Article Text

Abstract
Objective Acute ischemic stroke due to proximal intracranial vessel occlusion is associated with poor prognosis and neurologic outcomes. Outcomes specifically in patients with stroke due to these occlusions and lower National Institutes of Health Stroke Scale (NIHSS) scores (0–7 range) have not been described previously.
Methods We retrospectively reviewed discharge outcomes (reported in our ‘Get With the Guidelines-Stroke’ database) in patients with an admission NIHSS score of 0–7 due to proximal intracranial large vessel occlusion (based on CT angiography results) who were excluded from receiving intravenous (IV) thrombolysis with recombinant tissue plasminogen activator and endovascular intra-arterial (IA) stroke interventions.
Results Among the 204 patients included in our analysis, younger age and lower admission NIHSS score (0–4 range) were strong predictors of good outcome (defined as ability to ambulate independently) at discharge whereas female sex was a predictor of poor outcome. There was no significant difference between cerebrovascular risk factors, specific sites of occlusion, or presenting symptoms and outcomes at discharge. There was great variability in functional outcomes at discharge and discharge disposition (home versus acute or subacute facility or nursing home versus death/hospice) with a trend toward worse outcomes in patients with higher (5–7 range) NIHSS scores on admission.
Conclusions Patients with acute stroke due to large vessel occlusion and low admission NIHSS scores (0–7 range) may have poor functional outcomes at discharge. These patients, if not eligible for IV thrombolysis, might benefit from IA revascularization therapies.
- Stroke
Statistics from Altmetric.com
Introduction
Acute ischemic stroke due to occlusion of proximal intracranial vessels is associated with poor prognosis and neurologic outcomes.1 ,2 Intra-arterial (IA) endovascular interventions are an option for patients with large vessel occlusion and severe neurologic deficit who are not candidates for intravenous (IV) thrombolysis with recombinant tissue plasminogen activator, according to current acute stroke guidelines.3 Modern trials investigating IA approaches to acute stroke with intracranial large vessel occlusion typically use a National Institutes of Health Stroke Scale (NIHSS) score of 8 and higher as an inclusion criterion for study enrollment, at the same time mandating the use of non-invasive imaging (CT angiography or MR angiography) to confirm the presence of large vessel occlusion.
Strokes in patients with large vessel occlusion who are excluded from receiving IV thrombolysis or IA endovascular interventions are associated with worse prognosis and higher mortality, compared with stroke without evidence of large vessel occlusion, especially in conjunction with a baseline NIHSS score in the higher range.1 Functional outcomes specifically in patients with stroke due to proximal intracranial vessel occlusion and a lower NIHSS score (0–7 range) have not been described previously. In this study, we describe outcomes in this population of patients with acute ischemic stroke.
Methods
Study population and selection
This study was approved by our local institutional review board. We retrospectively reviewed cases of acute ischemic stroke admitted to our university based stroke center between January 1, 2010 and November 1, 2012. Using our hospital's ‘Get With The Guidelines–Stroke’ database as well as a retrospective review of clinical charts and images, we collected demographic data, functional level prior to stroke, initial baseline NIHSS score, description of proximal vessel occlusion, discharge NIHSS score, discharge destination, and functional level at discharge. For the present study, we included all patients with acute ischemic stroke and an initial NIHSS score of 0–7 whose imaging studies revealed evidence of proximal vessel occlusion suitable for endovascular stroke intervention but in whom the low NIHSS score precluded this approach. Patients who received IV thrombolysis were excluded from analysis.
Acute stroke protocol
Our center has a stroke neurologist and an endovascular neurosurgeon present on a 24 h basis for immediate clinical evaluation of patients with suspected acute ischemic stroke. Our acute stroke protocol includes clinical evaluation and documentation of baseline NIHSS score, immediately followed by non-contrast brain CT and whole brain CT perfusion imaging in combination with craniocervical CT angiography for all patients with suspected acute ischemic stroke. Stroke severity based on NIHSS score is documented by clinical staff certified through the American Stroke Association's NIHSS training program. All patients with ischemic stroke who present to our center within the first 24 h of symptom onset are evaluated for eligibility for endovascular intervention, using the following general inclusion criteria: (1) radiographic evidence of proximal vessel occlusion with a corresponding perfusion deficit and symptoms consistent with the imaging findings and (2) NIHSS score ≥8.
Neuroimaging protocol
CT perfusion imaging is done using a 320 detector row CT system (Aquilion ONE, Toshiba Medical Systems, Nasu, Japan). Contrast medium infusion (50 mL, Optiray 350, Mallinckrodt, Missouri, USA) is performed at a rate of 5 mL/s via automated antecubital venous injection. Perfusion maps (cerebral blood flow, cerebral blood volume, mean time transit, time to peak, and delay) are reconstructed utilizing Vitrea fX software (Vital Images, Minnetonka, Minnesota, USA). Immediately afterward, craniocervical CT angiography is performed using an infusion of contrast medium (80 mL) at a rate of 4 mL/s, with scanning starting manually once the contrast medium has reached the aortic arch. Perfusion maps and CT angiography are immediately reviewed by the on-call stroke neurologist and endovascular neurosurgeon to determine patient eligibility for IV thrombolysis or endovascular stroke intervention.
Study definitions
Proximal vessel occlusion was defined as the presence of occlusion of a large intracranial vessel (including both the anterior and posterior circulations) with a corresponding perfusion deficit on CT perfusion imaging indicative of an acute ischemic stroke that would be technically eligible for IA endovascular intervention. Specific segments (intracranial internal carotid artery (ICA), M1 and M2 segments of the middle cerebral artery, A1 and A2 anterior cerebral segments of the anterior cerebral artery, the basilar artery, V4 segment of the vertebral artery, and P1 and P2 segments of the posterior cerebral artery) were classified (at the time of CT angiography) on the basis of previously published definitions of proximal versus distal occlusion.4 ,5 Good outcome was defined as the ability to ambulate independently at discharge.
Statistical analysis
Statistical analysis for each outcome variable analyzed in the present study was performed with SPSS software (V.19, IBM Software, Chicago, Illinois, USA). Univariate analysis comparing demographic factors and outcome was performed using Fisher's exact test for categorical data and a two tailed t test for continuous data. For all statistical analyses, p<0.05 was considered statistically significant.
Results
We identified 874 patients with an admission NIHSS score <8 and presentation within the first 24 h of stroke symptom onset. We excluded from analysis 48 patients who did not receive CT angiography to confirm or exclude proximal vessel occlusion, 75 patients who had common carotid and/or cervical ICA occlusion, and 541 patients who had no proximal intracranial vessel occlusion. Six patients presented with a low NIHSS score (range 2–5, median 4) but developed worsening neurological symptoms in the emergency room and were taken for IA intervention; this subgroup of patients was excluded from analysis. A total of 204 patients had a confirmed occlusion and met the inclusion criteria for analysis in the present study (ie, no IV thrombolysis and/or IA endovascular intervention was performed). Fourteen of those 204 patients presented to the emergency room within the first 3 h of stroke onset; these patients were excluded from receiving IV thrombolysis because of presenting NIHSS scores ranging from 0 to 3 (n=10) or delay in recognition of stroke and/or diagnostic evaluation (n=4).
Mean age for the 204 study patients was 71 years, and mean admission NIHSS score was 2.6 (median 2). Demographic, medical history, and baseline level of functioning of these patients are described in table 1. Mean duration of hospitalization was 6.0 days (median 4 days). At discharge, 62% of patients were able to ambulate independently, and 63% of patients were discharged home. Discharge NIHSS score and description of functional status and discharge destination are summarized in table 1.
Baseline characteristics of 204 patients with a National Institutes of Health Stroke Scale score of <8 and proximal intracranial vessel occlusion
Predictors of ability to ambulate independently at discharge are listed in table 2. Younger age and lower admission NIHSS score (0–4) were strong predictors of good outcome at discharge. By dividing admission NIHSS score into a range of 0–4 versus 5–7, we saw a significantly higher chance of good outcome at discharge in patients with the lower admission score range (83% ambulate independently versus 64% unable to ambulate independently, p=0.002). Female sex was a strong predictor of poor outcome (unable to ambulate independently at discharge). We found no significant difference between cerebrovascular risk factors, specific sites of occlusion, or presenting symptoms and outcomes at discharge. Disposition status at discharge and its association with occlusion location are shown in figure 1.
Predictors of functional outcomes at discharge in patients with a National Institutes of Health Stroke Scale score of <8 and proximal intracranial vessel occlusion

Discharge destination of patients with a National Institutes of Health Stroke Scale (NIHSS) score of <8 depending on location of the proximal intracranial vessel occlusion on admission. ACA1/2, A1 or A2 segment of the anterior cerebral artery; Intracran ICA, intracranial internal carotid artery; MCA1/2, M1 or M2 segment of the middle cerebral artery; P1/2, P1 or P2 segment of the posterior cerebral artery.
Functional outcomes and patient discharge destination according to the severity of the NIHSS score on admission are shown in figures 2 and 3. There was great variability in functional outcomes at discharge, with a trend toward worse outcomes in patients with higher NIHSS scores (5–7 range) on admission.
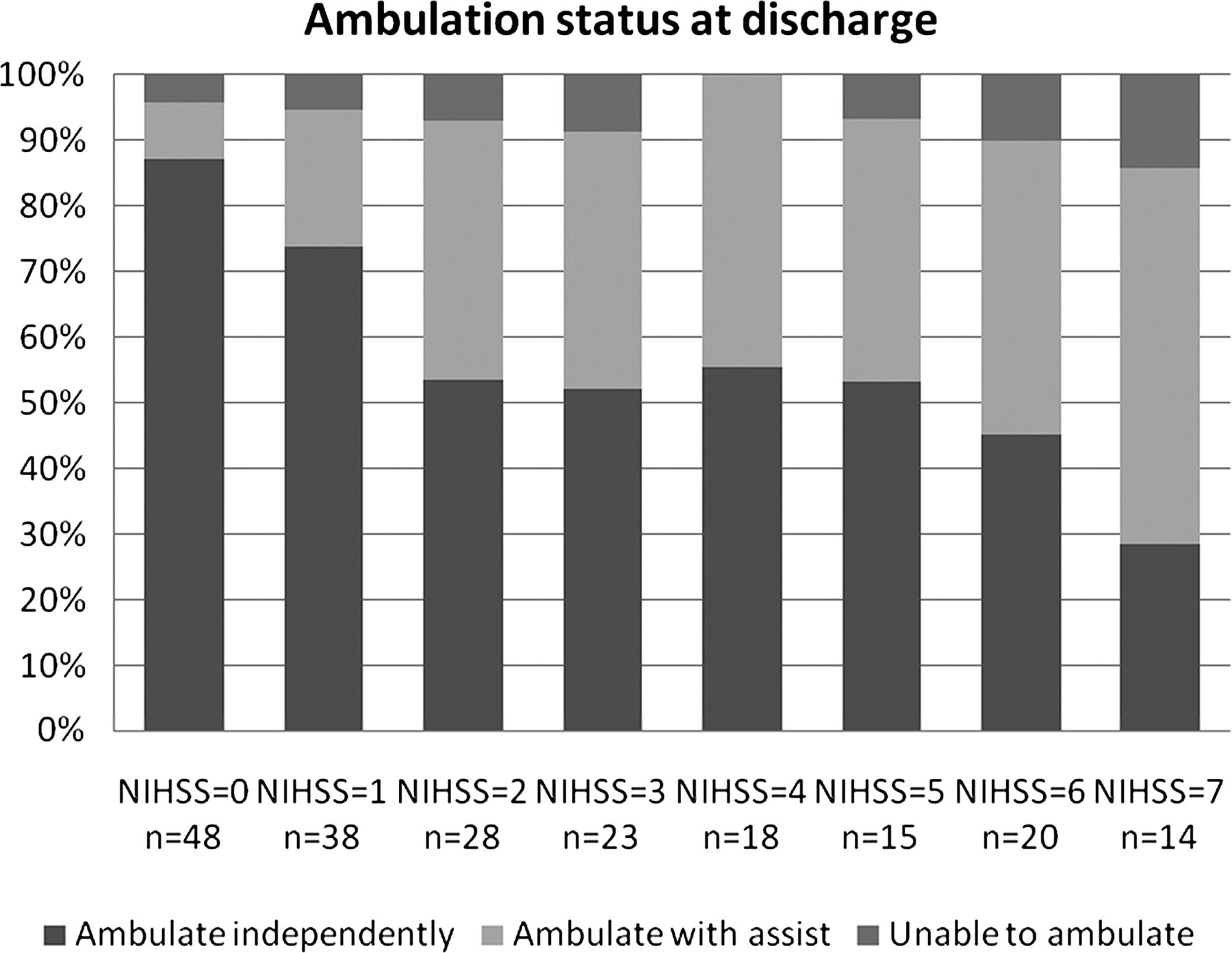
Functional outcomes in patients with proximal intracranial vessel occlusion depending on severity of the National Institutes of Health Stroke Scale (NIHSS) score on admission.

{kind=link}
{kind=link}
{kind=link}
Discharge destination of patients with proximal intracranial vessel occlusion depending on severity of the National Institutes of Health Stroke Scale (NIHSS) score on admission. Facility=acute or subacute rehabilitation facility or nursing home.
Discussion
Historically, an NIHSS score cut-off point of 8 or 10 was used in early stroke trials due to its high sensitivity and specificity in predicting the presence of intracranial large vessel occlusion as a potential target for IA interventions.6 ,7 However, more recent data support the argument that a substantial number of patients with large vessel occlusion can present with rather mild neurological deficits. For example, Smith et al1 demonstrated significant overlap in admission NIHSS scores, including the lower range of baseline NIHSS scores, in patients without large vessel occlusion and in those with intracranial occlusion, even with occlusion expanding beyond a single vessel segment. Similarly, in the study conducted by Maas et al,4 a large number of patients with lower baseline NIHSS scores (55% of patients with NIHSS scores ≤10) were found to have large vessel occlusion on non-invasive imaging investigations potentially amenable to interventional therapy.
It has been previously demonstrated that a finding of intracranial large vessel occlusion(s) during the initial diagnostic evaluation is strongly associated with worse functional outcome and higher mortality rate.1 ,2 Detailed outcomes in patients with intracranial large vessel occlusion presenting within a lower range of NIHSS scores have not been described previously. The main finding of our study is that in patients with acute stroke due to large vessel occlusion and a low admission NIHSS score (0–7 range), there is a great variability in outcomes. Within this range, patients with a baseline minimal neurological deficit had very favorable outcomes at discharge whereas increase in NIHSS score by each point demonstrated a trend towards progressively higher numbers of patients not able to ambulate independently at discharge and requiring transfer to other healthcare facilities, such as rehabilitation facilities or nursing homes. For example, only 29% of patients with an NIHSS score of 7 could ambulate independently at discharge and only 21% were discharged home. Our findings indicate that the NIHSS cut-off point of 8 when considering patients for endovascular IA interventions might need to be revisited in the future. Which patients with lower NIHSS scores who are ineligible for IV thrombolysis and might benefit from IA revascularization therapies remains to be determined.
Our findings are somewhat analogous to those in the study conducted by Smith et al8 of outcomes in patients excluded from IV thrombolysis because of mild or rapidly improving stroke symptoms. In that study, some patients had poor hospital discharge outcomes despite a ‘benign’ appearance of presenting symptoms. Because the results of that study were based solely on the Get With The Guidelines-Stroke database, those authors were not able to determine outcomes specifically for patients with large vessel occlusion.
Poisson et al9 conducted a study of patients with transient ischemic attacks who underwent non-invasive imaging (CT angiography) for detection of large vessel occlusion. They found that 13 patients with symptomatic intracranial large vessel occlusion had higher modified Rankin Scale scores (indicating worse outcome) at 3 months than 84 patients from the control group (patients without intracranial large vessel occlusion). Only patients with transient neurological deficits were included in that study, and the low number of patients with evidence of large vessel occlusion (n=13) limits interpretation of their findings.
In our study, patients who were diagnosed with cervical carotid occlusion were excluded from the final analysis. In clinical practice, on the basis of head or neck angiography alone, a higher level ICA occlusion, such as of the petrous or cavernous ICA segment, can be mistaken for a cervical occlusion because the CT angiogram can show no flow beyond the cervical segment. All patients included in our final analysis underwent whole brain CT perfusion imaging, along with head and neck CT angiography. Studies have shown the superb ability of whole brain CT perfusion to visualize contrast filling distal to the occlusion in an anterograde (in cases of partial occlusion) or retrograde (in cases of complete occlusion, via collateral filling) fashion, helping us to differentiate between cervical and more distal (petrous, cavernous, or ICA terminus) occlusion.10 ,11
Our study has several limitations. First, although each case was individually reviewed and we attempted to determined whether a perfusion deficit (based on CT perfusion results) and/or MRI evidence of acute stroke on a diffusion weighted imaging sequence (in patients eligible for a MRI study) correlated with the vascular territory of the occluded segment, there is a possibility that some occlusions could have been chronic. Second, the definition of good outcome used in our study was the ability to ambulate independently at discharge. This includes modified Rankin Scale scores in the 0–3 range whereas modern studies utilize scores of 0–2 to define good outcome. Long term outcomes, such as modified Rankin Scale score at 90 days, which is commonly used to evaluate outcomes in patients with acute stroke, were not available for analysis. This limits comparison of our data with the results of other studies. In addition, the disproportionally small number of patients with higher NIHSS scores creates a bias toward the majority of patients who had very low NIHSS scores (median score of 2). Finally, a large study population might have revealed significant differences in outcomes on the basis of specific location of the occluded vessel. For example, the presence of basilar occlusion was shown to be predictive of poor outcomes in patients with large vessel occlusion strokes.1 In our study, although there was a trend toward poor outcomes in this population of patients, it did not reach statistical significance.
Conclusion
Our study indicates that selected patients with stroke who fall under the category of ‘lower’ NIHSS score (ie, 0–7 range) and are diagnosed with intracranial vessel occlusion can have poor functional outcome at discharge. These patients, if not eligible for IV thrombolysis, might benefit from IA revascularization therapies, given their poor prognosis. Further studies are needed to determine whether the IA approach can result in improved outcomes in this patient population.
Acknowledgments
The authors thank Paul H Dressel, BFA, for assistance with preparation of the figures, and Debra J Zimmer for editorial assistance.
References
Footnotes
-
Contributors Conception and design: all authors. Data acquisition: MM and MWM. Data analysis and interpretation: MM, MWM, TMD, and TK-H. Literature research: MM. Statistical analysis: MM and TMD. Drafting the manuscript: MM. Critical revision and final approval of manuscript: all authors.
-
Competing interests LNH—grant/research support: Toshiba; consultant: Abbott, Boston Scientific, Cordis, Micrus, and Silk Road; financial interests: Access Closure, Augmenix, Boston Scientific, Claret Medical, Endomation, Micrus, and Valor Medical; board/trustee/officer position: Access Closure and Claret Medical; speakers’ bureau: Abbott Vascular; honoraria: Bard, Boston Scientific, Cleveland Clinic, Complete Conference Management, Cordis, Memorial Health Care System, and SCAI. TK-H—research funding: Genentech. EIL—research grant support, other research support (devices), and honoraria: Boston Scientific; research support: Codman and ev3/Covidien Vascular Therapies; ownership interests: Intratech Medical and Mynx/Access Closure; consultant: Codman, ev3/Covidien Vascular Therapies, and TheraSyn Sensors; fees for carotid stent training: Abbott Vascular and ev3/Covidien Vascular Therapies. MM—educational grant: Toshiba Medical System Corporation. AHS—research grants: National Institutes of Health (co-investigator: NINDS 1R01NS064592-01A1) and University at Buffalo (neither grant applies to the present submission); financial interests: Hotspur, Intratech Medical, StimSox, Valor Medical, and Blockade Medical; consultant: Codman and Shurtleff Inc, Concentric Medical, Covidien Vascular Therapies, GuidePoint Global Consulting, Penumbra, Stryker Neurovascular, and Pulsar Vascular; speakers’ bureaus: Codman and Shurtleff, and Genentech; serves on National Steering Committees for Penumbra 3D Separator Trial and Covidien SWIFT PRIME Trial; advisory board: Codman and Shurtleff, and Covidien Vascular Therapies; honoraria: American Association of Neurological Surgeons’ courses, Annual Peripheral Angioplasty and All That Jazz Course, Penumbra, and from Abbott Vascular and Codman and Shurtleff Inc for training other neurointerventionists in carotid stenting and for training physicians in endovascular stenting for aneurysms. KVS—consultant, speakers’ bureau, honoraria: Toshiba; speakers’ bureau and honoraria: ev3 and The Stroke Group.
-
Ethics approval The institutional review board at the University at Buffalo, State University of New York, approved this study (project 403427-1), and a standard Health Insurance Portability and Accountability Act compliant protocol was followed.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Unpublished anonymized/de-identified data may be available. This would be on a per request basis.