Article Text

Abstract
Introduction The use of mechanical thrombectomy for the treatment of acute ischemic stroke has significantly advanced over the last 5 years. Few data are available comparing the cost and clinical and angiographic outcomes associated with available techniques. The aim of this study is to compare the cost and efficacy of current endovascular stroke therapies.
Methods A single-center retrospective review was performed of the medical record and hospital financial database of all ischemic stroke cases admitted from 2009 to 2013. Three discrete treatment methodologies used during this time were compared: traditional Penumbra System (PS), stent retriever with local aspiration (SRLA) and A Direct Aspiration first Pass Technique (ADAPT). Statistical analyses of clinical and angiographic outcomes and costs for each group were performed.
Results 222 patients (45% men) underwent mechanical thrombectomy. Successful revascularization was defined as Thrombolysis In Cerebral Infarction (TICI) 2b/3 flow, which was achieved in 79% of cases with PS, 83% of cases with SRLA, and 95% of cases with ADAPT. The average total cost of hospitalization for patients was $51 599 with PS, $54 700 with SRLA, and $33 611 with ADAPT (p<0.0001). Average times to recanalization were 88 min with PS, 47 min with SRLA, and 37 min with ADAPT (p<0.0001). Similar rates of good functional outcomes were seen in the three groups (PS 36% vs SRLA 43% vs ADAPT 47%; p=0.4).
Conclusions The ADAPT technique represents the most technically successful yet cost-effective approach to revascularization of large vessel intracranial occlusions.
- Stroke
Statistics from Altmetric.com
Introduction
Stroke remains a leading cause of death and disability in the USA, with approximately 795 000 strokes occurring per year resulting in 130 000 deaths annually.1 ,2 The overall healthcare costs of strokes approach $40 billion annually.1 The direct costs of stroke were $28.3 billion in 2010 and are projected to nearly double by 2020, reaching $95.6 billion by 2030.1 Direct costs are defined as the total annual medical spending by insurers and out-of-pocket expenses by individuals. Loss of productivity through morbidity or premature morbidity are considered indirect costs and were found to be $25.4 billion in 2010 and projected to reach $42.8 billion by 2030.
The methodology of endovascular treatment for acute ischemic stroke has continued to evolve and improve over the last decade, as evidenced by the evolution and iteration of mechanical stroke devices.3 The latest thrombectomy devices and techniques have significantly improved the rates and speed of vessel revascularization, but with an unclear impact on outcomes.4–8 The impact of these advancements will likely be most apparent initially in direct costs on the healthcare system, but will evolve over time to impact indirect costs as well.
Limited data exist on the routine application of these devices with regard to overall procedure costs, device costs, acute hospitalization costs, time to vessel recanalization, and patient outcomes. The aim of this study is to compare the cost and efficacy of endovascular stroke therapies—more specifically, the various mechanical thrombectomy and adjuvant devices and techniques used during endovascular therapy of patients with ischemic stroke.
Methods
Under an Institutional Review Board approved protocol, a retrospective chart review from January 2009 through December 2013 was performed from the electronic medical record and hospital financial database of the Medical University of South Carolina (MUSC) of all patients with acute ischemic stroke who were treated with endovascular therapy. In accordance with the MUSC acute ischemic stroke protocol, all patients were evaluated for potential endovascular therapy based on CT perfusion imaging irrespective of time of symptom onset, as published previously.9 This analysis included all endovascularly treated patients with ischemic stroke (n=222). The procedures were categorized by the principal thrombectomy device(s) used. Outcome measures included functional (good neurological outcome) and angiographic outcomes (procedural success) as well as procedural and hospital costs.
Documented patient characteristics include age, gender, National Institute of Health Stroke Scale (NIHSS) score at presentation, time to presentation from last known normal, and modified Rankin Score (mRS) at 90 days or closest follow-up period to 90 days. mRS data were obtained from the Stroke Neurology clinic record. Radiological and angiographic imaging was reviewed to document location of vascular occlusion, recanalization time, Thrombolysis In Cerebral Infarction (TICI) flow pre- and post-procedure, and procedural complications. Device efficacy was ultimately evaluated based on restored flow post-procedure, based on a TICI score of 2b or 3 and the absence of periprocedural complications. Procedure-related complications were documented and separated by device group. Clinically significant complications (including procedure-related), including symptomatic intracranial hemorrhage, were also documented per device group. The use of general anesthesia or conscious sedation during the thrombectomy procedure was documented.
Device cost was defined as the cost of all devices used during the procedure including femoral sheaths, contrast, procedural medications including intra-arterial thrombolytics and platelet aggregation inhibitors, guidewires, and catheters. In order to standardize price changes across different years, the advertised manufacturer suggested retail price as of 2013 was used in determining the overall cost for all devices. Hospital length of stay (LOS) was defined as the date of admission for the acute stroke until the patient was discharged from the hospital to home, rehabilitation facility, or other assisted living facility. Direct and indirect hospital costs were those associated with the patient’s admission. If a procedural complication such as a vessel dissection was encountered, the cost to treat the complication was also included in the overall cost analysis.
Hospital metrics were extracted from the hospital financial database to determine the actual LOS and direct and indirect costs for the hospitalization. Direct costs were the costs ‘directly’ associated with patient care/procedures and included any surgeries, nursing care, medications, imaging, and equipment costs. Indirect costs were all other projected indirect costs such as utilities, human resources, maintenance, legal and insurance coverage. The total cost is the sum of the direct and indirect costs.
The three procedure types were categorized by the primary mechanical thrombectomy device used: (1) traditional Penumbra aspiration system with separator (PS; Penumbra, Alameda, California, USA); (2) stent retriever with local aspiration (SRLA); and (3) A Direct Aspiration first Pass Technique (ADAPT).10 The method and approach of thrombectomy was always determined using the newest generation of devices available. When stent retrievers became commercially available, our thrombectomy method completely switched from PS to SRLA. Similarly, when trackable large-bore aspiration catheters became available and the ADAPT technique was discovered, our method of thrombectomy completely switched.
The PS group included cases in which thrombectomy was achieved with Penumbra aspiration system catheters and separators of any size and combination. The technical details of the Penumbra aspiration system have been described in detail elsewhere.11 The general treatment approach for Penumbra aspiration system catheter sizing was to choose the largest size catheter that would fit within the occluded vessel. If fragmentation of the clot occurred into downstream smaller vessels, additional small aspiration catheters were often required. If there was failure to recanalize the target artery, additional adjunctive devices such as balloons, stents, or any other adjuvant devices in addition to the Penumbra aspiration system were used. When stent retrievers became commercially available, the SRLA technique was used and has been previously described. This technique uses a large-bore aspiration catheter; usually Penumbra 054 was advanced to the face of the thrombus and either a Solitaire (Covidien, Plymouth, Minnesota, USA) or Trevo (Trevo Pro, Stryker Neurovascular, Kalamazoo, Michigan, USA) stent retriever was deployed across the occlusion.12 The stent retriever was then removed while local aspiration was applied to the aspiration catheter, which remained in place. When new large-bore trackable aspiration catheters became available, the ADAPT technique was created and has been previously described. This approach to thrombectomy involves the use of a large-bore aspiration catheter alone for thrombectomy.10 In case of failure, the catheter can then be used as a local aspiration platform for a stent retriever, as described with SRLA.
Statistical analysis
Statistical analyses were performed using SAS V.9.3 (SAS Institute, Cary, North Carolina, USA). A population of 222 subjects was analyzed to characterize the differences in cost, functional outcomes, and LOS between the three treatments. Descriptive statistics were calculated for patient demographics, clinical variables, and clinical outcomes. Differences between the three groups were tested using analysis of variance (ANOVA) for continuous measures and a χ2 test for categorical measures. Differences between groups were tested using the Fisher exact test for categorical measures with expected cell sizes <5. Pairwise comparisons for differences between two of the groups were made using the Student t test. All tests were assessed at a significance level of 0.05.
Results
Patients
In the study period 222 patients underwent an endovascular procedure for acute ischemic stroke. The average age was 69 years, with 55% women. The median NIHSS score was 17 and did not differ between the treatment groups (p=0.8). As shown in table 1, there were no significant differences between stroke severity at presentation, age, gender, or administration of intravenous tissue plasminogen activator prior to endovascular treatment.
Patient data
Technical success
Of the 222 cases studied, 128 (58%) underwent PS, 30 (13%) underwent SRLA, and 64 (29%) underwent ADAPT. The PS technique was successful as the only thrombectomy device used in 42% of cases; the remaining cases required other devices such as balloons or stents to achieve final TICI 2b/3 recanalization in 79%. The SRLA technique was successful as the primary method of recanalization in 80% of cases with the remainder requiring aspiration thrombectomy, stents, or balloon maceration to achieve final TICI 2b/3 recanalization in 83% of cases. ADAPT was successful with aspiration alone in 78% of cases and ultimately 95% when stent retrievers were added. Thrombus location was documented for each of the 222 cases; 90.1% of all cases investigated involved an anterior circulation occlusion and 9.9% of cases involved the posterior circulation. Occlusion of the middle cerebral artery was the most common location (76.6%) followed by the internal carotid artery (13.5%) and the basilar artery (8.2%). There were 23 tandem stenoses involving the cervical carotid and intracranial vasculature (11 PS, 3 SRLA, 9 ADAPT). General anesthesia was used in 100% of the PS group, 90% of the SRLA group, and 15.6% of the ADAPT group.
Successful revascularization, defined as TICI score of 2b or 3, was significantly different between the three groups (p=0.0059). The proportion of TICI 2b/3 in the ADAPT group (95%) was significantly higher (p=0.0027) than in the PS group (73%). Across the study, subjects achieving TICI 2b/3 had a higher rate of good outcome, defined as mRS 0–2 at 90 days, than those achieving TICI 0–2a (45.5% vs 15.2%, p=0.0012).
When complete revascularization alone was compared, there was a significant difference between the groups with the ADAPT group achieving TICI 3 in 64% of patients, SRLA in 54%, and PS in 25% (p<0.0001). There was a significant difference in the time required to revascularization (87.7 min for the PS group vs 46.8 min for the SRLA group and 37.1 min for the ADAPT group; p<0.0001).
Clinical outcomes
Clinical outcomes with good neurologic function at 90 days, as defined by mRS score <2, were not significantly different between the groups (36% for the PS group vs 43% for the SRLA group vs 47% for the ADAPT group; p=0.4). When considering only those patients in whom the primary device alone was successful in achieving TICI 2b/3 revacularization, the proportion of patients with mRS 0–2 was 50% with PS, 50% with SRLA, and 54.6% with ADAPT (p=0.89). The average LOS of these patients when the primary device was successful was 10.7 days for PS, 9.7 days for SRLA, and 7.2 days for ADAPT (p=0.15). The correlation between TICI 2b/3 and mRS outcome as an ordinal variable was −0.3, which suggests low correlation. The percentage of patients achieving mRS 0–2 at 90 days who were not successfully revascularized was significantly lower than the percentage of patients who achieved mRS 3–6 who were not revascularized (6% vs 24%, p=0.0012).
Cost analysis
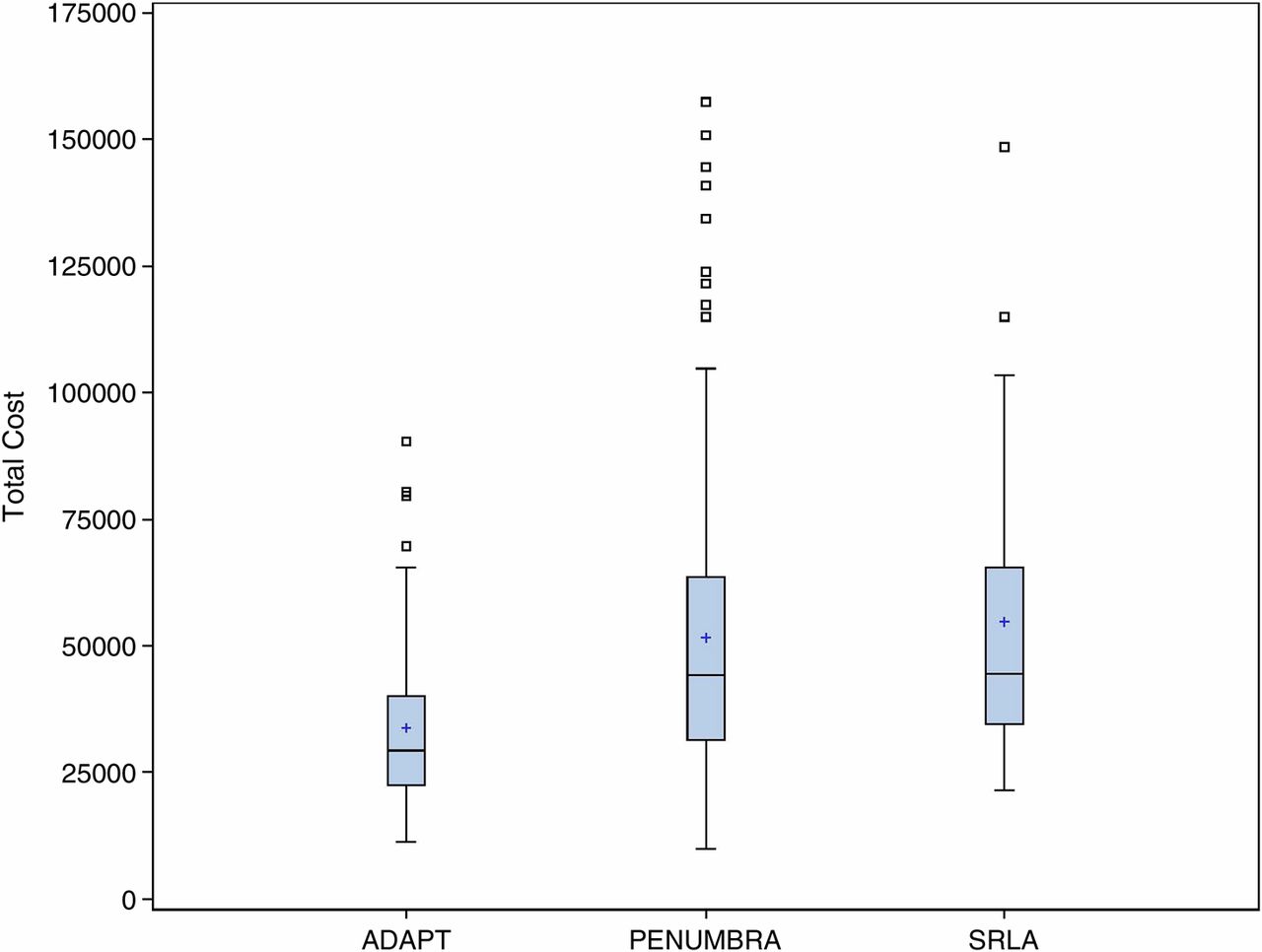
The average LOS was 10.6 days for the PS group, 8.3 for the SRLA group, and 7.0 days for the ADAPT group. The average total cost for subjects in the ADAPT group was significantly lower than both the PS group (p <0.0001) and the SRLA group (p=0.0008). The average total cost for these patients when the primary device was successful at achieving TICI 2b or 3 revacularization was $47 673 for PS (n=53), $46 735 for SRLA (n=20), and $31 716 for ADAPT (n=46) (p=0.007). There was no significant difference in the average total costs between the PS and SRLA groups (p=0.6228). The ADAPT group also had a smaller range in total costs than the PS and SRLA group (figure 1).

{kind=link}
Boxplot depicting total cost for ADAPT, PS and SRLA procedures.
Discussion
This study found that use of the ADAPT technique to revascularize occluded vessels in patients with acute ischemic stroke had a significantly lower cost, faster recanalization time, superior degrees of TICI 2b/3 recanalization with similar clinical outcomes. These findings demonstrate a cost-effective approach to the endovascular management of patients with large vessel occlusions.
The current approach to acute stroke thrombectomy has evolved over the last several years.3 The use of stent retrievers and very navigable large-bore aspiration catheters independently or in combination has resulted in superior angiographic outcomes over prior devices or techniques.4 ,6–8 ,12 ,13 These approaches have similar recananlization rates but often require adjunctive technologies such as a stent retriever to augment aspiration or using aspiration if the stent retriever is not successful. The basis of the ADAPT philosophy—to first use aspiration with a large-bore catheter and then to use a stent retriever or separator if this fails—builds on the concept of starting simple and then adding more complex tools as needed.10
High degrees of TICI 2b/3 recanalization were achieved with all devices and techniques, but were highest with ADAPT (95%). ADAPT had a significantly higher percentage of cases achieving TICI 2b/3 revascularization than PS, but the differences between ADAPT and SRLA or between SRLA and PS were not significant. Significantly more patients achieved TICI 3 outcomes in the ADAPT and SRLA groups. While the angiographic outcomes were significantly better in these groups, the proportion of patients achieving mRS 0–2 in the ADAPT and SRLA groups was also greater, but the difference was not significant.
While improvements in revascularization rates occurred, this was also accompanied with an improvement in the time required to achieve TICI 2b/3 recanalization. No significant difference was seen in the time required for revascularization between ADAPT and SRLA, but both were significantly faster than PS. The difference was probably related to improvements in catheter technology that allow current generation aspiration catheters to navigate easily into the brain blood vessels with minimal discomfort to the patient. The significance of this should not be downplayed, as it has also allowed transition from general anesthesia to conscious sedation for nearly all stroke cases. We previously reported that nearly a quarter of our patients who were intubated had some type of complication in the intensive care unit (ICU) such as extubation failure, pneumonia, or sepsis. When this occurred, the average ICU stay was prolonged from approximately 3 days to almost 11 days and the chance of a good functional outcome decreased from approximately 50% to 20%.14 This is consistent with other published data showing improved clinical outcomes in patients undergoing sedation rather than general anesthesia.15 These data highlight the fact that functional outcomes are probably multifactorial.
Endovascular therapy has recently been shown to be associated with better clinical outcomes and to have a higher cost of recovery than intravenous tissue plasminogen activator in patients with large vessel occlusions.16 However, the endovascular approach to acute stroke is varied, which can significantly influence the cost of the procedure and affect subsequent care. We found that the use of the ADAPT technique significantly lowered our procedure costs, hospitalization costs, and LOS. All of these factors have lowered the overall cost of care for the average stroke patient to $33 610. The reimbursement for diagnosis-related group (DRG) 23–24 for our hospital for 2014 is $38 963.
The ADAPT group had the lowest mean cost of care and the smallest range in costs. The PS group had a significantly wider range in cost, which was more than 1.5 times higher than the range of the ADAPT device group combined. Increased costs associated with the use of a mechanical separator device in the PS group may be attributable to the tendency for such devices to fragment and dislodge the thrombus into downstream vessels requiring further thrombectomy. Such downstream fragmentation increases the need for use of additional smaller catheters to achieve revascularization in the distal vessels, which further increases cost. The large number of cases in this group should increase the accuracy of these data. The SRLA device group had a high mean cost at $54 663.59. The overall cost in this group is probably minimally impacted by the cost of an aspiration catheter in addition to a stent retriever. The cost ranges on these procedures was less than with PS, suggesting a higher primary device success rate and requirement for fewer or cheaper adjunctive devices in the case of failure.
The significantly lower use of general anesthesia in the ADAPT group probably did not affect the procedural cost as an anesthestist was still present and the care-related procedural charges do not differ based on intubation. The lower device costs, decreased LOS, and lower chance of ICU-related complications in this group were probably the primary drivers for lowering the overall cost of the hospitalization. The reduction in LOS between PS and ADAPT was 3.6 days (10.6 vs 7.0), which directly translates into a significant cost reduction. This can be extrapolated further to a potential additional 17.7 patients per year who could be accommodated in a hospital running at capacity. With average DRG reimbursement of $38 963, this potentially amounts to $689 645 in additional revenue per year if beds were backfilled immediately.
Several limitations in both device cost and efficacy exist in this study. This study was not designed to illustrate differences in patient clinical outcomes, only cost differences and differences in the degree of recanalization. All patients who underwent endovascular stroke therapy were considered for this study, regardless of time of symptom onset. Although previously documented, variables for each case such as NIHSS score, mRS, and time from last normal to procedure start were not considered when analyzing the data.9 These daily practice variables and others must be considered when comparing outcomes to select patients reported in stroke trials. Data were missing from several patients, the majority in the PS group, but the large number of cases in this group makes it likely that this did not influence the results. Most devices used in the cases were subject to unit cost inflation from 2009 to 2010 and, as a result and for the purposes of this study, the device cost was standardized using manufacturers’ suggested retail price values from the last year they were used (PS 2012; SRLA 2013; ADAPT 2014). For the purposes of this study, the cost of recombinant tissue plasminogen activator was standardized from 2009 to 2012 at $87 per 2 mg used. Most importantly, the sample sizes of the ADAPT and SRLA groups is relatively small. However, the standardized approach with these techniques and the high success rate with the primary device is not likely to change the overall cost due to low probability of using a different device. Larger ADAPT and SRLA group data would also be more likely to positively affect our clinical and angiographic outcomes, although these values are within those reported in the literature.
In conclusion, for the treatment of patients with acute stroke, the use of the ADAPT technique was the most cost-effective method to achieve very high recanalization rates and low complication rates. The addition of a stent retriever, while improving recanalization, significantly increases costs of care. By contrast, the use of the ADAPT technique achieves a similar rate of recanalization without a similar increase in cost. This suggests that the most cost-effective approach to a large vessel occlusion is direct aspiration with a large-bore catheter (without the separator) first and, if this fails, to proceed with other devices such as a stent retriever.
References
Footnotes
Contributors All authors contributed to writing the article, revising the article and final approval of the article for submission to this journal.
Competing interests AST, AS, RT, and MIC have interests in the following companies in the way of speakers’ bureaus, honoraria, research grants and consultants: Mircovention, Stryker, Penumbra, Siemens, Codman, and Medpace.
Competing interests None.
Ethics approval Ethics approval was received from the Medical University of South Carolina Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.