Article Text

Abstract
Objective Tandem occlusions of the internal carotid artery (ICA) and a major intracranial artery respond poorly to intravenous thrombolytic therapy, and are usually managed by endovascular means. This study describes experience with stent-assisted endovascular ICA revascularization and stent-based thrombectomy.
Methods In patients with tandem ICA–middle cerebral artery (MCA)/distal ICA occlusion, the carotid occlusion was recanalized by primary angioplasty and stent implantation, and the distal occlusion by stent-based thrombectomy. Two variant techniques are described.
Results Seven consecutive patients, mean age 64.1 years (range 49–75) and mean admission National Institutes of Health Stroke Scale score of 23, were included. Occlusion sites were tandem proximal ICA and MCA trunk (six patients) and tandem proximal left ICA and ICA terminus (one patient). Complete recanalization with complete perfusion (Thrombolysis in Myocardial Infarction [TIMI] 3, Thrombolysis in Cerebral Infarction [TICI] 3) was achieved in six patients and partial recanalization with partial perfusion (TIMI 2, TICI 2A) in one. Mean time to therapy was 4.9 h (range 3–6.5); mean time to recanalization was 55 min (range 38–65 min). CT performed 1 day after recanalization showed cortical sparing (>90% of the cortex at risk) in seven patients. Five patients (72%) presented with good clinical outcome (modified Rankin Scale (mRS) score 0–2) at 1 month; one patient (patient No 7) reached an mRS score of 3 and one patient died.
Conclusions In selected cases of acute ICA occlusion and concomitant major vessel embolic stroke, angioplasty and stenting of the proximal occlusion and stent-based thrombectomy of the intracranial occlusion may be feasible, effective and safe, and provide early neurological improvement. Further experience and prospective studies are warranted.
Statistics from Altmetric.com
Introduction
Extracranial internal carotid artery (ICA) occlusion with tandem distal occlusion is usually associated with major acute stroke leading to severe disability or death.1 ,2 In this situation, intravenous thrombolysis and other combined approaches have been attempted with limited success.3–7 A significant clot burden and limited delivery of the thrombolytic drug to the distal occlusion may explain the poor results in tandem major occlusions.8 Endovascular treatment has become a more frequent approach to managing these patients, with or without previous intra-venous thrombolysis.6 In selected cases, successful revascularization of carotid occlusion with stent implantation immediately followed by intracranial intra-arterial thrombolysis, balloon angioplasty or thromboaspiration has been reported.9–13
Castaño et al were the first to describe the use of self-expanding stents as a thrombectomy device in acute stroke and showed excellent recanalization rates.14 Following this pioneering experience, stent-based neurothrombectomy has been increasingly used in the endovascular management of acute stroke.15 ,16 Experience in the management of tandem occlusions by means of stent-based thrombectomy is still very limited.
We present our recent experience in the endovascular management of major acute stroke in patients presenting with tandem occlusion of the proximal ICA and middle cerebral artery (MCA) or distal ICA (‘T’ occlusion) by means of proximal angioplasty followed by stent-based thrombectomy of the intracranial occlusion. We present two different endovascular approaches and discuss the advantages and disadvantages of each.
Materials and methods
This analysis was conducted with institutional review board approval (03-12-HMO). Informed consent for the study was waived but patients or a family member signed informed consent forms for the endovascular procedure.
Participants included seven consecutive patients with major acute ischemic stroke secondary to tandem occlusion of the ICA and MCA (six patients) or carotid ‘T’ (one patient). In all patients, the proximal occlusion was treated by stent-assisted carotid angioplasty and the distal embolic occlusion was managed with the use of self-expanding microstents as thrombectomy device (Solitaire; ev3, Irvine, California, USA). Patients who sustained endovascular revascularization by other means and those with major intracranial occlusions associated with underlying atherosclerotic stenoses who required permanent stent implant were excluded.
The procedures were performed at a single institution (Hadassah-Hebrew University Medical Center) between March 2010 and October 2011.
The endovascular procedure was performed within 8 h of symptom onset in patients with a National Institutes of Health Stroke Scale (NIHSS) score of >10 on presentation to the emergency department, in cases where there was no cerebral hemorrhage and no clear sign of early cerebral infarction involving more than one-third of the endangered territory. Tandem occlusion was demonstrated on admission cranial CT angiography; MR studies were performed for penumbra evaluation only in selected cases to determine whether there was an indication for endovascular revascularization. Comorbidities and current medications were taken into consideration when the therapeutic options were weighed.
Selected clinical, radiographic and interventional data are presented in table 1. Clinical data included age, admission NIHSS, time to endovascular therapy (defined as the interval from stroke onset to arrival in the angio suite) and modified Rankin Scale (mRS) score at the 1–3 month follow-up. Radiological data included Alberta Stroke Program Early CT Score (ASPECTS),17 occlusion sites and extent of collateral supply on CT angiogram, MR (when available) and postprocedural head CT evaluation. Interventional data included anesthesia type, medications used during endovascular treatment, endovascular techniques, time to recanalization (defined as the interval between introducer sheath placement to first angiographic run showing recanalization), Thrombolysis in Myocardial Infarction (TIMI) flow grade at recanalization and Thrombolysis in Cerebral Infarction (TICI) grade.18 ,19
Demographic information, clinical presentation and outcome
Collateral supply was evaluated as ‘good’, ‘fair’ or ‘poor’. The suggested classification was based on the ratio of the area of parenchyma supplied by collaterals to the total area that should have been supplied by the thrombosed vessel, as assessed on CT scans, MRI and/or digital subtraction angiography. A good supply was defined as a ratio of more than 66%, fair as 33–66% and poor as less than 33%. This classification may be partially correlated with the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) Collateral Flow Grading System on pretreatment angiography,18 where a good collateral supply corresponds to grade 3–4, fair corresponds to grade 2–3 and poor to 0–2.
Assessment of hemorrhagic transformation was based on evaluation of follow-up CT scans by an experienced neuroradiologist. Following established definitions, hemorrhagic transformation was diagnosed in patients with petechial or confluent hemorrhage within the ischemic lesion. Parenchymal hemorrhage was defined as blood clot in the infarcted area with at least a slight space occupying effect. Symptomatic intracerebral hemorrhage was defined as any sign of hemorrhage on follow-up imaging that was associated with clinical deterioration of 4 points on the NIHSS score within 36 h.
Endovascular technique
Patients were intubated and brought to the interventional neuroradiology suite. A single dose of 5000 units of intravenous heparin was given immediately after femoral access was obtained. Diagnostic angiography was performed to confirm the occlusion pattern and collateral supply. Heparin was added before carotid stent implant to achieve an activated clotting time of 230–250 s.
Two endovascular techniques were used in the management of patients with tandem occlusions and these are described below.
Antegrade technique: proximal ICA stenting followed by intracranial stent-based thrombectomy (stenting followed by thrombectomy)
An 8 F 90 cm Concentric Merci balloon guide catheter (Concentric Medical, Mountain View, California, USA) was placed at the distal common carotid artery (CCA) ipsilateral to the occluded ICA. The ICA occlusion was crossed with a Synchro 0.014 inch microguidewire (Boston Scientific, Natick, Massachusetts, USA) and a Rebar 18 microcatheter (ev3). Angiography was performed through the microcatheter to assess ICA patency. Predilation of the cervical occlusion was performed using a 2.5/3.0×20–30 mm balloon. The balloon was then exchanged for a distal protection device (SpiderFX; ev3), which was placed beyond the stenosis. Then, clopidogrel (600 mg) and aspirin (300 mg) were administered per nasogastric tube. A carotid stent (Wallstent, Boston Scientific/Target; or Precise, Cordis Corp, Bridgewater, New Jersey, USA) was placed, and postdilation was performed with a 5.0×20 mm balloon. Carotid angiography was performed to assess recanalization of the ICA and to determine the precise location of the distal occlusion. The microcatheter was navigated through the MCA occlusion and the distal end of the clot was identified. A 4 mm×20 mm Solitaire AB stent (ev3) was fully deployed across the entire occluded segment of the MCA.
After a brief period of 2–5 min of reperfusion, the proximal third of the stent was resheathed and the guiding catheter was repositioned over the stented ICA. The guide catheter balloon was inflated to provide proximal ICA occlusion. The partially deployed stent was slowly pulled back under continuous aspiration through the balloon guide catheter to entrap the clot into the stent (mechanical thrombectomy). Any remaining fragments of the clot were aspirated from the guide catheter.
Reverse technique: proximal balloon angioplasty followed by intracranial stent-based thrombectomy and stent-assisted proximal carotid angioplasty under cerebral protection (thrombectomy followed by stenting)
An 8 F guiding catheter was placed at the distal common carotid artery. Under roadmap, the ICA occlusion was crossed with an SL-10 microcatheter (Boston Scientific/Target) over a 0.014 inch microguidewire (Synchro-14, Boston Scientific/Target). Over a 300 cm Choice floppy 0.014 inch exchange wire (Boston Scientific/Target), the SL-10 catheter was exchanged for a 2.5×20 balloon and angioplasty of the occlusive plaque was performed. The balloon was exchanged for a 0.021 inch ID microcatheter (Rebar 18). The microcatheter was navigated through the MCA occlusion and the distal end of the clot was identified. A 4 mm×20 mm Solitaire AB stent (ev3) was fully deployed across the entire occluded segment of the MCA.
After a brief period of 2–5 min of reperfusion, the proximal third of the stent was resheathed. The deployed stent was slowly pulled back under continuous aspiration. After confirming intracranial revascularization, we proceeded to stent-assisted proximal ICA angioplasty under cerebral protection. Patients who were not under antiplatelet agents received a loading dose of clopidogrel (600 mg) and aspirin (300 mg) through the nasogastric tube immediately before stent implant. We usually used the SpiderFX protection device (ev3) and either Wallstent (Boston Scientific/Target) or Precise stent (Cordis Corp), depending on patient characteristics.
A final angiogram was performed to assess revascularization of the ICA and MCA and its branches. Heparin was not administered after the procedure. Patients were kept under a double regimen of antiplatelet agents for 3 months (clopidogrel 75 mg/day plus aspirin 100 mg/day) and then clopidogrel was discontinued. Aspirin (100 mg/day) was continued indefinitely.
Results
Seven patients met inclusion criteria, including one woman and six men, with a mean age of 64.1 years (range 49–75 years). Mean admission NIHSS score was 23.4 (range 18–28). Occlusion sites were tandem proximal left ICA and left MCA trunk in four patients, tandem right ICA and MCA trunk in two, and tandem proximal left ICA and ICA terminus (‘T’) in one. In all seven patients, collateral supply was considered poor (ASITN/SIR Collateral Flow Grading System grade 1–2).
Thrombectomy followed by stenting (reverse technique) was used in five patients while stenting followed by thrombectomy (antegrade technique) was used in two. Successful intracranial stent deployment across the clot was achieved in all patients, and Solitaire stents (ev3) were used as the thrombectomy device for distal clot removal in all. Complete recanalization with complete perfusion (TIMI 3, TICI 3) was achieved in six patients, and partial recanalization with partial perfusion (TIMI 2, TICI 2A) was obtained in one (patient No 4). The mean time to therapy was 4.9 h (range 3–6.5). The mean time to recanalization was 54.7 min (range 38–65 min). A mean of 1.5 thrombectomy attempts was needed to achieve removal of the distal clot (range 1–3).
Complete recanalization was achieved in four patients (57%) with one pass. In five patients, the complete embolus was removed in one piece, trapped into the stent; in one patient, a large clot was removed and small pieces of clot were obtained after gentle aspiration through the occluding guiding catheter, and in one patient the stent was recovered with no trapped clot but a major clot was obtained by aspiration through the guiding catheter.
No intracranial self-expanding stent was permanently implanted. However, in patient No 7, a balloon-expandable stent was implanted in a significant cavernous stenosis after successful ICA terminus thrombectomy. In five patients with complete extracranial ICA occlusion, Precise stents (Cordis Neurovascular, Miami Lakes, Florida, USA) were implanted; in two, Wallstent were used. ICA stent implantation was preceded by predilation and followed by postdilation. Stenting and postdilation were performed under cerebral protection in the five patients who sustained thrombectomy followed by stenting, as well as in both patients who sustained the reverse recanalization strategy. No embolic event occurred during carotid angioplasty in any patient.
On routine CT scans performed 24 h after recanalization, all seven patients demonstrated cortical sparing (>90% of the cortex at risk). This is particularly remarkable considering that all presented with very limited collateral flow at admission angiography. Six patients presented with lenticulostriate dependent deep residual infarcted areas on CT (volume ranged from 0.8 to 4 cm3).
In this series, no patient required decompressive craniectomy for mass effect or infarction. Patient No 2 presented with a deep-seated parenchymal and intraventricular hemorrhage 12 h after a successful and uneventful revascularization procedure, and died after 10 days (mortality 14%). Five patients (72%) presented with a good clinical outcome (mRS score 0–2) at 1 month; one patient (patient No 7) obtained an mRS score of 3 at 1 month.
Illustrative cases
Case No 5
A 70-year-old was transferred to our center 2.5 h after stroke onset with an NIHSS score of 23. The patient had a history of multiple partially controlled vascular risk factors. On arrival, the patient was drowsy with global dysphasia and gaze deviation, and presented right dense hemiplegia. Head CT followed by CT angiogram showed unclear signs of left hemispheric ischemia (ASPECTS 10) and tandem occlusion of the left ICA and proximal MCA.
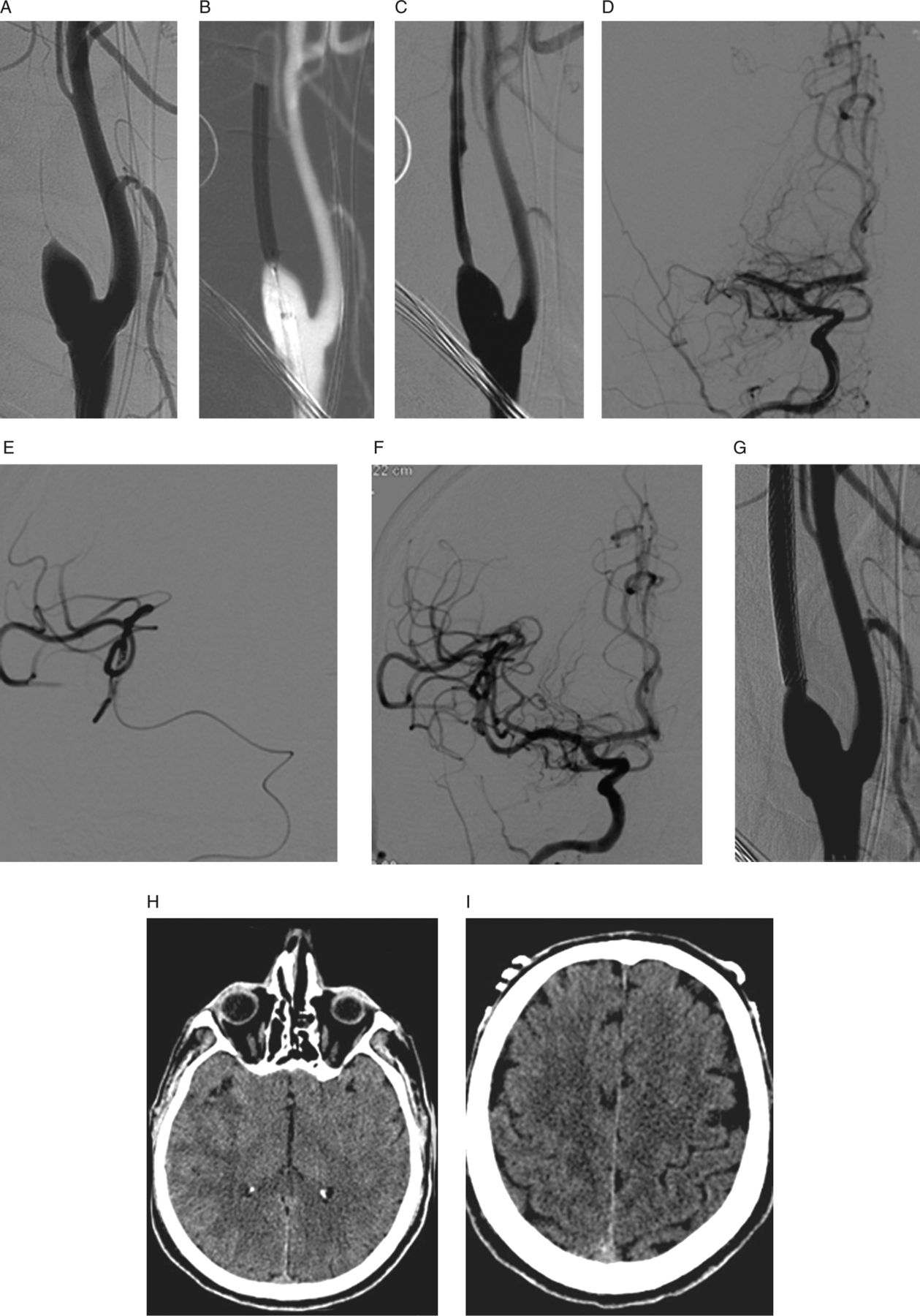
Under general anesthesia, diagnostic angiogram confirmed proximal occlusion of the left ICA (figure 1A). A small angiographic spike marked the ICA ostium and assisted occlusion crossing with a microguidewire. Balloon angioplasty was performed at the proximal left ICA occlusion, achieving partial revascularization (figure 1B). Anteroposterior and lateral views of the cerebral circulation revealed occlusion of the left MCA trunk (figure 1C, D). The balloon was exchanged for a 0.021 microcatheter that was navigated across the MCA occlusion and stent-assisted thrombectomy was performed. In 49 min, after one pass, the left MCA was completely recanalized and reperfused (TIMI 3, TICI 3; figure 1E, F). Stent-assisted angioplasty of the left ICA under cerebral protection was then performed (figure 1G). Head CT performed 30 h later showed a residual caudate infarction and complete cortical sparing (figure 1H). The patient's condition improved, with neurological assessment reaching an NIHSS score of 0 after a week.

A 70-year-old presented with major left hemispheric ischemic stroke and a National Institutes of Health Stroke Scale score of 23 (case No 5). (A) Left common carotid angiogram, lateral projection, depicting proximal occlusion of the left internal carotid artery (ICA). (B) Left common carotid angiogram, lateral projection, obtained after balloon angioplasty showing partial revascularization of the ICA. (C, D) Anteroposterior and lateral views of the cerebral circulation reveals occlusion of the left MCA trunk with poor collateral supply. (E, F) Anteroposterior and lateral views of the cerebral circulation revealed complete recanalization of the MCA trunk after stent-based thrombectomy (TIMI 3, TICI 3). (G) Left common carotid angiogram, lateral projection, showing no residual stenosis after stent-assisted angioplasty of the ICA under cerebral protection. (H) Head CT 30 h after endovascular treatment showed a residual caudate infarction and complete cortical sparing.
Case 6
A 59-year-old was transferred to our center 4 h after major right hemispheric stroke onset with an NIHSS score of 18. The patient had a history of multiple partially controlled vascular risk factors. On arrival, the patient was agitated, with global dysphasia and gaze deviation, and presented with left hemiplegia. Head CT followed by CT angiogram showed no signs of right hemispheric ischemia (ASPECTS 10) and tandem occlusion of the right ICA and MCA.
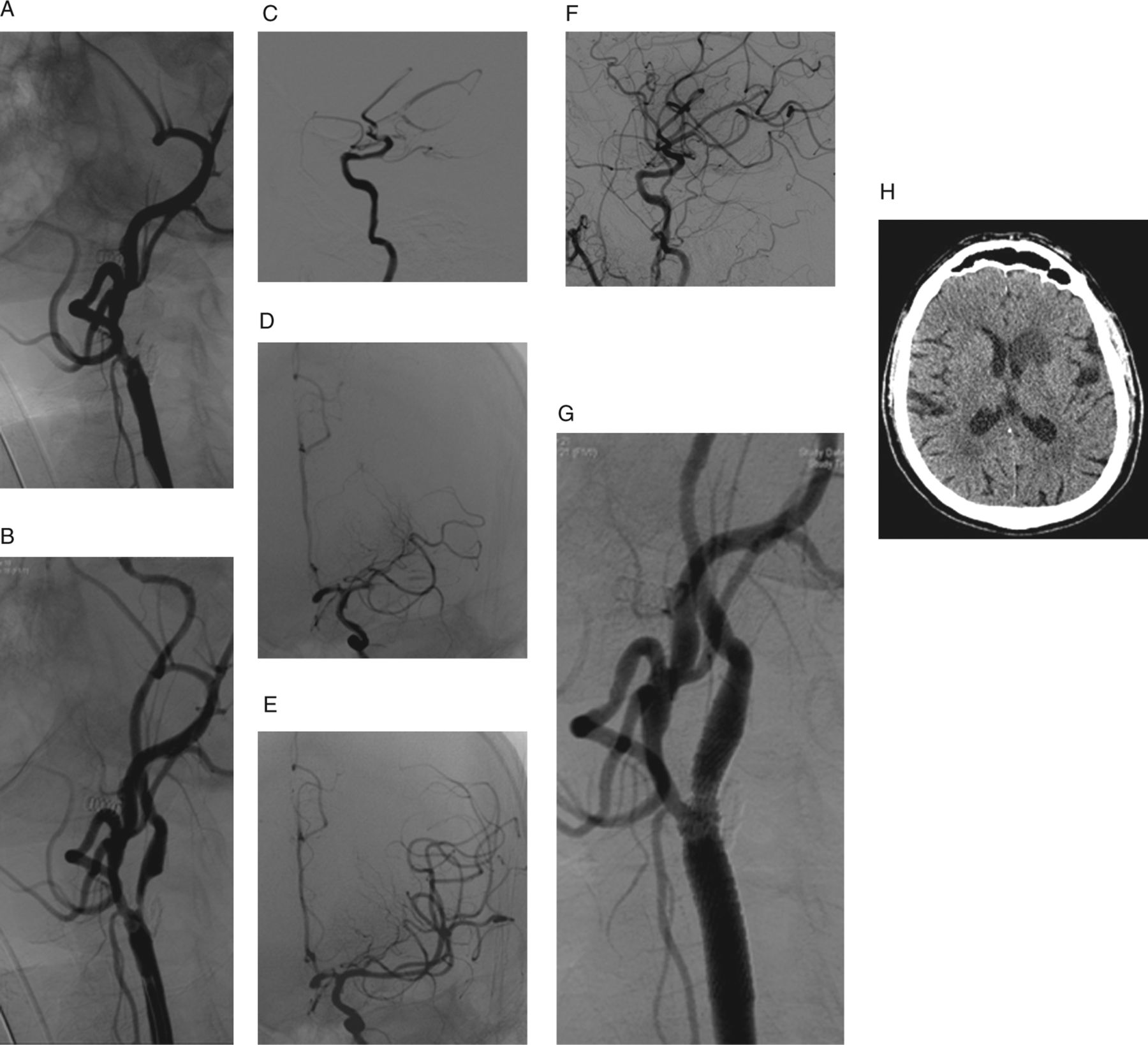
Under general anesthesia, diagnostic angiogram confirmed proximal occlusion of the right ICA (figure 2A). A small angiographic spike marked the ICA ostium and assisted crossing the arterial occlusion with a microguidewire. Balloon angioplasty was performed at the proximal right ICA occlusion achieving partial revascularization (figure 2B,C). Anteroposterior view of the cerebral circulation revealed occlusion of the right MCA trunk (figure 2D). The balloon was exchanged for a 0.021 microcatheter that was navigated across the MCA occlusion (figure 2E). Stent-based thrombectomy was performed. The MCA was completely recanalized and reperfused in a single pass (TIMI 3, TICI 3) (figure 2F). Immediately afterwards, stent-assisted angioplasty of the proximal right ICA was performed under cerebral protection (figure 1G). Follow-up head CT after 24 h showed no signs of ischemic stroke (figure 1H, I). The patient's condition improved, with neurological assessment reaching an NIHSS score of 0 after a week.
{kind=link}
{kind=link}
A 59-year-old presented with major right hemispheric stroke and a National Institutes of Health Stroke Scale score of 18 (case No 6). (A) Right common carotid angiogram, lateral projection, showing proximal occlusion of the right internal carotid artery (ICA). (B, C) Right common carotid roadmap image and angiogram showing balloon angioplasty at the proximal right ICA occlusion achieving partial revascularization. (D) Anteroposterior view of the cerebral circulation revealed occlusion of the right MCA trunk. (E) Microangiogram obtained with a microcatheter across the MCA occlusion showing the patent vessels beyond the embolus. (F) Cerebral angiogram, lateral projection, showing complete revascularization of the MCA after thrombectomy (TIMI 3, TICI 3). (G) Right common carotid angiogram, lateral projection, showing no residual stenosis after stent-assisted angioplasty of the ICA under cerebral protection. (H, I) Head CT obtained 24 h after endovascular treatment showing no signs of ischemic stroke.
Discussion
The natural history of acute stroke secondary to tandem occlusion of the ICA and MCA leads to poor outcomes.1 ,2 Carotid occlusion may cause ischemic stroke secondary to hemodynamic factors, or embolic and hemodynamic factors, with tandem ICA–MCA occlusion cases an example of the second mechanism. Although intravenous tissue plasminogen activator may be useful in other types of acute occlusions, it provides a much more much limited effect in this condition. Even patients presenting within 3 h of symptoms who have no contraindication to intravenous plasminogen activator treatment, have a low probability of recanalizing ICA occlusions and tandem occlusions when this is the primary intervention.3 ,6–8
Endovascular revascularization of tandem occlusions has been reported only recently. Several endovascular techniques have been described, with high rates of recanalization and acceptable clinical outcomes.6 ,7 ,9 ,12 ,13 However, traditional endovascular approaches are usually complex and time consuming, especially when they must address the revascularization of both the proximal and distal sites of occlusion.
Mechanical thrombectomy is a relatively new concept of interventional stroke treatment that is rapidly replacing selective intra-arterial fibrinolysis. The principle is based on rapid clot removal by means of different devices instead of slow pharmacological disintegration of the embolic material after intra-arterial injection. The recent introduction of stent-based thrombectomy has revolutionized the endovascular revascularization of acute large vessel occlusion, with marked improvement in both recanalization rates and times.14–16 ,20 ,21 We recently included this technique in the management of tandem occlusions after performing primary angioplasty/stenting of the proximal ICA occlusion. Our small series of seven consecutive patients with acute ischemic stroke after tandem occlusion treated by endovascular techniques, including extracranial ICA angioplasty and intracranial stent-based thrombectomy, confirms the feasibility, efficacy and safety of this proposed approach.
The main finding of this report is that stent-assisted endovascular revascularization of ICA occlusion followed by stent-based thrombectomy of tandem ICA and distal MCA occlusion in the setting of acute ischemic stroke is feasible, achieves a high revascularization rate, presents an acceptable safety profile and significantly improves neurological outcome in selected patients. This novel approach has proved to be fast (less than 1 h after gaining femoral access) and effective in terms of recanalization, resulting in TIMI 2–3 in all cases in this series and in very good functional outcome (mRS 0–2) in five out of seven patients (71%).
However, this series also presented procedure related mortality (14%). Patient No 2, a 66-year-old, presented with parenchymal hemorrhage 2 days after the endovascular procedure that evolved to fatal intracerebral and intraventricular hemorrhage. This hemorrhagic complication occurred after a successful revascularization procedure that was uneventful in terms of the technical aspects of the neuroendovascular procedure, with no procedural trauma. The occurrence of hemorrhagic complications after mechanical recanalization requires further investigation.
Here we described two different approaches, which vary in the timing for the ICA stenting step. The first (antegrade) approach involves protected stent-assisted carotid angioplasty followed by intracranial thrombectomy, and the second (reverse) approach involves primary carotid angioplasty followed by intracranial thrombectomy and then finally protected stent-assisted angioplasty of the proximal ICA. Both techniques have advantages and disadvantages. The antegrade technique focuses first on the proximal occlusion, which is stented at an early stage, securing the ICA occlusion. However, this postpones the critical distal thrombectomy step, delaying cerebral reperfusion. In this technique, it is crucial to reposition the balloon guiding catheter over the stent artery before removing the partially sheathed thrombectomy device to avoid entrapment of the microstent in the mesh of the implanted carotid stent.
The reverse strategy is increasingly preferred in our center, and is aimed at reducing cerebral ischemia time by postponing ICA reconstruction until after successful intracranial revascularization. The main concern with this approach is that immediately after the thrombectomy step, the guidewire is withdrawn from the carotid lumen, leaving no means of recatheterizing the ICA in case of reocclusion.
Thrombolytic agents were not used in our patients, reducing the chances of hemorrhagic complications associated with their use. However, patients who were not on an antiplatelet regimen received a loading dose of clopidogrel and aspirin immediately before stent implantation. The safety of this practice on acute settings will require further investigation. A double antiplatelet regimen was prescribed for at least 3 months.
This report provides pilot data for a subsequent study on tandem ICA–MCA occlusions treated with stent-based techniques. Endovascular stent assisted recanalization of cervical ICA occlusion followed by intra-arterial thrombolysis, balloon angioplasty and thrombo-aspiration to achieve MCA recanalization was proposed as a valuable option in selected patients.6 ,7 ,9 ,12 ,13 The use of stents as a thrombectomy device has only recently been described but is considered an attractive alternative to intra-arterial thrombolysis and to other thrombectomy devices that are currently available.14–16
The Solitaire AB (ev3) is a stent-like device that was originally designed as a remodeling tool to assist the embolization of wide necked cerebral aneurysms. This device can be completely deployed and fully retrieved back into the microcatheter if needed; detachment is only accomplished with the assistance of an electrical detachment system. The controlled detachment of this device allowed us to first deploy the stent, achieving an immediate recanalization of the artery, and then to remove the partially resheathed stent, using it as a thrombectomy device. This combined approach achieved three desirable effects: rapid endovascular revascularization (endovascular bypass), clot removal (thrombectomy) and avoiding the need to leave a permanent implant. Stent based thrombectomy devices that can be detached if necessary may become a valuable tool in the primary therapy for acute ischemic stroke.15
One of the most challenging technical steps when dealing with tandem occlusion is catheterization of the true lumen of the occluded ICA.22 Small subtle angiographic signs may indicate the most adequate point of entry to the true arterial lumen, as shown in figures 1A and 2A.
Our case series suggests that the ICA stenting and MCA stent thrombectomy approach for acute tandem ICA–MCA occlusion appears to be feasible and safe, and may be associated with early neurological improvement. After having tried different available options, we found proximal angioplasty and distal stent based thrombectomy the most effective and rapid approach in terms of recanalization for tandem occlusions. These encouraging preliminary results await confirmation from further experience and prospective randomized studies.
Acknowledgments
The authors wish to thank Shifra Fraifeld, Senior Medical Writer and Head of Research Support in the Departments of Neurosurgery and Radiology at the Hadassah-Hebrew University Medical Center, for her editorial assistance in the preparation of this manuscript.
References
Footnotes
-
Contributors All authors made a significant contribution to the study and manuscript preparation. JEC, MG, RRL and EI contributed to study conception and design, JEC, MG, GR, SM and SR contributed to data acquisition and JEC, RRL and SR to data interpretation and analysis. JEC and MG drafted the manuscript, JEC, SM, RRL, SR and GR critically revised the paper and EI contributed significant intellectual content. JEC, MG, GR, SM, RRL, SR and EI approved the final version of the manuscript.
-
Competing interests None.
-
Ethics approval The study was approved by institutional review board of Hadassah-Hebrew University Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Data central to this study are included in the manuscript. Readers may contact the corresponding author (jcohenns@yahoo.com) with questions or comments on the article.