Article Text

Abstract
Introduction A tandem occlusion is a rare presentation of acute stroke that involves an occlusion of the internal carotid artery at the bifurcation with an intracranial middle cerebral artery occlusion. This study describes the experience at our institution in treating tandem occlusions with a proximal to distal approach in the acute stroke setting.
Methods A retrospective review of acute strokes caused by tandem occlusions requiring thrombectomy were performed.
Results 16 cases were identified with a mean National Institutes of Health Stroke Scale score at presentation of 13.1±3.9. The proximal occlusion was crossed initially with a microwire in all cases. All carotid occlusions were treated with stenting, and intracranial vessel thrombectomy was performed with a variety of devices. Procedure related complications occurred in two (12.5%) patients. Eight patients (50%) achieved a good outcome (modified Rankin Scale score of 0–2).
Conclusions A tandem occlusion of the carotid artery at the bifurcation with a concomitant intracranial occlusion is a relatively rare and complex presentation of acute stroke. We have found that addressing the proximal lesion first and covering it with a stent prior to performing distal thrombectomy appears to be a safe and effective option in the treatment algorithm.
- Stroke
- Thrombectomy
Statistics from Altmetric.com
Introduction
Administration of intravenous tissue plasminogen activator (IV tPA) is the only Food and Drug Administration approved treatment for acute stroke.1 ,2 Those patients that do not have resolution of their symptoms with administration of IV tPA as well as those patients that are not candidates for IV tPA may still benefit from intra-arterial therapy, including mechanical thrombectomy, stent placement, and administration of tPA.3 ,4 The treatment options for endovascular therapy have rapidly evolved over the past few decades.5–13
A tandem occlusion is a rare presentation of acute stroke that involves occlusion of the proximal cervical internal carotid artery (ICA) at the bifurcation with an intracranial middle cerebral artery (MCA) occlusion, although the distal lesion may also involve the anterior cerebral artery (ACA) territory. The underlying pathophysiology involves either atherosclerotic disease or a dissection of the proximal vasculature leading to complete occlusion and an embolus causing a distal tandem occlusion.14 Two approaches exist for the treatment of tandem occlusions, including treating either the proximal occlusion first or the distal occlusion first; however, there is no consensus on which approach is more efficacious.15–22 This study describes the experience at our institution in treating tandem occlusions with a proximal to distal approach in the acute stroke setting.
Methods
This analysis was conducted with institutional review board approval. A retrospective review of the charts and radiologic studies of all acute strokes requiring thrombectomy at our institution from August 2009 to July 2013 was performed.
The endovascular procedures were performed by four neurointerventionalists (two neurosurgeons and two neurointerventional radiologists). All patients underwent non-contrast head CT, CT angiography of the head and neck, and CT perfusion of the head on arrival to the emergency department. Patients deemed to have an arterial occlusion as well as a large area of penumbra were deemed candidates for intervention. Clinical data included age, sex, admission National Institutes of Health Stroke Scale (NIHSS) score, administration of IV tPA prior to endovascular intervention, NIHSS score at discharge, and modified Rankin Scale (mRS) score at 90 days (obtained at the clinic follow-up appointment by a clinician certified in mRS or at latest available clinical follow-up if data collected prior to the 90 day follow-up). Interventional data included time from last known normal examination until the start of the endovascular procedure (defined as the time of placement of the groin sheath), time from the start of the endovascular procedure to resolution of the distal occlusion (defined as the time of the first angiographic run showing recanalization of Thrombolysis in Cerebral Infarction (TICI) 2b or 3), devices employed, and complications.
Endovascular technique
Patients who could not protect their airway on admission were intubated and then brought to the neurointerventional suite. All other patients were brought directly to the neurointerventional suite after undergoing CT/CT angiography/CT perfusion in the emergency department. Patients who were able to cooperate with the procedure remained under conscious sedation whereas those patients who were unable to do so required intubation in the neurointerventional suite. After femoral access was obtained, 1000–2000 units of heparin were administered intravenously, and diagnostic angiography of the vessel of interest was performed. The occlusion was initially crossed with a microwire. Treatment of the proximal occlusion was typically performed with balloon angioplasty and stenting. A loading dose of abciximab (0.25 mg/kg) was administered intra-arterially through the guide catheter at the time of stent deployment. Patients were administered aspirin (325 mg) and clopidogrel (600 mg) via the enteral route (either orally or nasogastrically) at completion of the procedure.
After satisfactory treatment of the proximal carotid occlusion, the guide catheter was advanced distally to attempt distal vessel recanalization via thrombectomy.
Results
Demographics
Sixteen patients from August 2009 to July 2013 underwent treatment of tandem occlusions of the anterior circulation causing acute stroke symptoms (table 1).
Summary of patient demographics, site of occlusion, devices used to cross and treat the occlusion, time to recanalization, and outcome
Eight (50%) patients were men with a mean patient age of 67.8±12.3 years and a mean NIHSS score at presentation of 13.1±3.9. Twelve (75%) patients had tandem occlusions on the right side and four (25%) patients had tandem occlusions on the left side. Twelve patients were found to have two simultaneous occlusions (ICA and MCA) while four patients had three simultaneous occlusions (ICA, MCA, and ACA). Mean time from symptom onset to groin access was 9.9 h±6.2 h. Eight (50%) patients received IV tPA prior to thrombectomy.
Technical considerations
Proximal occlusion
The proximal occlusion was crossed initially with a microwire in all cases. The most commonly employed wire was a 0.014 inch diameter (n=13, 81.3%) followed by a 0.016 inch (n=3, 18.7%).
In the majority of patients (81.3%) a microcatheter was advanced beyond the proximal occlusion over the microwire, after which angiography was performed to confirm the microcatheter was in the true lumen of the carotid artery as well as to confirm the site of the distal occlusion (figure 1A). The microcatheter diameters used ranged from 0165 to 025. Double roadmap imaging was then obtained with injection of contrast simultaneously via the guide and microcatheter (figure 1B). In cases in which a microcatheter was not utilized, the initial device used to cross the proximal occlusion was a balloon catheter (n=1), a stent (n=1), and a Penumbra 026 reperfusion catheter. A distal embolic protection device (SpiderFX; ev3, Irvine, California, USA) was used in five (31.3%) patients prior to treatment of the proximal occlusion. All carotid occlusions were treated with eventual stenting, most commonly angioplasty followed by stenting with post-stenting balloon dilatation as required; however, in one case, the occlusion was treated with stenting alone and in another case the proximal occlusion was treated with angioplasty initially and a stent was placement after successful recanalization of the distal occlusion (figure 1C, D). Balloons used for angioplasty ranged in diameter from 2.5 to 6 mm and in length from 15 to 20 mm. Carotid stents (Precise Pro Rx; Cordis, Bridgewater, New Jersey, USA) were used in diameters ranging from 5 to 10 mm and lengths 30 to 40 mm. Two cases required three stents and one case required two stents to be deployed.
{kind=link}
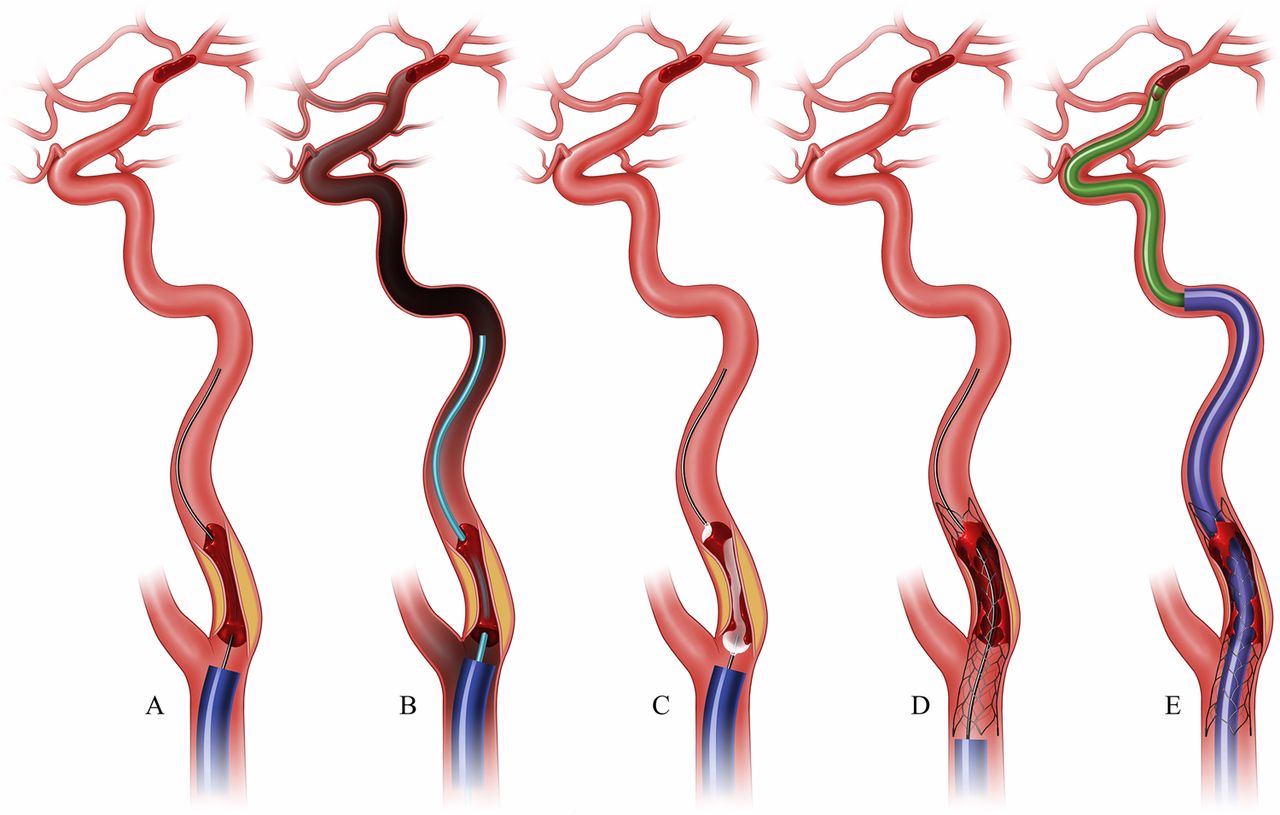
Stepwise illustration of the proximal to distal approach in treating tandem occlusions causing acute stroke. (A) A microcatheter is advanced beyond the proximal occlusion over a microwire, after which angiography is performed to confirm the microcatheter is in the true lumen of the carotid artery. (B) Double roadmap imaging is obtained (injection of contrast simultaneously via the guide and microcatheter). All carotid occlusions were treated with stenting, most commonly balloon angioplasty (C) followed by stenting (D), with post-stenting balloon dilatation as required. (E) Once the proximal occlusion has been addressed, the guide catheter is advanced past the stent into a more distal position along the cervical carotid artery to provide sufficient support for thrombectomy of the tandem intracranial occlusion utilizing the ADAPT technique.
Distal occlusion
Intracranial vessel thrombectomy was performed with a variety of devices: Penumbra reperfusion catheter and separator (n=8), direct aspiration (n=5), and a combination of direct manual aspiration and stent retriever deployment (n=2). In one case, revascularization of the proximal occlusion resulted in spontaneous resolution of the tandem intracranial occlusion.
Recanalization
Successful recanalization of the proximal occlusion was achieved in all patients. Distal occlusion recanalization (TICI 2b or 3) was also achieved in 16 (100%) patients. Mean time from groin access to recanalization of the distal occlusion was 86±39.0 min (range 35–152 min). Recanalization was achieved within 1 h in four patients.
Complications and outcome
Procedure related complications occurred in two (12.5%) patients. One patient suffered a non-flow limiting dissection of the petrous segment of the ICA that was treated with an additional stent and resulted in no clinical sequelae. Another patient had a perforation of the MCA M2 anterior division branch which was treated by advancing a Penumbra 026 reperfusion catheter into the perforated vessel until it was occluded and leaving the catheter in place for 6 min. Nine patients (56.3%) achieved a good outcome (mRS 0–2). In three patients, the family chose to withdraw care after the intervention (one patient suffered a large hemorrhage within the core infarct with intraventricular extension and the other two patients failed to improve neurologically). One patient had an asymptomatic 3 cm×2 cm right parietal hemorrhage seen on routine follow-up CT scan. Seven patients had either a small amount of subarachnoid hemorrhage or a small petechial hemorrhage (<3 mm) within the core infarct on routine follow-up CT scan, all of which were asymptomatic.
Discussion
Tandem occlusions are a relatively uncommon presentation of acute ischemic stroke and involve occlusion of the ICA at the bifurcation and an M1 and/or an A1 occlusion.5 The underlying pathophysiology involves either atherosclerotic disease or a dissection of the proximal vasculature leading to complete occlusion and an embolus causing a distal tandem occlusion.21 While proximal cervical carotid occlusion leads to arrest of anterograde flow, the circle of Willis as well as collaterals from the external to the ICA can still supply perfusion. However, with more distal M1 occlusions, the collateral supply is restricted to the pial collateral circulation, which is not as robust. Thus an acute carotid occlusion may not necessarily become symptomatic until an embolus causes a distal occlusion, which is thought to be the predominant cause of acute symptomatology. The challenge with the tandem occlusion scenario is that the access to the distal lesion is blocked by the proximal occlusion.
Distal–proximal approach
The principle behind a distal–proximal approach is to treat the symptomatic lesion first and restore perfusion to the involved territory, thereby ‘resetting the clock’ on the at risk tissue.17 ,22 Once the distal occlusion has been recanalized, time may be devoted to definitively addressing the proximal occlusion to prevent future embolic events without the time sensitive pressures of the acute stroke setting. However, the major drawback to this approach is that angioplasty and stenting the proximal lesion after recanalization of the distal lesion exposes the patient to the possibility of distal emboli causing a post-treatment intracranial occlusion, necessitating repeat thrombectomy.17 Another drawback is that the untreated carotid lesion can impede distal delivery of the guide catheter to provide support for the devices needed for distal thrombectomy.
Proximal–distal approach
A proximal–distal approach affords benefits that can make the procedure safer and more efficient for the patient.14 First, after the proximal lesion is crossed, balloon angioplasty and stenting can be performed with the added protection against showering of emboli afforded by a tandem occlusion. This can obviate the need for use of an embolic protection device. For example, if the carotid terminus is occluded, we believe distal protection is not required as any potential emboli do not have access to the intracranial circulation. If an M1 occlusion is present and the ACA territory is widely patent, use of an embolic protection device may be considered as additional safety. Second, once the carotid is recanalized, we believe there are additional benefits of thrombolysis afforded by restoration of flow.23 In our experience, one intracranial occlusion was completely recanalized following carotid revascularization without the need for thrombectomy. In other instances, a carotid terminus occlusion converted to a more manageable M1 occlusion.
Tips and tricks
Tandem occlusions can be daunting lesions to treat due to the additional steps and devices required, as well as the time pressures of the acute stroke setting. However, we endorse a methodical stepwise approach that can render these lesions much more simple to conceptualize and address. Adoption of a proximal–distal approach relies on the confidence that the carotid can be recanalized efficiently. In our experience, all proximal lesions were successfully treated with acceptable distal recanalization times to achieve TICI 2b or greater. This may require aggressive attempts to cross the carotid occlusion with a microwire. We have found that a 0.016 inch microwire provides the benefits of additional stiffness to ‘push’ through the occlusion. The wire is given a slight curve, as too much of a curve will cause the microwire to double over on itself when advanced and impede travel through what is often times a relatively long and thin channel of thrombus superimposed on atherosclerotic plaque. Once the proximal lesion is crossed, a microcatheter is delivered over the microwire. Angiography performed through the microcatheter will delineate the intracranial occlusion and allows the creation of a dual simultaneous roadmap image with injections of contrast through the guide and microcatheter to fully demarcate the extent of the proximal occlusion which can ensure that angioplasty and stent deployment adequately address the lesion. Once the stent is deployed across the carotid occlusion, anterograde flow has been restored, and the caliber of the vessel has been sufficiently restored, the guide catheter can be safely advanced through the stent to a more distal position in the cervical or petrous carotid. We encountered no mechanical stent complications related to guide catheter advancement and recommend this to be done in a coaxial or triaxial fashion, when possible, to reduce the ‘lip effect’. Distal delivery of the guide catheter provides additional support for the navigation of large bore catheters past the carotid siphon and ophthalmic artery origin. In addition, it removes the stent from the equation which is especially important in cases that involve multiple passes with thrombectomy devices to be withdrawn into the guide catheter. Once a satisfactory guide catheter position is obtained, we recommend using whatever thrombectomy approach with which the neurointerventionalist is most comfortable. The antiplatelet effect of abciximab likely promotes the maintained patency of the intracranial vessel and reduction of the microembolic burden into the distal vasculature following thrombectomy. However, there is an increased risk of bleeding with the use of abciximab in the setting of recent administration of intravenous or intra-arterial tPA use. Over our experience in treating tandem occlusions included in this report, we employed Penumbra separators, stent retrievers, and direct manual aspiration. The tandem intracranial occlusion was successfully recanalized in every instance.
Conclusion
A tandem occlusion of the carotid artery at the bifurcation with a concomitant intracranial occlusion is a relatively rare and complex presentation of acute stroke. We have found that addressing the proximal lesion first and covering it with a stent prior to performing distal thrombectomy appears to be a safe and effective option in the treatment algorithm of tandem occlusions causing an acute stroke.
References
Footnotes
-
Contributors Each author listed should receive authorship credit based on material contribution to the article, revision of the article, and final approval of the article for submission to this journal.
-
Competing interests RDT, MIC, AST reports grants and non-financial support from Penumbra, Microvention, Covidien, Siemens, Medpace, and Stryker. AMS is consultant to Pulsar Vascular.
-
Ethics approval The study was approved by the institutional review board of the Medical University of South Carolina.
-
Provenance and peer review Not commissioned; externally peer reviewed.