Article Text

Abstract
Background Spinal digital subtraction angiography (DSA) is the gold standard for diagnosis of spinal dural arterial venous fistulas (SDAVFs), but can require extensive time, radiation exposure and contrast dose. We hypothesize that contrast-enhanced time-resolved MR angiography (CE-TR MRA) will have utility for the non-invasive diagnosis and pre-angiographic localization of SDAVFs.
Methods Eighteen patients underwent both CE-TR MRA and DSA for suspected SDAVFs, with DSA performed a median of 11 days (range 0–41) after MRA. CE-TR MRA was performed on a 1.5 T GE unit using Time Resolved Imaging of Contrast Kinetics (TRICKS). CE-TR MRA and DSA images were evaluated for the presence of SDAVFs and location of the feeding arterial supply, with DSA as the reference standard. DSA was also evaluated for the number of vessels catheterized, contrast volume and fluoroscopic and procedure times.
Results Eight of the 18 patients were positive for SDAVF on DSA. Sensitivity, specificity, positive predictive value and negative predictive value for the 18 CE-TR MRAs were 88%, 90%, 88% and 90%, respectively. Localization of the SDAVF arterial supply on CE-TR MRA was within one vertebral level from DSA for 6/7 SDAVFs. Compared with patients with a SDAVF and feeding artery identified on CE-TR MRA, patients with negative or suboptimal CE-TR MRA had a significantly increased number of vessels catheterized (p=0.027) and larger contrast volumes (p=0.022).
Conclusions CE-TR MRA is a useful initial examination for the diagnosis and localization of SDAVFs, with a high concordance rate with DSA. When CE-TR MRA demonstrates a SDAVF, the number of catheterized vessels and contrast dose can be decreased during DSA.
- Fistula
- Magnetic Resonance Angiography
- Spine
- Technique
Statistics from Altmetric.com
Introduction
Spinal vascular malformations represent rare lesions that can be divided into shunting lesions, including spinal arterial venous malformations and spinal dural arterial venous fistulas (SDAVFs), and non-shunting lesions consisting of capillary telangiectasias and cavernous malformations. SDAVFs represent approximately 70% of spinal vascular malformations1 ; however, timely diagnosis can be challenging, with patients frequently misdiagnosed and treated for entities such as spinal canal stenosis from spondyloarthropathy or inflammatory myelitis.2–4 A high degree of clinical suspicion and knowledge of the MRI appearance is critical for guiding appropriate investigation and management.
Catheter-based spinal digital subtraction angiography (DSA) remains the definitive diagnostic technique for evaluation of SDAVFs due to the unsurpassed spatial and temporal resolution of the technique; however, DSA is invasive and not without risks from extensive catheter manipulation. Additionally, the time-consuming procedure of spinal DSA can require general anesthesia, result in a high radiation dose to the patient and require large volumes of iodinated contrast material. Optimal selection of patients for spinal DSA and focusing examinations to limit procedure time, radiation dose and contrast dose is therefore desirable.
MRI has been used successfully to suggest a diagnosis of SDAVF based on T2 hyperintensity in the spinal cord and conus medullaris and associated flow voids.3 ,5 However, the level of T2 hyperintensity is not predictive of the level of the SDAVF.3 ,6 Previous studies have used different MR angiography (MRA) techniques for localization of the arterial supply of SDAVFs with varying success.7–10 More recently, contrast-enhanced time-resolved MR angiography (CE-TR MRA) techniques have shown great potential as non-invasive approaches to probing vascular flow in a temporally sensitive manner. Efforts to rapidly image contrast kinetics have benefited from acquisition schemes aimed at accelerated data collection, primarily using parallel receive algorithms, novel k-space trajectories and incorporation of view-sharing techniques.11–13 The purpose of this study was to determine the utility of spinal CE-TR MRA for evaluation of SDAVFs prior to DSA.
Methods
Patients
Since the spinal CE-TR MRA protocol at our institution was implemented in October 2010, 36 consecutive patients have presented for evaluation through February 2013, 18 of whom had subsequent DSA performed and available for direct comparison. The remaining patients did not undergo DSA. All studies were performed to evaluate for SDAVFs, with indications for the examination consisting of progressive lower extremity motor weakness or sensory symptoms (n=16), non-traumatic spinal subdural hematoma (n=1; patient 9) and spinal cord hematoma (n=1; patient 11). There were 15 men and 3 women of median age 65 years (range 30–80).
CE-TR MRA technique
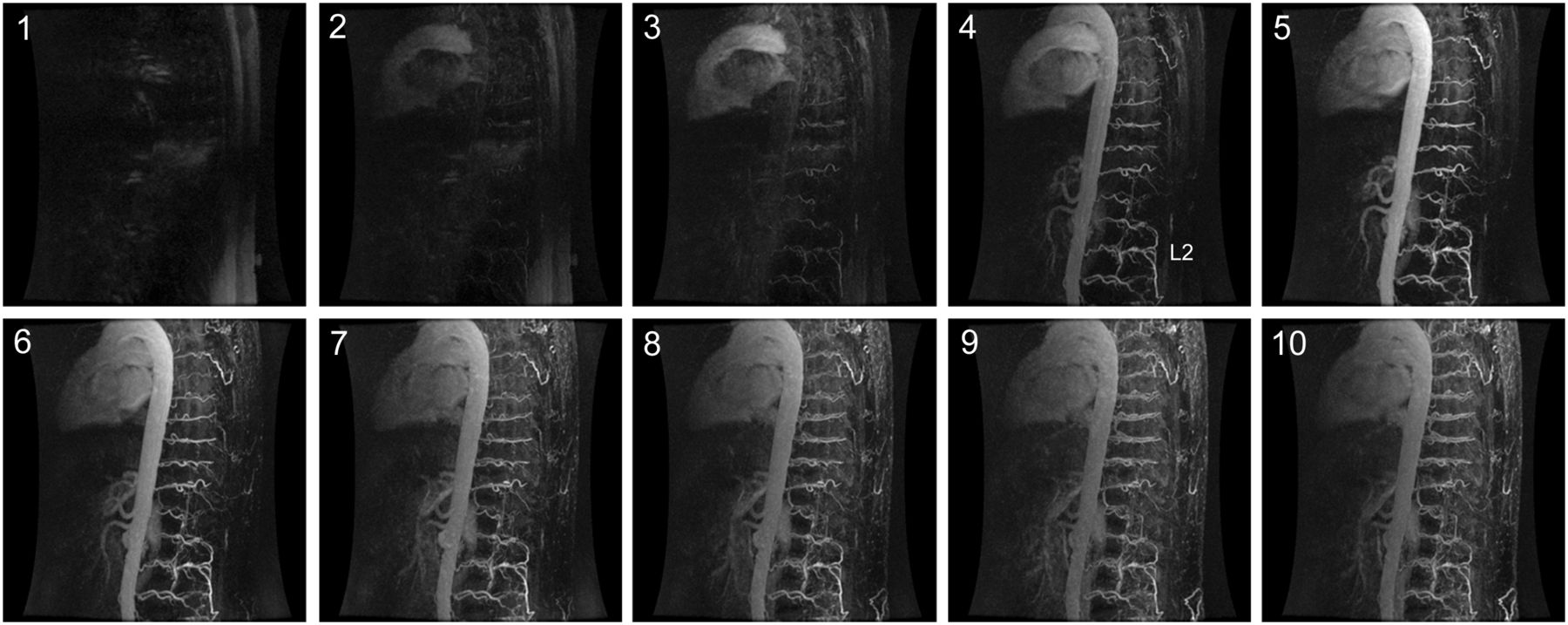
All patients underwent a standardized protocol for CE-TR MRA. Imaging was performed at 1.5 Tesla on a GE Signa HDx unit (Milwaukie, Wisconsin, USA) using body transmit and signal reception with a dedicated 32-channel spine coil. Following localizing sequences, an oblique sagittal plane was chosen for set-up of the Time Resolved Imaging of Contrast Kinetics (TRICKS) CE-TR MRA sequence using a 35 cm field of view extending from approximately the T4 through the L4 vertebral body levels. Specific parameters of TR=2.54, TE=1.97, flip angle=35° were used for this three-dimensional acquisition with a 256×224 matrix resulting in a 1.4×1.2 mm in-plane resolution with 2 mm slice thickness. A pre-contrast mask was acquired, followed by 10 dynamic temporally discrete post-contrast phases at approximately 7 s temporal update during the intravenous injection of a gadolinium-based contrast agent (figure 1).

Dynamic phases acquired during contrast-enhanced time-resolved MR angiography (CE-TR MRA). Ten dynamic phases are acquired with 7 s temporal resolution. The images are from patient 1, demonstrating a spinal dural arterial venous fistula arising from the left L2 segmental artery. The L2 level is indicated in phase 4 of the figure.
Patients underwent injection of either gadobenate dimeglumine (Multihance, Bracco Diagnostics) 0.1 mmol/kg at an injection rate of 2.0 mL/s (n=16) or the blood pool agent gadofosveset trisodium (Ablavar, Lantheus Medical Imaging) 0.03 mmol/kg at an injection rate of 1.5 mL/s (n=3). Bolus infusion in both protocols was followed immediately by 25–30 mL normal saline flush. Background subtraction of a pre-contrast imaging volume was performed in-line during acquisition, allowing for production of both background subtracted and unsubtracted CE-TR MRA volumes as well as cine maximum intensity projection series.
Spinal DSA technique
The angiographic technique included selective manual injections of vessels that were most likely to supply a fistula after correlation with non-invasive imaging. This could include the segmental arteries from the supreme intercostals through the middle sacral artery, bronchial arteries, internal iliac arteries, external carotid arteries, vertebral arteries, thyrocervical trunks and costocervical trunks. Generally, vessels were selected under fluoroscopy starting with the most likely candidates for possible fistula supply, and 3–5 mL of 270 mg/mL iodinated non-ionic contrast agent (Visipaque 270, GE Healthcare) were injected with anteroposterior filming at a rate of 2–3 frames/s. Once a fistula or arteriovenous malformation was identified, angiograms were obtained at adjacent levels in both the cranial and caudad directions until two adjacent normal levels were identified. At that point, no more vessels were imaged and the study was complete. In cases where the CE-TR MRA suggested a specific arterial feeder for a SDAVF, the specific vessel was cathetherized first. In cases where the CE-TR MRA was negative for SDAVF, the spinal DSA was conducted as would normally be performed without prior localizing information with initial catheterization at the levels most likely to correspond to the individual patient's MRI findings.
Image analysis
CE-TR MRA and DSA images were reviewed by an experienced neuroradiologist (AMS) in consensus with a neuroradiology fellow (SRB) without knowledge of the diagnosis. Studies were determined to be of diagnostic or of non-diagnostic quality owing to improper scan initiation resulting in complete venous contamination or excessive patient motion. The CE-TR MRA was then reviewed for the presence or absence of abnormal arterial vascularity that suggested a SDAVF and levels of arterial feeders. The DSA was evaluated for the presence or absence of a SDAVF, as well as levels of arterial feeders. For cases positive for SDAVF, the location of arterial feeders was noted. For all DSA examinations, the number of vascular pedicles arising from the aorta that were catheterized, total iodinated contrast dose, procedure time and fluoroscopic time were recorded.
Statistical analysis
The sensitivity, specificity, positive and negative predictive values for detection of SDAVFs on CE-TR MRA were calculated using DSA as the reference standard. CE-TR MRA studies were classified as being either SDAVF positive or SDAVF negative/non-diagnostic quality. DSA measures of the number of vascular pedicles catheterized, total iodinated contrast dose, procedure time and fluoroscopic time were compared between the SDAVF positive CE-TR MRAs and SDAVF negative/non-diagnostic quality CE-TR MRAs using an independent samples t test for equality of means (SPSS V.20.0.0.1).
Results
Concordance between CE-TR MRA and DSA
For the 18 patients who underwent both CE-TR MRA and DSA, the median time from the CE-TR MRA to the DSA was 11 days (range 0–41). Four of the 18 CE-TR MRA studies were determined to be of non-diagnostic quality owing to improper scan initiation (n=2) or excessive patient motion (n=2) during the early experience with this technique; the remaining 14 CE-TR MRA studies were determined to be of sufficiently good diagnostic quality for confident interpretation. In the four non-diagnostic CE-TR MRA examinations, three did not demonstrate a SDAVF (with confirmation on spinal DSA), while one did not identify a SDAVF that was found on DSA with an arterial supply from the right T12 segmental artery.
Of the 14 patients with diagnostic CE-TR MRA, eight were interpreted as positive for SDAVF, of which seven were concordant with DSA. Figure 2 illustrates representative cases with CE-TR MRA and DSA correlations. One patient that was described as having a prominent right L1 segmental artery but no clear shunting represented a false positive for SDAVF on CE-TR MRA. The six patients who were negative for SDAVF on CE-TR MRA were all also negative on DSA. Including both diagnostic and non-diagnostic quality CE-TR MRA studies, the overall sensitivity, specificity, positive and negative predictive values for detection of SDAVF on CE-TR MRA in comparison with DSA were 88%, 90%, 88% and 90%, respectively. In the seven concordant SDAVFs on CE-TR MRA and DSA, the feeding arteries were within one vertebral level in six cases. In the seventh case a SDAVF was identified on the CE-TR MRA but the feeding artery could not be identified. On DSA, the feeding artery was found to arise from the left internal iliac artery, several centimeters below the field of view for the CE-TR MRA. The results are summarized in table 1.
Concordance of findings of SDAVF on CE-TR MRA and DSA

{kind=link}
{kind=link}
Correlative images between contrast-enhanced time-resolved MR angiography (CE-TR MRA) and digital subtraction angiography (DSA). (A, B) Patient 2 in his/her 60s presenting with lower back pain and lower extremity weakness status after lumbar surgery for spondylosis; (A) demonstrates a spinal dural arterial venous fistula (SDAVF) with apparent supply from the right T11 and T12 segmental levels and (B) shows that the fistula arises from the right L1 level. (C, D) Patient 3 in his/her 70s presenting with progressive lower extremity weakness; CE-TR MRA demonstrates SDAVF arising from the left T8 segmental level (C) and DSA confirms the site of the fistula from the left T8 segmental level (D). (E, F) Patient 4 in his/her 70s presenting with lower extremity weakness; CE-TR MRA shows a SDAVF arising from the left T10 segmental level (E) and DSA shows the fistula actually arising from left T11 (F). (G, H) Patient 5 in his/her 60s with lower back pain and lower extremity weakness; CE-TR MRA shows a SDAVF arising from the right T6 level (G) and DSA confirms a fistula at the right T6 level (H). Additional supply was present from the right T7 level.
Differences in DSA measures between positive and negative/non-diagnostic CE-TR MRA studies
Compared with patients with a non-diagnostic or negative CE-TR MRA for SDAVF, patients with a CE-TR MRA positive for SDAVF had significantly fewer vascular pedicles catheterized (p=0.027) and a significantly lower contrast dose (p=0.022) during their DSA. Two patients (patients 1 and 2) with CE-TR MRAs who were positive for SDAVF underwent combined diagnostic and therapeutic DSA; the specific contrast dose, fluoroscopic time and procedure time for the diagnostic portions of these two examinations could not be accurately ascertained. The results are summarized in table 2.
Comparison of DSA parameters in patients with CE-TR MRA positive for SDAVF and patients with suboptimal or negative CE-TR MRA
Discussion
SDAVFs can pose a challenge for both diagnosis and specific localization. On MRI, SDAVFs are characterized by an increased T2 signal within the spinal cord and conus medullaris which is thought to be related to venous hypertension and resultant cord swelling.3 ,5 This can be associated with enhancement following contrast administration, reflecting breakdown of the blood/spinal cord barrier.14 ,15 The MRI appearance can mimic various other etiologies including inflammatory or infectious myelitis and cord edema from spinal canal stenosis. The location of T2 hyperintensity within the spinal cord does not necessarily localize the site of the SDAVF since the conus is frequently involved due to orthostasis.3 ,6 Flow voids are frequently seen on T2-weighted images within the subarachnoid space in the setting of SDAVFs, representing enlarged and arterialized perimedullary venous channels. These are best seen on heavily T2-weighted myelographic sequences,16 but have also been demonstrated on CT myelography as filling defects in the intrathecal contrast pool.17 These prominent subarachnoid space venous structures are frequently extensively present longitudinally, and thus also do not localize the level of the SDAVF and arterial supply.6
Given the inability of MRI to localize SDAVFs prior to DSA, various non-invasive techniques using both CT angiography (CTA) and MRA have been attempted for this purpose. The large craniocaudal coverage of the spine and small caliber of spinal vessels makes this challenging. Studies using CTA with newer generation CT scanners have shown a modest ability to detect SDAVFs, but with a high dependence on contrast bolus timing and frequently poor differentiation of arterial and venous structures at the expense of considerable radiation exposure.18 Early attempts with non-contrast MRA techniques including phase contrast and time-of-flight showed poor ability to detect SDAVFs.19 ,20 Initial CE MRA studies offered a single phase or limited phases that could not differentiate between arteries and veins and were not able to detect SDAVF arterial feeders with confidence.10
Vargas et al used a MRA protocol with timing determined by an initial test bolus of contrast agent followed by arterial and venous phase acquisitions. The study group consisted of a variety of spinal vascular malformations but included four SDAVFs that were localized accurately.21 More recent studies using elliptic centered reordering of k-space to generate high-resolution CE MRA has shown improved performance. Farb et al used an auto-triggered technique based on a set signal intensity threshold within the aorta in nine patients with suspected DAVF to initiate optimal arterial acquisition from which a baseline acquisition was subtracted. While this technique was able to localize the DAVF in all nine patients, five were initially negative and required repeat MRA to determine the site of the fistula.7 Luetmer et al8 examined 31 patients with a suspected SDAVF using a similar technique, detecting 20 of 22 SDAVFs found on DSA and accurately determining the level of the fistula in 14. Mull et al also used a similar CE MRA technique in 34 patients, of which DSA revealed 20 SDAVFs. The MRA was concordant with DSA for all cases with the feeding artery identified correctly in 14 cases, within one segmental level in five cases, and outside the field of view in one case. The post-processing in this technique, however, was fairly time-consuming and required specific expertise to perform.9
While techniques based on elliptic centric CE MRA are useful for pre-angiographic evaluation, they lack information on contrast kinetics from multiple phases, are reliant on a test bolus or fluoroscopic triggering and may require extensive post-processing. CE-TR techniques including vendor-specific products such as TRICKS use a combination of undersampled k-space trajectories and view sharing to accelerate acquisition, allowing for much higher temporal resolution than traditional bolus-chase MRA techniques while maintaining a high spatial resolution.12 ,22 This provides temporal information and the ability to achieve an uncontaminated arterial phase without dependence on exact contrast bolus timing due to variations in cardiac output and injection rates. In the current study a 7 s temporal resolution was obtained while maintaining sufficient spatial resolution to detect shunting at the level of the radiculomeningeal arteries. The post-processing for this technique was all performed in-line at the scanner using vendor-configured settings.
Early in our experience with the CE-TR MRA technique four cases were non-diagnostic. Two were due to improper initiation of the contrast bolus prior to scanning the pre-contrast mask which resulted in a delayed and entirely venous phase study and oversubtraction of the vasculature since the pre-contrast mask contained vascular enhancement. The other two were related to excessive patient motion resulting from the sensation of contrast injection. Technologist training with regard to the proper administration of contrast and scan initiation and better patient preparation concerning the sensation during injection of the contrast bolus can help to limit these problems. The fact that one SDAVF identified on DSA was not found on CE-TR MRA underscores the importance of optimal technique.
We found a high concordance with DSA for the presence or absence of SDAVFs. All SDAVFs were detected on diagnostic quality CE-TR MRAs; however, one case with a prominent right L1 segmental artery but no definite shunting on CE-TR MRA was still felt to be suspicious for an underlying SDAVF and a DSA was performed demonstrating no abnormality. This was the only false positive case. In six of the seven cases where a SDAVF was correctly detected, CE-TR MRA detected the arterial supply within one segmental level and always on the correct side. The slight variability in levels is probably a limitation of the temporal resolution of the technique, with adjacent vertebral artery levels demonstrating similar enhancement profiles such that a fistula between two levels may be attributed to an adjacent level instead. Because of this limitation, we recommend targeting the level in question by DSA first, but also thorough examination of the segmental artery from the level above and below on the ipsilateral side. In one case a feeding artery on CE-TR MRA was not identified and was ultimately found to arise from the left internal iliac artery far outside our standard field of view. While SDAVFs commonly arise from the thoracic and lumbar segmental arteries, other arterial sources are possible and an exhaustive search by DSA or repeat CE-TR MRA should be performed with a different field of view prior to DSA.
When we were able to identify a SDAVF on CE-TR MRA, the number of vascular pedicles catheterized on DSA could be limited and the contrast dose minimized to far less than that used when no localizing information was present prior to DSA. Our analysis excluded two of the eight CE-TR MRAs positive for SDAVF; a combined diagnostic and therapeutic endovascular procedure was performed or attempted, resulting in a generally longer procedure with more contrast and fluoroscopic time than a solely diagnostic DSA would generate. The ability to plan and perform a simultaneous diagnostic and therapeutic endovascular procedure in selected cases is, in fact, a major potential benefit of performing CE-TR MRA prior to DSA.
There are several limitations to our findings. First, the retrospective nature of this study incorporates a learning curve in both the performance of the technique by technologists and the experience of the readers. During the study period an additional 18 patients did not undergo DSA due to a very low risk of SDAVF or other reasons and had normal MRAs. It is unclear how the technique would fare with all patients or whether false negative cases would arise; however, in the 3-year follow-up period of these patients there has been no indication that a SDAVF was missed. Additionally, our institution is a regional referral center for suspected vascular malformations, and it is unclear whether or not CE-TR MRA would perform similarly in practices with a lower frequency and lower pretest probability of finding a SDAVF. The detection of low-flow vascular pathology may also be limited by the CE-TR MRA technique given the 7 s temporal resolution of the protocol. Newer iterations of the acquisition employing further increases in k-space undersampling and newer reconstruction techniques promise to further improve the temporal resolution. Finally, a disadvantage of this technique is the inability to identify the Adamkievicz artery (AKA) due to limitations in spatial resolution; however, for the purpose of determining the location of the arterial supply of a SDAVF, this becomes less important as the arteries in question will undergo catheterization by DSA to exclude the AKA arising from it to determine the risk of endovascular and surgical treatment.
In conclusion, CE-TR MRA of the spine is a reliable technique for the initial evaluation of suspected SDAVFs, with high concordance with DSA. For cases in which a SDAVF is demonstrated on CE-TR MRA but a definite arterial source is not identified, the source may be outside the field of view. In cases where the CE-TR MRA is able to localize an arterial feeder, the number of catheterized vessels and total contrast dose can be decreased during DSA, with attention to the suspected level ±1 segmental levels. However, if the CE-TR MRA study does not confidently identify an arterial feeder or is of suboptimal quality, a full spinal DSA should be performed.
References
Footnotes
-
An oral abstract of this study was presented at the American Society of Neuroradiology meeting in San Diego, California in May 2013.
-
Contributors AMS initiated the project, was involved in data review and analysis and helped with the construction and review of the manuscript. SRB was involved in data review and analysis and helped with the construction and review of the manuscript. FCT and JED helped with the clinical care of the patients and the construction and review of the manuscript. SD helped with the construction and review of the manuscript. AMS is the guarantor of the paper.
-
Competing interests None.
-
Ethics approval Ethics approval was obtained from the Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.