Article Text

Abstract
Object Flow diversion has emerged as a promising treatment alternative for cerebral aneurysms. As a new device, treatment-related events and complications are currently being characterized.
Methods Data on 100 consecutive procedures with the intention to use flow diversion were prospectively collected and analyzed retrospectively.
Results Ninety-five aneurysms were treated in 93 patients during 100 consecutive procedures in which the intention was to treat an intracranial aneurysm with flow diversion. Death occurred in 1% and permanent morbidity in 1%. However, periprocedural technical complications occurred in 35% of the procedures and included proximal device migration in 12%, incomplete device expansion in 9%, catheter-induced vasospasm in 6%, and artery perforation from the wire in 3%. Perioperative clinical events were seen in 28% (thromboembolism and access site complications were the most common, being observed in 6.5% of patients). Worsened extraocular motility was seen in 5.4% and resolved in 4/5 patients. Mean clinical follow-up was 17 months. There were no late clinical or technical issues resulting in permanent deficits, although one patient suffered worsening ataxia. Overall, using very strict angiographic criteria, complete angiographic obliteration was 50% at 6 months and 69% after 1 year.
Conclusions Flow diversion for intracranial aneurysms is a safe and effective treatment. Technical and clinical events are common in the perioperative period. Careful perioperative care and proper management of technical and clinical events encountered is key to achieving low morbidity and mortality. Late clinical events can occur but are unlikely to result in permanent complications.
- Aneurysm
- Flow Diverter
Statistics from Altmetric.com
Introduction
The introduction of flow diverters has heralded a new era in the endovascular treatment of intracranial aneurysms.1 ,2 Previously published case series have detailed the efficacy of flow diversion and have focused on major complications and short-term angiographic outcomes,3–9 but relatively minor technical or clinical events have received little attention. In this report we detail our experience with 100 consecutive procedures, with special emphasis on early and late technical and clinical events.
Materials and methods
Data regarding consecutive procedures in which the intention was to use the Pipeline Embolization Device (intention-to treat) (PED; ev3, Irvine, California, USA) were prospectively recorded. Information collected included patient demographics, aneurysm characteristics, treatment characteristics, number of devices used, intraprocedural and periprocedural technical events (including device deployment, detachment or migration events, perioperative vasospasm, or inability to access the target), clinical events (including aneurysm perforation, thrombosis, neurological symptoms, medical symptoms, ophthalmological symptoms, or wound issues), late technical and clinical events (including any subsequent device migrations, thrombosis, new neurologic changes, late medical complications) at clinical follow-up. Any technical unexpected event and any clinical event potentially related to the procedure and/or the device were considered. The periprocedural period was defined as the 30 days following a procedure, with events following this considered late. Clinical follow-up after discharge was done by a specialized neurosurgery nurse not directly involved in the procedure. Clinical follow-up was collected by telephone within the first 30 days, at the time of the radiographic follow-up at 6 and 12 months and 3 years, and by telephone at 24 months. Radiological follow-up with catheter angiography was recommended after 6 months, 12 months, and 3 years in the early phase of the experience, after which patients were recommended to have either 6-month or 12-month angiography. Any angiographic filling of the aneurysm was considered as incomplete filling.
The periprocedural pharmacological protocol was uniform throughout the study period. Patients were recommended to start clopidogrel (Plavix; Bristol-Meyers-Squibb, New York, USA) 75 mg and aspirin 325 mg daily for 5 days before the procedure. Postoperatively, patients were maintained on the same clopidogrel and aspirin doses for 3 months. After 3 months, clopidogrel was discontinued for patients undergoing ‘on-label’ treatment (ie, aneurysms of the internal carotid artery (ICA) proximal to the take-off of the posterior communicating artery). In on-label cases, we have adhered to the minimum length of dual antiplatelet therapy suggested in the Pipeline for Uncoilable or Failed Aneurysms (PUFS) trial.9 For non on-label cases, and especially in high-risk locations, we have continued antiplatelet therapy for longer periods of time due to a supposed higher risk of thromboembolic events. Patients with aneurysms distal to the origin of the posterior communicating artery or involving the posterior circulation were usually maintained on clopidogrel for a longer period of time and the antiplatelet therapy was recommended according to the results of their follow-up catheter angiography. After discontinuation of clopidogrel, patients were recommended to stay on low-dose aspirin (81 mg/day) indefinitely. Loading doses of clopidogrel and aspirin were given on the day prior to or the day of the procedure for patients who were not electively admitted. Platelet reactivity was not tested in any patient.
Treatment took place with at least two of the three senior authors present for each procedure. Patients with subarachnoid hemorrhage were treated with flow diversion after a minimum of 3 weeks. This time period allowed for recovery from the effects of the acute hemorrhage and diminished the likelihood of needing an additional surgical procedure such as ventriculoperitoneal shunting. Once the treatment had started, an introducer sheath was placed and patients were administered a bolus of intravenous heparin to maintain the activated clotting time between 250 and 300 s. At the end of the procedure the heparin was usually reversed with protamine sulfate. A coaxial system was preferred. After placement of a guide catheter on the target vessel, the aneurysm was crossed with the Marksman microcatheter (ev3) over either a Transcend or a Synchro 2 micro guidewire (both Boston Scientific, Natick, Massachusetts, USA). Patients were examined by the treating physicians or a study nurse immediately after the procedure and before discharge. In one case the aneurysm was coiled directly before PED placement.
Simple statistical comparison of the number of devices used was done with the paired Student t test and performed in Microsoft Excel (Microsoft, Redmond, Washington, USA).
Results
In the period under study (May 2009 to April 2013), 100 consecutive procedures were recommended for treatment of 93 patients with 95 target aneurysms. Five patients underwent two separate procedures and two patients had bilateral procedures. Demographic and aneurysm characteristics are listed in table S1 in online supplement 2 and aneurysm location is summarized in table S2 in online supplement 2.
Staged treatment (coiling first followed by PED placement) was planned in 15 patients with very large or giant aneurysms or ruptured aneurysms. Another 15 patients had PED placement for aneurysm recurrence from a previously coiled aneurysm. In 51 aneurysms a single device was used (mean number of devices 1.5, range 1–10). With more experience, significantly fewer devices were used in the second half of the analysis, with a mean of 2.0±1.6 devices used from May 2009 to September 2011 and 1.2±0.5 devices from October 2011 to April 2013 (p=0.0069). Fifty-nine of the procedures were for ‘on label’ indications and 41 for ‘off label’ indications. There were no statistically significant differences in complication rates between the two groups.
Periprocedural technical events
Technical failure (no device deployed and/or premature procedure completion) occurred in six procedures (6%) (see table S3 in online supplement 2). The reasons included wire perforation (two cases), inability to cross the aneurysm with the microguidewire (two cases), inability to cross a pre-existing stent (one case), and excessive vessel tortuosity (one case). In these six patients the aneurysm was treated in a separate procedure with ICA sacrifice in two, coiling in one, and flow diverter in one (re-access with a triaxial system resulted in successful procedure on the second attempt). In two patients no further treatment was offered and both patients remain stable at follow-up.
Periprocedural technical events occurred in 35 (35%) of the 100 procedures and are summarized in table 1. Although common, these technical issues did not result in any permanent clinical complication. Proximal device migration from the intended target distal segment of the vessel after or during deployment was the most frequent technical issue, occurring in 12% of procedures. Incomplete initial expansion of the device during deployment occurred in 9% (two of these patients were treated with balloon angioplasty; see figure S1 in online supplement 1). In the remaining seven patients, simple mechanical manipulation by pushing the microcatheter over the delivery wire resulted in adequate expansion of the device. Catheter-induced vasospasm with transient distal flow limitation was seen in 6% of the procedures and resolved in all patients.
Periprocedural technical events among 100 consecutive procedures
Three patients suffered a wire perforation which resulted in subarachnoid hemorrhage in one patient, a contained asymptomatic neck very small hematoma in one patient, and an asymptomatic carotid–cavernous fistula in the remaining patient. No patient had any permanent effects.
Periprocedural clinical events
Periprocedural clinical events are listed in table 2. Periprocedural events resulted in death in one patient (1%) (figure 1) and minor permanent morbidity in another patient (1%). Overall, periprocedural thromboembolic complications occurred in 6/93 patients (6.5%). One patient with a ruptured ICA ‘blister-like’ aneurysm was noted clinically to have a dominant premotor area stroke the day following the procedure. An urgent CT did not show any hypodensity but the clinical symptoms were unequivocally localized to the left premotor area. The patient suffered a fatal hemorrhagic transformation after being given a heparin bolus during catheter angiography done to rule out thromboembolic complications (figure 1). In four patients an intraprocedural large vessel occlusion was noted at the termination of the procedure during a final control angiogram in three cases (opercular middle cerebral artery branch occlusion in two, posterior cerebral artery and basilar summit occlusion in one) which were successfully treated with abciximab (ReoPro, Eli Lily, Indianapolis, Indiana, USA).10 In the fourth case dysarthria was noted upon extubation and an immediate angiography revealed an ipsilateral posterior inferior cerebellar artery occlusion which was similarly treated with intra-arterial abciximab. None of these patients suffered any clinical sequelae. A transient neurologic deficit (speech impairment) occurred in one patient 1 week after repeat PED embolization for a recurrent giant aneurysm (see figure S2 in online supplement 3). This was treated with intravenous heparin and a subsequent short course of warfarin anticoagulation in addition to dual antiplatelet therapy. MRI showed small embolic diffusion-weighted imaging lesions in the left frontotemporal area (see figure S2 in online supplement 3). There were no cases of delayed aneurysm rupture in this series.
Periprocedural clinical events in 93 patients
{kind=link}
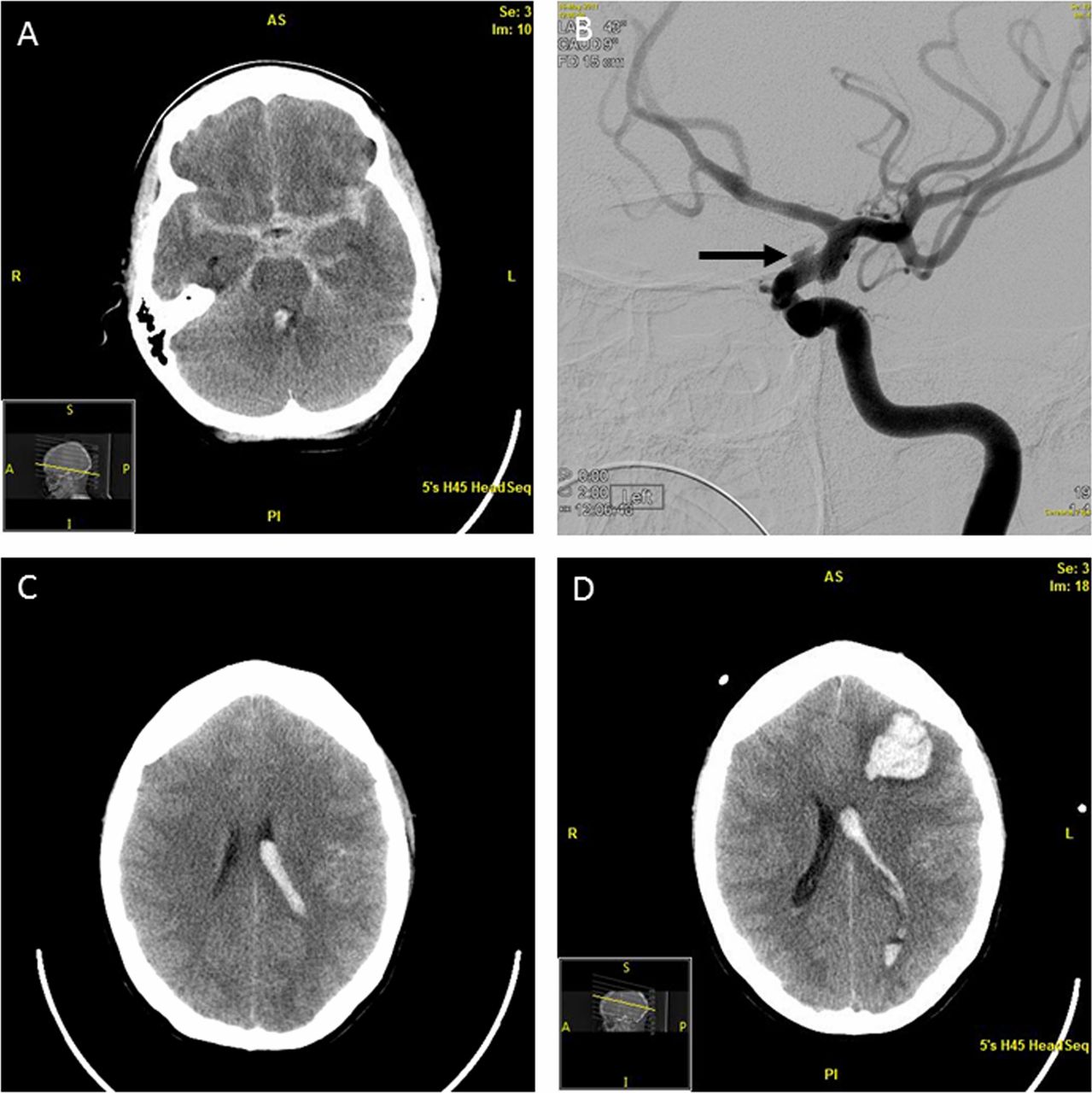
Non-contrast head CT with diffuse subarachnoid hemorrhage (A) from a left dorsal internal carotid artery blister aneurysm (B) (black arrow) which was treated with flow diversion. On postoperative day 1 the patient was noted to have symptoms consistent with a dominant frontal premotor stroke. A head CT done on the same day did not show early evidence of ischemia (C). Head CT on postoperative day 2 shows an ipsilateral parenchymal hemorrhage distal to the target aneurysm (D).
In the first week after the procedure, five patients (5.4%) had new (two patients) or worsening (three cases) extraocular motility deficits. These were transient in four patients. One patient was left with persistent up-gaze limitation 1 year later. This patient is the only one to have suffered a permanent neurologic worsening due to flow diverter placement in this series.
Groin access complications were seen in six patients (6.5%). These included two patients with superficial infections. Three patients had femoral pseudoaneurysms requiring local thrombin injection and one patient required surgical exploration of their arteriotomy.
Two patients experienced transient neurologic deficits with no imaging correlations. One patient experienced an isolated seizure which was treated medically. Three patients experienced medical events periprocedurally which included severe nausea and vomiting, urinary retention, and tongue laceration. Steroids were not routinely administered in this series for pain or discomfort in the postoperative period.
Late technical and clinical events
Mean clinical follow-up was 17 months (range 1–36 months, with minimum 1 month clinical follow-up). No patients were lost to clinical follow-up, but some refused to undergo further imaging. Late clinical events in the 92 surviving patients are listed in table S4 in online supplement 2. All but one of these events was transient. One patient with a giant vertebrobasilar junction aneurysm arising from a fenestration suffered permanent worsening of ataxia after additional coiling of a residual expanding portion of the aneurysm filling from the contralateral arm of the fenestration. This procedure was performed 9 months after flow diversion.
Two patients suffered from definite (one case) or possible (one case) amaurosis fugax 22 and 6 months after the procedure, respectively. Both of these resolved with resumption of antiplatelet therapy. A further patient was found to have an asymptomatic infarct on follow-up MRI. One patient had symptoms of contralateral leg weakness with no areas of restricted diffusion on MRI. Three patients experienced bleeding events related to antiplatelet therapy and two patients were found to have asymptomatic carotid occlusion on follow-up angiography.
Late technical complications were uncommon and are listed in table S5 in online supplement 2. These consisted of device migration requiring retreatment in two patients. In one case, device migration resulted in symptomatic recurrence and further growth of a giant aneurysm which was successfully retreated with urgent placement of additional flow diverters across the recurrent aneurysm neck (see figure S2 in online supplement 3).
Angiographic results
Of the 92 eligible patients, 79 had undergone at least one catheter angiography either at 6 or 12 months. Three patients refused (MR angiography was available in one) and 10 were treated within a few months before data analysis. Using very strict angiographic criteria, overall rates of complete angiographic obliteration were 50% at 6 months and 69% after 1 year. Inadequate coverage of the distal aneurysm neck portion due to proximal migration during, immediately after deployment, or delayed was the reason for incomplete occlusion at follow-up requiring placement of an additional device in six patients.
Discussion
In a consecutive prospective unselected series of 100 consecutive flow diversion procedures we encountered very low permanent morbidity (1%) and mortality (1%); however, we noted high rates of periprocedural technical events and transient clinical events, both of which occurred in about one-third of our procedures. The most common technical events were treatment failures due to difficulty accessing the aneurysm, device migration, incomplete device expansion or deployment, catheter-related vasospasm, and wire perforation. The most common clinical events were periprocedural thrombosis, worsened ophthalmoparesis, and groin access complications. We did not see a trend toward fewer complications over time. While this may have been expected as the learning curve was surmounted, this improved technical proficiency took place during increased use of the device for off-label purposes. Overall, these findings suggest that, while overall outcomes with flow diversion can be excellent, operators should be aware of and prepared to manage technical issues and clinical events related to flow diversion treatment.
Periprocedural and late clinical events
The most feared complications associated with flow diversion are delayed aneurysm rupture and distal intraparenchymal hemorrhage not related to aneurysm rupture.11–13 These complications are typically observed within the first week after deployment of the device and are particularly feared because they are unpredictable. Delayed aneurysm rupture has been observed primarily in very large and giant symptomatic aneurysms.14 The incidence of aneurysm rupture has been reported to be between 0.4% and 2.6% in large series and 3% in a meta-analysis of published cases.6 ,15 ,16 In an attempt to decrease the incidence of this complication, some authors have suggested placing coils to reduce the amount of clot burden after placement of the flow diverter.15 ,17 In our series we did not encounter such a complication. This may be in part related to our use of coils in association with flow diversion for those very large and giant symptomatic aneurysms which we felt could have been at risk of this complication. The absence of delayed ruptures in our series may be related to the low power of our study to detect such complications, given the low number of giant and very large symptomatic aneurysms relative to other series.4–9
Distal parenchymal hemorrhages seem to be a peculiarity of this type of treatment and continue to be poorly understood.18–20 We have encountered one such event (figure 1). However, in our patient there were several other factors besides the flow diverter itself which may have accounted for this catastrophic complication. This includes the fact that the patient had an evolving clinical infarct which was localized to the area of the eventual hemorrhage and to the temporal relationship with a heparin bolus which was administered during a diagnostic catheter angiography as the patient had a known—but, at that time, undefined—procoagulable state. The incidence of distal hemorrhage is reported to be 0.8–8.5%, and 3% in meta-analysis.6 ,16 ,21 Hemorrhage may be related to the actual flow-diverting effect in the setting of dual antiplatelet therapy, to hemorrhagic transformation of small ischemic strokes in the setting of dual antiplatelet therapy, or to unrecognized factors. The low incidence of distal intraparenchymal hemorrhages in our series may be related to our uniform antiplatelet regimen without testing (and therefore without adjusting antiplatelet therapy to the result of the sensitivity test). Patients were maintained on aspirin and clopidogrel for 5 days before the procedure while anticoagulation was usually maintained only throughout the endovascular procedure and the heparin reversed immediately at the end of the procedure. Our experience is similar to that of other groups who have experienced a very low incidence of hemorrhagic complications with a similar uniform antiplatelet therapy and no testing.22 ,23 However, testing of the platelet response is controversial without uniform standard of care at this stage.
Thromboembolic complications with flow diverters may be lower than are observed with traditional intracranial stents. We have observed immediate thromboembolic complications in 6.5% of patients, and these were often promptly reversed with abciximab administration.10 The incidence of thromboembolic complications after discontinuation of antiplatelet therapy seems to be very low, but we have had occasional patients who suffered episodes of amaurosis fugax as late as 22 months after the original procedure. Long-term surveillance is therefore of paramount importance, but the incidence of delayed thromboembolic complications is likely low.
Access site complications were observed in 6.5% in this series. This is at the higher end of the incidence usually observed during neuroendovascular procedures.24 We ascribe this higher incidence, which has also been reported by others,25 to the poor quality of the vasculature, especially in patients with intracranial proximal ICA dysplastic aneurysms, and on the dual antiplatelet therapy and heparinization.26 Since the occurrence of these infections, we now suture the small femoral incision in case of persistent oozing after manual pressure.
Periprocedural and late technical events
Despite the overall good results, many of these procedures were characterized by technical events as shown in table 1. Although these devices have been available for a few years, several unresolved technical issues persist and the incidence of technical complications has not decreased over the course of our series. Periprocedural technical issues were noted in 35% of procedures. The more common ones were related to device migration which can occur in a delayed fashion (as also reported by others27) or, more commonly, intraprocedurally. The inability to adequately control the landing proximal and distal zone of the device is undoubtedly one of the main shortcomings of the PED device as currently designed. It is possible that, with further improvement of this technology, the incidence of these events can be decreased. In our series, several aneurysms remained incompletely covered after deployment of the first device due to its proximal migration during or immediately after deployment. In some of these cases we were able to immediately place an additional device distally. Other times, if placement of a second device was in anyway complicated or not straightforward or in situations where we did not want to further increase the duration of the procedure (and possibly the risk of complications), we elected to consider placement of an additional device at a later time if aneurysm filling persisted at follow-up. Except for the case illustrated of proximal device migration, there were no major clinical complications associated with placement of an additional device either in the same or in a separate session. The inability to predict exactly the landing zone resulted in additional costs (related to additional procedures and/or devices). In order to minimize this untoward event, we have learned to begin unsheathing the distal aspect of the device more distally and to allow more room for the entire system to shift proximally upon deployment.
After device migration, incomplete expansion of the devices was the most common periprocedural technical issue. Interestingly, in several cases in which the device did not expand completely, full expansion followed from the friction of the microguide wire while advancing the angioplasty balloon or during the ‘recapture’ of the delivery coil after device deployment. Adequate apposition and expansion of the device is important to prevent delayed stenosis within the PED or the development of ‘endoleaks’. The incidence of delayed ICA occlusion was low but not negligible, occurring in two patients. These were both asymptomatic and discovered during routine 6-month follow-up. We did not observe delayed symptomatic vessel occlusions and we have discussed the issue of covering vessels such as the ophthalmic artery with a rich collateral supply in a separate publication.28
Our series has limitations. It is a single-center experience and, although we included every patient with intracranial aneurysms treated with flow diversion during the period under study, there was undoubtedly some degree of selection. However, the procedures were performed following a relative uniform protocol and philosophy throughout the period under study. It is possible that we may have failed to capture some outcome measures, but it is unlikely that important clinical outcomes were missed since no patient was lost to clinical follow-up during the period under study. We did not collect information about costs and (given the current socioeconomic environment), this information will be important to assess the role of these devices in the treatment of intracranial aneurysms. In the past we have reported on the changes induced by flow diverters in the ophthalmic artery flow,28 but in the current study we did not collect data regarding hemodynamic changes induced by flow diverters. We feel that these hemodynamic changes, including lack of angiographic visualization and even occlusion of side branches covered by the flow diverter, occur in the presence of significant collateral flow and, to some extent, are part of the flow-diverting effect of the devices. As long as these hemodynamic and angiographic changes remained asymptomatic, we did not feel it was indicated to provide a detailed description. However, longer term follow-up is paramount to understand whether such changes can have long-term clinical effects.
Conclusion
Flow diversion for intracranial aneurysms is a safe and effective treatment. Technical and clinical events are common in the perioperative period. Low morbidity and mortality can be achieved with compulsive perioperative care and close patient follow-up.
Acknowledgments
Sherry Kallies provided editorial and administrative assistance during manuscript preparation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors AMB collected, cleaned, and analyzed the data, drafted the manuscript, and revised the manuscript. HC and DFK collected the data, interpreted the results, and drafted and revised the manuscript. GL formulated the study, collected the data, analyzed and interpreted the data, and participated in the drafting and revision of the manuscript.
Competing interests GL: Consultant, Covidien. DFK: Consulting and grant funding, Covidien.
Ethics approval Mayo Clinic Insitutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.