complication rate in the TRA group. Our findings are consistent with previous cardiology studies wherein not only were access site complications lower, but net adverse clinical events were fewer with radial than femoral access.8 We speculate potential reasons could include a combination of factors, such as the need to pause or alter antiplatelet and anticoagulation management in the event of access site hematomas as well as coagulopathy or complications associated with blood transfusions. However, future studies will be necessary to determine this.
We also found that a broad range of aneurysm locations can be accessed for flow diversion with TRA, despite the tortuous path of navigation via the radial artery and the lack of a radial-dedicated catheter system. This large multicenter study demonstrates a significant safety benefit with TRA flow diversion in decreasing access site and overall complication rates, as well as the feasibility of treating both ruptured and unruptured aneurysms via TRA at a wide range of locations. Combining these findings with other benefits of TRA, including higher patient preference, elimination of post-procedural bed rest and decreased cost, we continue to advocate for the transition to a radial-first approach for endovascular flow diversion.5 9 30
Limitations
This is a retrospective study with inherent selection bias. The collective flow diversion experience has grown and matured over the years, which helped providers in this study determine patient suitability for each access approach. Proper patient selection will continue to be relevant in future TRA and TFA flow diversion practice. This study is also limited by its multicenter design with inevitable heterogeneity of patient selection criteria and technical variations. However, this does reflect a “real-world” cohort, in which patients with a broad range of aneurysm locations benefited from TRA in diverse settings. In addition, the scope of this study is the safety of TRA flow diversion, and does not cover outcomes such as aneurysm occlusion, catheter systems or the subsequent functional status of the patients, which will be examined in subsequent studies.
Conclusion
This multicenter study demonstrated that TRA was a safe and feasible approach for flow diversion to treat cerebral aneurysms at a wide range of locations. Both access site complication rate and overall complication rate appeared to be lower in TRA flow diversion compared with TFA, although a large proportion of procedures in this study were performed via TFA. With growing experience, we believe there are safety benefits in transitioning to a radial-first approach for endovascular flow diversion. Further large prospective studies are indicated.
Acknowledgments
We would like to acknowledge Roberto Suazo for his excellent illustration.
References
Footnotes
Twitter @PascalJabbourMD, @AdamArthurMD, @MichaelNahhas, @DornbosIII_MD, @Starke_neurosurgery
YL and SHC contributed equally.
Contributors Conception: RMS. Data acquisition: all authors. Statistical analysis: YL and RMS. Drafting and critical revisions: all authors. Final approval and agreement to accountability: all authors.
Funding This research is in part supported by National Institutes of Health (R01NS111119-01A1) and (UL1TR002736, KL2TR002737) through the Miami Clinical and Translational Science Institute.
Competing interests RMS research is supported by the NREF, Joe Niekro Foundation, Brain Aneurysm Foundation, Bee Foundation, and by National Institute of Health (R01NS111119-01A1) and (UL1TR002736, KL2TR002737) through the Miami Clinical and Translational Science Institute, from the National Center for Advancing Translational Sciences and the National Institute on Minority Health and Health Disparities. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. RMS has consulting and teaching agreements with Penumbra, Abbott, Medtronic, InNeuroCo and Cerenovus. DRY: Medtronic Neurovascular: Consultant, Cerenovus: Consultant, Rapid Medical and Neuralanalytics: consultant. ECP: Stryker Neurovascular: Consultant, Penumbra: Consultant, RIST Neurovascular: Stockholder, Medtronic Neurovascular: Consultant, Cerenovus: Consultant. MRL: Grants: National Institutes of Health (R01NS105692, R01NS088072, U24NS100654); American Heart Association (18CDA34110295); The Aneurysm and AVM Foundation. Unrestricted educational grants: Stryker Neurovascular, Medtronic, Philips Volcano. Equity interest: eLoupes Inc, Cerebrotech, Synchron. AS: Penumbra: consulting, research support, Stryker: consulting, Cerenovus: consulting. CMS: NTI stockholder, AANS honoraria. ASA: Consultant for Johnson and Johnson, Medtronic, Microvention, Penumbra, Scientia, Siemens, Stryker. Research support from Balt, Cerenovus, Medtronic, Microvention, Penumbra, Siemens, and Stryker. Shareholder in Bendit, Cerebrotech, Endostream, Magneto, Marblehead, Neurogami, Serenity, Synchron, Triad Medical, Vascular Simulations. JWO: Disclosures: consultant for Terumo, Medtronic, Microvention. Royalties: Caeli Vascular, inc.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.