Article Text

Abstract
Background Evidence regarding the most appropriate management of aneurysm recurrences following coiling consists only of uncontrolled case series and the resulting expert opinions, which range from not following coiled patients at all to performing invasive angiography at regular intervals.
Methods We discuss several current attitudes toward how to manage post-coiling recurrences and outline an approach to finding concrete, practical answers to common clinical questions.
Results Although some maxims and general statements can be reluctantly offered, in the absence of evidence the best approach is to emphasize proper methods in order to one day find reliable answers. These can only come from randomized clinical trials. The multitude of research questions is an added difficulty. A program of necessary trials is proposed and centers are encouraged to work in a collaborative fashion in order to offer best possible care as well as progress.
Conclusion Common clinical questions, including how to follow coiled aneurysm patients, if and when to re-treat, and with which treatment modality, are best addressed with the sound scientific methodology of clinical trials.
- Aneurysm
- coil
- coiling
- follow-up
- intracranial aneurysm
- methodology
- recurrence
Statistics from Altmetric.com
The clinical problems related to intracranial aneurysm recurrences after endovascular treatment remain difficult to evaluate objectively. Should we dutifully look for recurrences in all patients? Do we need to treat all the recurrences we find? If so, how and when? Other than for clear-cut cases, such as recurrences that have re-bled, or those with recurrent or persistent symptoms, for which angiographic re-evaluation and retreatment are likely uncontroversial, recurrences continue to plague our field with more questions than answers. This issue, like many others, has been obscured rather than enlightened by a train of a priori prudential maxims and ‘common sense’ arguments, unreliable statistics and poorly justified expert opinions. Compounding this issue is the fact that preventing recurrences has often been used as a marketing tactic for new devices, or used as fodder in the turf battle with aneurysm clippers.
Questions of whether and when to re-treat an asymptomatic recurrent aneurysm following coiling cannot be disentangled from issues related to imaging follow-up protocols, since most retreatments are performed after radiologic documentation of a sizable recurrence. How to follow treated patients is therefore a separate but related issue which also remains controversial.
We will first attempt to clarify the problems by analyzing the literature in order to pose the most pertinent questions. While we will reluctantly provide some opinions, our main objective here is to offer a framework that can one day give practical, reliable answers, if we are willing to work rather than argue, and humbly admit uncertainty rather than pontificate. Not surprisingly, the questions are numerous and inter-related, leaving much room for the introduction of errors, misinterpretations and hasty conclusions. One fundamental problem is that we have not performed our clinical research responsibilities properly from the very beginning of the endovascular story, so now all problems resurface with more force and complexity. The problems related to recurrences post coiling require a discussion of the context and importance of this question relative to the other unanswered questions in our field. Until we, as a community, can come together to work toward answering these questions, we will be resigned to the current method of so-called knowledge sharing: experts giving their opinions. The task of ordering the types of questions our patients need answered requires a frank assessment of what little is known, and what remains to be determined. These questions can be ordered and organized hierarchically, from the most fundamental to more specific questions.
As is commonly the case, specific questions are more easily addressed than fundamental ones. So we will first deal with the relatively simpler questions of the timing and type of retreatment, followed by the more difficult question of whether following patients is necessary after endovascular treatment. We will finally propose a canvas for designing the trials we need to appropriately deal with the problems imposed on our patients, created by our own treatments.
Retreatments: selection and timing
When a significant recurrence is found, whether the patient should be re-treated remains a difficult decision that draws on clinical judgment; typical items that are factored in this decision are the size of the recurrence, the status of the initial lesion (ruptured vs unruptured), time since the initial treatment, the purported risk of subarachnoid hemorrhage (SAH) according to shape (saccular, multilobulated) or location, the likelihood of successful, durable obliteration with retreatment, estimated procedural risks and a host of other factors specific to the case (eg, age, history, concomitant diseases). The decision to re-treat suffers from wide interpersonal variability, as was recently shown.1 2 With this problem we are again confronting a preventive intervention that carries risks, with unknown efficacy and the absence of reliable evidence. Many parallels exist between this decision and the one to initially treat an unruptured intracranial aneurysm, which itself remains plagued with uncertainty.3 Outside of a proper clinical trial, this type of question cannot be reliably answered.
So let us now examine an easier question: once the decision to re-treat has been made, when is it best to proceed? Here we do not have any proper answers either, only simple observations. Waiting for a recurrent aneurysm to increase in size may facilitate surgical clipping, since recurrences often have short, sclerotic, broad-based necks which leave little room for safe clip application. When the recurrence is too small, one immediate option is surgical extraction of the coils from the aneurysm sac, which may increase the risk of retreatment.4 Delaying retreatment favors both surgical and endovascular treatment, allowing development of more tissue at the neck to accommodate clip blades, or conversely, a better neck-to-sac ratio to help coiling without jeopardizing the parent vessel. How long one can wait is a difficult question, since no one knows the risks involved in observing a recurrent aneurysm. Given that neck size and morphology can change between evaluations, any retreatment should only be planned following a recent angiographic evaluation.
What type of retreatment is best?
Re-treating a recurrent aneurysm with additional coils is notoriously bound for failure in perhaps 50% of cases,5 and it seems reasonable to offer something different than what was initially done in order to hope for better results. Under these circumstances, there is potential for uncontrolled human experimentation. No reliable evidence exists to choose between microsurgical or endovascular treatments and decisions will often be based on ‘clinical judgment’ (according to eg, age, location, additional lesions, anticipated technical difficulties, physician preferences, available devices or opportunities). These opinions vary widely from one specialty to another, as well as from physician to physician within the same specialty.1
A successfully clipped aneurysm has less risk of recurrence, but clipping may be more risky than routine endovascular options. While we possess evidence that coiling is less morbid than clipping for ruptured aneurysms,6 no such evidence is available for recurrences. While some have reported that endovascular retreatments are exceedingly safe,7 we lack a reliable assessment in the absence of severe selection bias. Furthermore, the more adjunctive techniques we add to standard coiling, the less confident we can be that endovascular treatment is less risky than microsurgical clipping. The addition of stents, modified coils, flow diverters or liquid embolics in planning treatment of a recurrent aneurysm will undoubtedly involve more risks than simple treatment with platinum coils. Compounding this difficulty is the fact that endovascular clinical trials of devices, when they exist, typically exclude patients with recurrences,8–10 and there is no way to know whether alleged advances in endovascular treatment offered by these products, if they exist, can be applied to patients with recurrences. This specific difficulty can easily be corrected in the future: we should no longer accept trials with too narrow selection criteria, which exclude for example patients with recurrences. They are bound to leave behind categories of patients for whom an answer to the question will be most important.
The key questions now are: (a) is the retreatment option under consideration truly effective at preventing another recurrence? and (b) how much additional risk are we willing to accept in order to improve an image? We see no other way to address these important questions accurately and with transparency than to use the established methodology of clinical trials (see below).
Follow-up imaging studies
For almost two decades, we have chosen to follow our coiled aneurysm patients with catheter angiography and to re-treat recurrences with endovascular methods when they became sizable. Follow-up examinations were more frequent and the surveillance period longer if: (a) the patient was young; (b) the aneurysm was initially ruptured; (c) a residual aneurysm or recurrence had already been documented. In the absence of reliable evidence we have been inclined to use prudential maxims to decide what responsible physicians should do, and a common answer to the problem of recurrence was to follow patients closely. The difficulty is that by increasing surveillance we may be causing more harm than good, as recently claimed by van Rooij and Sluzewski.11 How patients are followed has been changing, first in an imperceptible fashion, and now more obviously: there is a trend for resorting to less frequent, less-invasive imaging, and to proceed with retreatment in a smaller number of patients. This change in conduct, however, is based on very little data. One way to dissolve the problem of recurrences then is simply to stop monitoring patients.
In the only randomized trial available (ISAT) late rebleeding was more frequent (though not significantly so) after coiling than clipping (7% vs 3%) but late retreatments were clearly more frequent (9% vs 0.85%).12 One of the criticisms of the ISAT methodology is that the clipped patients were not followed as assiduously as the coiled patients, and this group may have undetected aneurysm recurrences as well. Hence the comparison between retreatment rates is not valid. It may be interesting to note further that a proportion of aneurysms in this randomized series of small ruptured lesions (some of which had been completely occluded), recurred only after 3 years, suggesting that some recurrences take longer to become apparent.12 But again this is not a strong objection to coiling; the more relevant question is whether the frequency of recurrent SAH is sufficient to justify follow-up imaging in all these patients. The answer seems to be no, at least for van Rooij and Sluzewski.11 If SAH is considered a life-long disease because patients remain at higher risk of recurrent SAH than the general population, screening clipped patients (and by extrapolation, coiled patients) was not shown to be cost-effective.11–14 It is true that in the long term, rebleeds in ISAT6 (and in CARAT15) were reassuringly uncommon, but would this still be true had follow-up imaging and retreatments not been performed?16 17 The proposition to cease follow-up when non-invasive studies show complete or near-complete occlusion at 6 months has been made11; we believe this choice of conduct remains risky; we know how complacent self-evaluation of angiographic results can be.18 Combined with pressure to use less-invasive methods such as MR angiography for follow-up with the attending difficulty in reliably comparing two different modalities at two different dates (typically digital subtraction angiography at the end of treatment and MR angiography at 6 months) could yield a spuriously high proportion of ‘stable near-occlusions’ that could never be shown to be erroneous if longer follow-up is not performed.
There exists a tension between individual care and a more global assessment of our performance, as well as between two common prudent attitudes that may not be equally appropriate, depending on the context: ‘More care (read: more follow-up exams) means better care’ versus ‘Patients should not be submitted to tests (that can lead to treatments) when treatment has not yet been proven beneficial’. The latter principle is one version of the ‘primum non nocere’ clause that may now be more appropriate to a more mature field. When endovascular treatment was progressively supplanting clipping it may have been prudent to ensure that the coiling treatment would ‘hold’. By recommending more frequent and long follow-up simply because it led to increased detection of recurrences, we fell into a fallacy: the mere presence of an imaging finding does not ‘mandate’ doing something about it.5 In general, we must first prove that our actions lead to better clinical outcomes. This proof is not available for any type of patient with an aneurysm recurrence, not even the troublesome cases of early (within 6 months) recurrence. The expedient solution we should resist is to offer guidelines based on expert opinions. At best, these would be based on weak observational evidence if any, and conflicts of interests are bound to bias our judgments. Perhaps experts should limit their recommendations to the selection and formulation of the most burning clinical questions, as we will see below. We know that the only reliable way to demonstrate clinical benefit from follow-up imaging or from new devices designed to improve efficacy is to employ the rigorous methodology of a randomized trial.19 20
The trials we need
How can we find the optimal way to manage our patients, and how can we find answers to these various questions and their combinations? For one thing, we now believe that we cannot act and then reflect only afterwards on our practices. This is exactly the type of behavior which has led us into this dead-end. Rather than separate research and practice, we should do both simultaneously, revealing the uncertainty to our patients up front, and learning as we go, providing the best care that is currently possible. Hence we need to resort to trials. We need to make clinical decisions every day; when the reliable knowledge to make these decisions is lacking, how else can we proceed? The sheer number of unanswered questions we have reviewed so far is an immediate difficulty, but we should not let ourselves be intimidated by this complexity. This should only serve as a reminder that we have not done our job properly so far. The first step is to formulate as precisely as we can each question and attempt to ‘classify’ questions—for example in table 1.
Pertinent questions
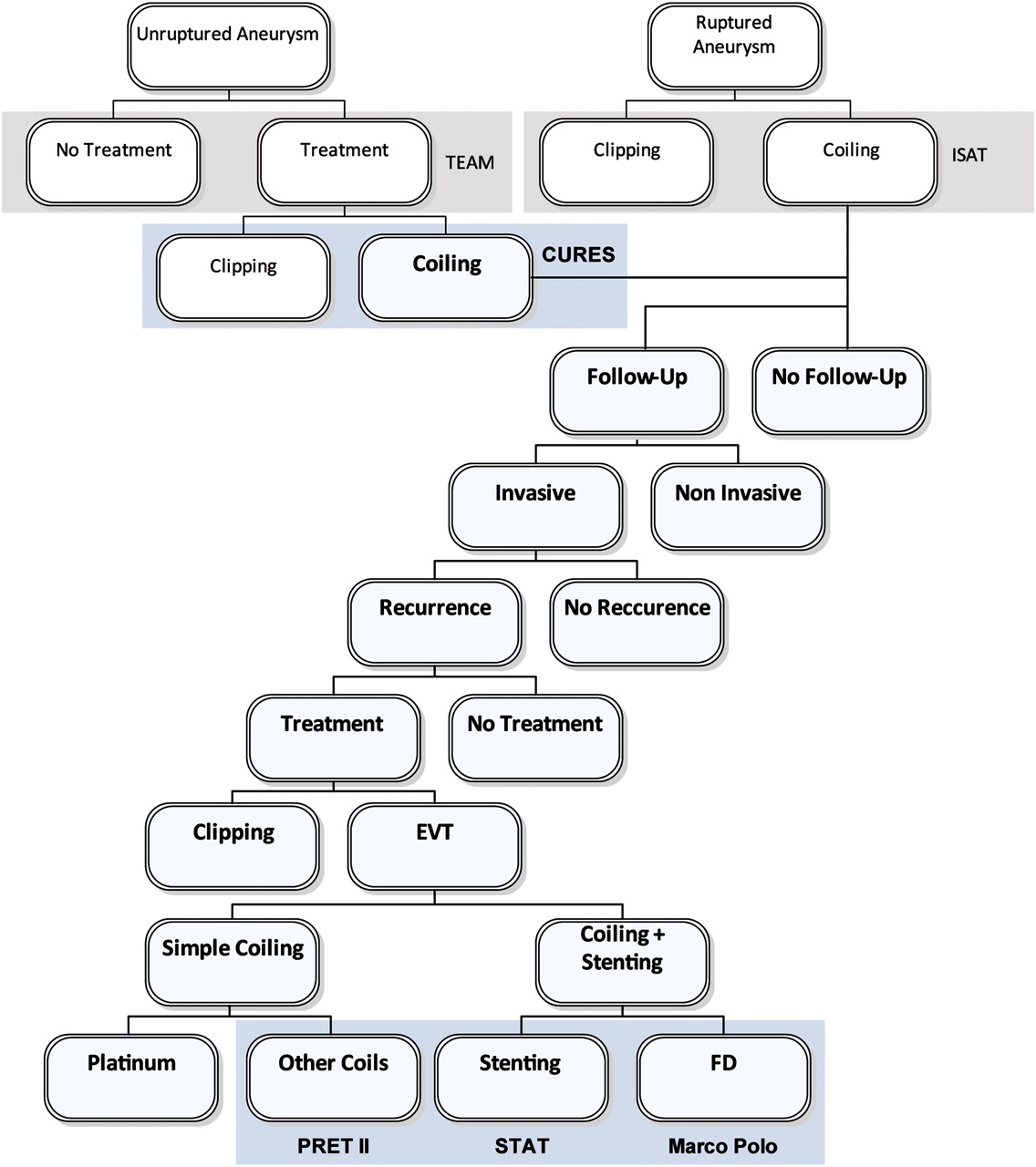
Can all these questions be submitted to a randomized controlled trial? If we resort to multiple randomized controlled trials, which ones should be prioritized? Here we illustrate the problem with a diagram, integrating our questions regarding recurrences with questions regarding initial treatments, giving an overview that illustrates a hierarchy of trials, with different levels (figure 1). Now what?
{kind=link}
A tentative hierarchy of trials on aneurysms. Please note the lack of trials addressing the more fundamental questions. ISAT: International Subarachnoid Aneurysm Trial; TEAM: Trial on Endovascular Aneurysm Management; CURES: Canadian UnRuptured Endovascular versus Surgery; PRET: patients Prone to Recurrence after Endovascular Treatment; STAT: Stenting in the Treatment of Aneurysm Trial.
The first thing to notice is the large amount of work that needs to be done. But how else can we appropriately inform and treat our patients? Perhaps we can imagine that (a) if a center works as an organization, and (b) if questions that remain unsolved are formulated into trials, the very same patient that is included at the top of the diagram may benefit from all research efforts that follow below. Furthermore, at each step, patients will be informed of the uncertainty, protected from fashion and conflicts of interest, and will have access to optimal management strategies (the best possible given the gaps in our knowledge) as they become known (and not earlier, when decision making is close to wishful thinking). Each trial helps other trials, all centers collaborate in providing cutting-edge care, in forwarding knowledge, and the practice of the field becomes informed and targeted, self-controlled by a rational process guided by scientific principles. This is the idea behind a consortium of neurointerventional centers.21
Now how to select the appropriate research questions, the hypotheses that will structure the design of these trials? A scientific principle may prove helpful: in each case, what must be trialed are the actions that we are tempted to offer, but that have never been validated. Under this paradigm, whenever a physician contemplates using a treatment for an unproven benefit, he or she should do so within the context of a trial: they offer the patient a chance to be treated with the new, promising treatment, along with an equal chance of escaping possible false promises and potential added risks. This principle applies equally to radiologic testing protocols as well as to treatment options.
Once more, proceeding from the easiest to the most difficult, from less to the more fundamental questions: (i) if we do not want to question the necessity of retreatment in a particular patient but want to propose a novel device, this should be done within a randomized controlled trial, comparing the new option with the more conventional alternative. This is the design of the PRET II trial, which compares platinum and hydrogel coils for recurrent aneurysms,22 or the Marco Polo trial (http://clinicaltrials.gov/CT2/Show/NCT01084681), which is not limited to, but does not exclude recurrences. The same principle should apply to those proposing the use of stents as part of a retreatment plan; we have designed a trial for this purpose, the STAT trial. (ii) If the need for retreatment itself is questioned, then we need a trial comparing retreatment with observation, a more fundamental question that remains unsettled. (iii) If the need for imaging follow-up after 6 months is in question, then we should design a trial comparing the potential benefits to patients of performing any follow-up studies at all, compared with not doing them.
For those who still consider coiling an experimental treatment that has, without evidence, replaced clipping, an aneurysm recurrence remains the signature of failure, and they may prefer to clip the recurrence, because they believe ‘standard’ treatment was originally withheld, and clipping may be no more risky than complex endovascular approaches. But then they should perhaps submit their pretensions to the verdict of a trial in the spirit of the CURES trial.23
Another fact that becomes conspicuous when looking at the diagram is the lack of trials as we go up in the hierarchy, with more fundamental, but more critical questions. We know from experience that the more fundamental the question, the more difficult it is to implement a trial.24 Once more let us not be cowed by the magnitude of this problem. All participating centers need not participate in all trials. Perhaps some centers will only contribute at the bottom of the hierarchy. Others, enthralled by the promises of evidence-based medicine, may progressively adopt more fundamental trials. It is only by adopting rational ways to guide our actions that we can escape the current free-for-all and achieve real progress.
We cannot imagine that anyone would be interested enough to consider the relative urgency of the above questions, if not the community of physicians caring for these patients. It is time to get our act together, and work as a unified body to provide, simultaneously, optimal care in a transparent context that will eventually lead to demonstrably better patient outcomes.
Key messages
Recurrences after endovascular treatment of intracranial aneurysms, their impact as well as their management, remain controversial.
This problem is closely connected to other important issues, such as follow-up imaging protocols after treatment, as well as to the use of new devices that promise to be more effective, but lack rigorous evidence of their worth.
These problems and controversies will remain pervasive, and will increase in complexity until proper scientific practices are more widely adopted in the endovascular community.
In this context, optimal clinical care can only be provided by a concerted effort to design and participate in meaningful randomized clinical trials.
References
Footnotes
Paper presented at the 7th annual meeting of the SNIS, Carlsbad, California, United States. July 26–30, 2010.
Competing interests Jean Raymond is a principal investigator for the PRET and STAT studies. Tim E. Darsaut is a principal investigator for the CURES study.
Provenance and peer review Not commissioned; internally peer reviewed.