Article Text

Abstract
Advances in the management and endovascular treatment of intracranial aneurysms are progressing at a tremendous rate. Developments in novel imaging technology may improve diagnosis, risk stratification, treatment planning, intraprocedural assessment, and follow-up evaluation. Evolution of devices, including microwires, microcatheters, balloons, stents, and novel scaffolding devices, has greatly expanded the potential to treat difficult aneurysms. Although developments in technology have greatly improved the efficiency and efficacy of treatment of neurovascular disorders, novel devices do not always improve outcomes and may be associated with unique complications. As such, it is paramount to have an in-depth understanding of new devices and the implications of their introduction into clinical practice. This review provides an update on developments in endovascular treatment of intracranial aneurysms.
- Aneurysm
- Balloon
- Stent
- Coil
- Angiography
Statistics from Altmetric.com
Introduction
Endovascular treatment of intracranial aneurysms has significantly increased, and is the primary treatment modality at many centers. Additionally, advances in the management and endovascular treatment of intracranial aneurysms are progressing at a tremendous rate. This includes imaging technology as well as devices used in treatment. Developments in novel imaging technology may improve patient evaluation and treatment. Evolution of devices may also significantly help improve the efficiency and efficacy of treatment. Although developments in technology have greatly improved, novel devices do not always improve outcomes and may be associated with unique complications. As such, it is important to have an in-depth understanding of new devices and the implications of their introduction into clinical practice. This review provides an update on developments in endovascular treatment of intracranial aneurysms.
Developments in imaging technology
Improvements in imaging technology are greatly expanding our ability to assess and understand the morphology of intracranial aneurysms. Although digital subtraction angiography (DSA) is the gold standard, non-invasive modalities, computer enhanced alterations, and intraprocedural adjuncts can improve evaluation. Future developments in imaging may improve diagnosis, risk stratification, treatment planning, intraprocedural assessment, and follow-up evaluation.
Three-dimensional evaluation
During cerebral angiography, multiple images can be obtained during rotation of a single C arm to create a three-dimensional image. Three-dimensional rotational angiography may decrease fluoroscopy time and contrast load while helping with diagnostic evaluation, treatment planning, and catheter navigation (figure 1A). Three-dimensional imaging can provide detailed assessment of intracranial aneurysm anatomy as well as associated parent vessels and perforator arteries. Studies have found that this may allow detection of small aneurysms which are unable to be visualized in two-dimensional angiography.1 Three-dimensional imaging also allows selection of optimal working projections for aneurysm treatment. After developing a treatment plan, an interactive three-dimensional roadmap can be created that allows three-dimensional imaging to be overlaid on live fluoroscopy in any working projection to guide catheterization through complex vascular anatomy or aneurysms.2

Three-dimensional (3D) reconstruction of a basilar tip aneurysm (A). Flat panel 3D CT angiography following placement of a Surpass flow diverter stent for a giant internal carotid artery aneurysm (B). Intravascular ultrasound demonstrates the navigation of a vessel with a diameter of 4 mm (C). Optical coherence tomography following stent placement demonstrates incomplete apposition of the stent (arrow) to the blood vessel lumen with associated artifact from the stent (broken arrow; D).
Flat panel detection
Flat panel detector angiographic CT imaging can also be carried out during cerebral DSA with a single C arm to create a three-dimensional image within the associated bony anatomy with less beam hardening from coils, stents, or intra-aneurysmal flow diverters (figure 1B).3 ,4 Flat panel detector software can greatly improve visualization of stent position, configuration, and apposition to the parent vessel wall. This provides detailed anatomic data that can help define in-stent stenosis, thrombosis, endoleaks, fractures, incomplete deployment, and twisting.5 ,6 Additionally, flat panel CT can be used to evaluate for intraprocedural complications, such as subarachnoid or intraparenchymal hemorrhage, without the necessity for patient transfer to a CT scanner.7
Four-dimensional assessment
Time resolved three-dimensional phase contrast velocity mapping can be performed with CT or MRI to provide a fourth dimension of volumetric blood flow. Most recently, this has been used during conventional three-dimensional cerebral angiography to generate time resolved sequences with improved spatial and temporal output.8
These three-dimensional reconstructions of cerebral blood flow can provide multidirectional velocity data and assessment of flow patterns, including laminar, helical, or turbulent blood flow within complex vascular lesions.9 Post-processing software allows quantification of pre- and post-procedure blood volume, calculation of three-dimensional pressure differences, and derivation of hemodynamic indices, such as wall shear stress and pulse wave velocity, based on vascular compliance.9 This hemodynamic evaluation may provide improved risk assessment for the likelihood of aneurysm rupture and prediction of periprocedural complications or aneurysm obliteration.
Microangiography fluoroscopy
Continual imaging improvements in DSA allow clearer visualization of vascular anatomy. Specifically, microangiography uses extreme fluoroscopic resolution within a small field to provide exquisite detail. For complex anatomy, this may help define microwire or microcatheter position. Additionally, this may be particularly beneficial during the treatment of very small or large, partially thrombosed aneurysms in defining areas of incomplete coiling or residual aneurysm filling.10
Intravascular ultrasound
Intraprocedural cerebral angiography is greatly limited in its evaluation of the wall thickness of cerebral blood vessel walls. Unlike MRI, CT, and DSA, ultrasound provides a limited three-dimensional assessment of vessel wall layers (figure 1C). In the example of a dissection, visualization is achieved by determining the alterations in contour and caliber of the intima and identifying potential contrast extravasation/stasis within the vessel wall.11 Intravascular ultrasound has seen little use in cerebrovascular pathology, but development of smaller delivery catheters may allow expansion of its use into the intracranial realm. This technique has the benefit of being able to provide a real time evaluation of both intravascular and vascular wall pathology, and it has been used extensively in coronary angiography in the delineation of a wide range of pathology, including plaque, thrombus, and dissections.11 ,12 Additionally, large trials have demonstrated that intravascular ultrasound may improve stent placement, apposition, and overall technical outcomes.13 In cerebral pathology, ultrasound may help further define intraluminal and extraluminal aneurysm morphology not fully defined by angiography.14
Optical coherence tomography
Intravascular ultrasound is limited by artifact and overall tissue penetration. Optical coherence tomography (OCT) is an optical signal acquisition and processing method that can capture microscopic resolution of tissue from a light source mounted within a microcatheter. Similar to confocal microscopy, an optical based technique, OCT penetrates more deeply into surrounding tissue. Unlike confocal microscopy, OCT can provide imaging at a microscopic, but not subcellular, resolution. Frequency domain OCT provides advantages in signal to noise ratio, thereby permitting faster signal acquisition. This can allow real time imaging of a 5 cm length of blood vessel segment while the light source and camera move within a stationary rapid exchange 0.014 inch microcatheter positioned over a microwire. This generates a cross sectional and longitudinal image that can be re-created into a three-dimensional image or video. Microscopic imaging allows visualization of vessel wall components, including the intima, media, and adventitia, and can clearly identify small perforating arteries.11 ,15 ,16 This has been adapted in the coronary vasculature to improve visualization of vessel pathology and can be used to differentiate among fibrous, calcified, and lipid plaques, and between acute, red colored clot, and chronic white colored thrombus or emboli.11 ,15 ,16
Intraprocedurally, this imaging can be rapidly acquired following stent deployment to obtain additional microscopic evaluation of stent struts, apposition to the parent vessel, endoleaks, patency of perforating arteries, in-stent stenosis or thrombosis, and tissue prolapse through the stent.11 ,15 ,16 On follow-up angiography, OCT may demonstrate neointimal growth, restenosis, and stent fracture, foreshortening, or prolapse (figure 1D).11 ,15 ,16 Since this modality relies on a light source, there is no additional radiation. Therefore, OCT may be a safer modality than both DSA and flat panel technology for imaging of stents and coils after deployment.
Developments in aneurysm treatment technology
Detachable coils
For endovascular treatment of intracranial aneurysms, there is a wide selection of detachable coils. Recent advances with softer coils have expanded the endovascular repertoire. Prior trials comparing surgical and endovascular treatment of aneurysms did not include aneurysms of very small size,17 in part due to the potentially increased risk of intraoperative rupture with endovascular therapy for small aneurysms (<3 mm).18 With the advent of smaller (1 mm in diameter) and softer coils, it is now possible to treat these small aneurysms. A study comparing microsurgical to endovascular treatment of small aneurysms demonstrated higher complication rates with microsurgical clipping and higher retreatment rates with endovascular therapy, but similar overall functional outcomes between modalities.19 Further prospective studies are indicated; the Effectiveness and Safety of Small Aneurysm Coiling Trial (NANO trial) aims to prospectively assess the long term outcomes of small aneurysms treated with microcoils.
For larger aneurysms, coils with an increased secondary diameter are now available that may decrease the number of coils necessary to achieve an adequate packing density. The P400 coils (Penumbra Inc, Alameda, California, USA) have increased their primary shape diameter to 0.0020 inches while utilizing a smaller nitinol coil for support. Preliminary results from a small single center experience demonstrated acceptable results20 but we await the final outcomes of the Aneurysm Coiling Efficiency Study of the Penumbra Coil 400 System (ACE trial). A number of coils have also recently been developed to achieve greater packing density with fewer coils by increasing the outer diameter of the primary coil from 0.010 to 0.014 inches while allowing selection from coils of varying stiffness.
A number of bioactive coils have been developed. These coils have a coating that is meant to expand after contact with blood. These novel coils have the potential to increase packing density and decrease retreatment rates. Despite these theoretical advantages, multiple randomized clinical trials, including the recently released long term results of the Matrix and Platinum Science (MAPS) trial did not shown the superiority of bioactive coils over bare platinum coils.21–23
Liquid embolics
Unlike coils, liquid embolization may allow for complete occlusion of the aneurysm as a liquid agent may be better able to assume the conformation of the aneurysm. The most widely tested agent is an ethylene vinyl alcohol copolymer, Onyx HD500 (ev3 Inc, Irvine, California, USA). Liquid embolics are typically delivered through a microcatheter jailed within the aneurysm by a balloon. Although this has only been reported in the treatment of arteriovenuous malformations, newer dual chamber balloons may allow simultaneous flow cessation and Onyx delivery.24 Despite these potential advantages, liquid embolic agents have been associated with high complication rates, and parent vessel stenosis and occlusion at follow-up.25–27 As such, liquid embolic agents are often reserved for retreatment of complex aneurysms not amenable to alternative treatment strategies.27
Developments in stent technology
The area of greatest advancement over the past several years has been in the field of primary and adjunct endoluminal devices for the treatment of complex aneurysms. This includes the use of stents for coiling assistance, intra- and extra-aneurysmal flow diversion technology, and aneurysmal neck reconstruction and coil support devices. While offering additional treatment options, these devices are not without a number of unique risks. The use of an endoluminal device often necessitates that the patient be placed on dual antiplatelet therapy, which can predispose the patient to gastrointestinal bleeding, bruising, or bleeding, and exacerbation of intraoperative complications.
As delivery catheters must be navigated distal to the aneurysm neck prior to device deployment, there is the potential for distal vessel injury in addition to local parent vessel or aneurysm perforation.28 This may also increase the risk of thromboembolic events. In ruptured aneurysms, the use of dual antiplatelet therapy may be associated with an increased incidence of complications, especially in post-subarachnoid hemorrhage patients who require permanent CSF diversion.29 In the long term, the endoluminal devices may be associated with in-stent stenosis, thrombosis, and thromboembolic complications.28
Low surface area coverage stents
Currently, there are two stents approved by the Food and Drug Administration (FDA) through a humanitarian device exemption for the treatment of intracranial aneurysms which provide approximately 5% parent vessel coverage. The partially open cell (hybrid architecture) Neuroform stent (Stryker Neurovascular, Fremont, California, USA) (see online supplementary figure IA) and closed cell Enterprise stent (Cordis Corporation, Miami Lakes, Florida USA) (see online supplementary figure IB) are both self-expanding stents produced from thin film nitinol hypotubes. Stent assisted coiling has been associated with relatively higher rates of aneurysm obliteration and lower rates of aneurysm recurrence compared with coil embolization alone, but the associated incidence of complications may be increased.30–32 Although there have been no prospective randomized studies to compare the Enterprise and Neuroform stents, a number of studies have compared institutional outcomes. Two earlier studies found greater difficulties with the delivery of the Neuroform stent,33 ,34 two studies found greater aneurysm recanalization rates with the Neuroform stent,33 ,35 and one study found increased complications associated with the Enterprise stent.33 Disparities in outcomes between stent technologies may be partly attributable to older designs.33 ,34 Next generation Neuroform stents have greatly improved the delivery mechanism. The next generation of Enterprise stents, which are not currently available in the USA, have an improved platform that will likely improve stent apposition to the parent vessel around tight bends and improve angiographic visualization (see online supplementary figure IC).
The Liberty stent (Penumbra) is a self-expanding stent currently under review in an ongoing clinical trial.36 Compared with the Enterprise (0.042 mm) and Neuroform (0.066 mm) stents, the Liberty stent is produced from an ultrathin 0.005 mm nitinol hypotube that may improve delivery, decrease thromboembolic complications, and decrease the incidence of associated vessel injury and perforation.37 ,38
Although originally designed for use in stent assisted coiling of cerebral aneurysms, the Solitaire stent (Covidian, Mansfield, Massachusetts, USA) has predominantly been used in mechanical thrombectomy for the treatment of acute ischemic stroke. This stent may also be detached, and recently more centers in Europe have been using it in stent assisted coiling of aneurysms.39 As the Solitaire may be retrieved and has limited metal coverage, this stent may be associated with fewer thromboembolic complications which make it a potentially more attractive alternative in the treatment of ruptured wide necked aneurysms.40 ,41 Further studies are necessary to determine the benefits and optimal indications for low coverage nitinol stents.
Intermediate coverage stents
Woven or braided stents are cut from nitinol fiber with an approximate diameter of 0.05 mm to create an intermediate degree of parent vessel coverage (∼15%) which is greater than conventional nitinol hypotube stents (∼5–10%) but less than flow diverting stents (∼30%). Stents with greater parent vessel coverage have the potential advantage of increased parent vessel support and protection, but this may be offset by greater difficulties accessing the aneurysm through the tines of the stent or removing jailed microcatheters, poorer trackability, and a greater risk of thromboembolic complications. Currently, there are no FDA approved woven or braided stents, but three stents are currently in use in other countries and the subject of current clinical trials. The closed cell Leo stent used in Europe (Balt Extrusion, Montmorency, France) has a number of advantages over the Neuroform and Enterprise stents, including radiopaque markers which increase visibility, and the ability to be retrieved after 90% unsheathing. In seven retrospective series of 9–28 patients, the Leo stent resulted in complete aneurysm occlusion in 65% of patients, complications in 8.9%, and recurrence in 7.7%.42–48 Further assessment with long term follow-up is indicated.
The newest woven or braided stent is the low profile visualized intraluminal support (LVIS; MicroVention, Tustin, California, USA) device, which is currently only available in the USA as part of a clinical trial (figure 2A). Similar to the Leo stent, it is cut from nitinol wire (0.056 mm), has improved radiopaque markers compared with the Enterprise and Neuroform stents, and is retrievable after up to 80% deployment.49 A smaller version (LVIS Jr) is available which can be placed through a microcatheter with an inner diameter of 0.0165 inches (figure 2B). This may facilitate stenting of aneurysms with smaller parent vessel diameters or creation of Y configuration stent constructs with easier navigation through the tines of a larger stent. Preliminary in vivo and clinical outcomes with the LVIS stents are encouraging, but current clinical trials have not yet been completed.49 ,50
The low profile visualized intraluminal support (LVIS) stent (A). Middle cerebral aneurysm status after placement of the LVIS Jr (B, C). Final treatment image status after stent assisted coiling of the middle cerebral artery aneurysm with the LVIS Jr (D).
Flow diverting stents
Observation of the altered flow dynamics in an aneurysm after stenting prompted the development of specialized devices that could be used for endoluminal reconstruction of the artery and flow diversion away from the aneurysm. These devices, which provide higher coverage of the parent vessel (30–50%) than conventional intracranial stents, can decrease blood flow into the aneurysm, resulting in stasis of the intrasaccular blood products and eventual aneurysmal thrombosis.51 This may also lead to potential aneurysm regression, thereby reducing aneurysm related mass effect. Flow diverters theoretically provide an alternative therapy for wide necked, giant, or fusiform aneurysms that are associated with significant morbidity and mortality following treatment with either microsurgical or traditional endovascular treatments.52 Studies have also found these devices to be an acceptable alternative therapy for small aneurysms,53 blister aneurysms,54 and pseudoaneurysms55 that may be difficult to treat with conventional endovascular approaches. A drawback of flow diverters is delayed obliteration, which is particularly risky with these fragile aneurysms which may be associated with high re-rupture rates.
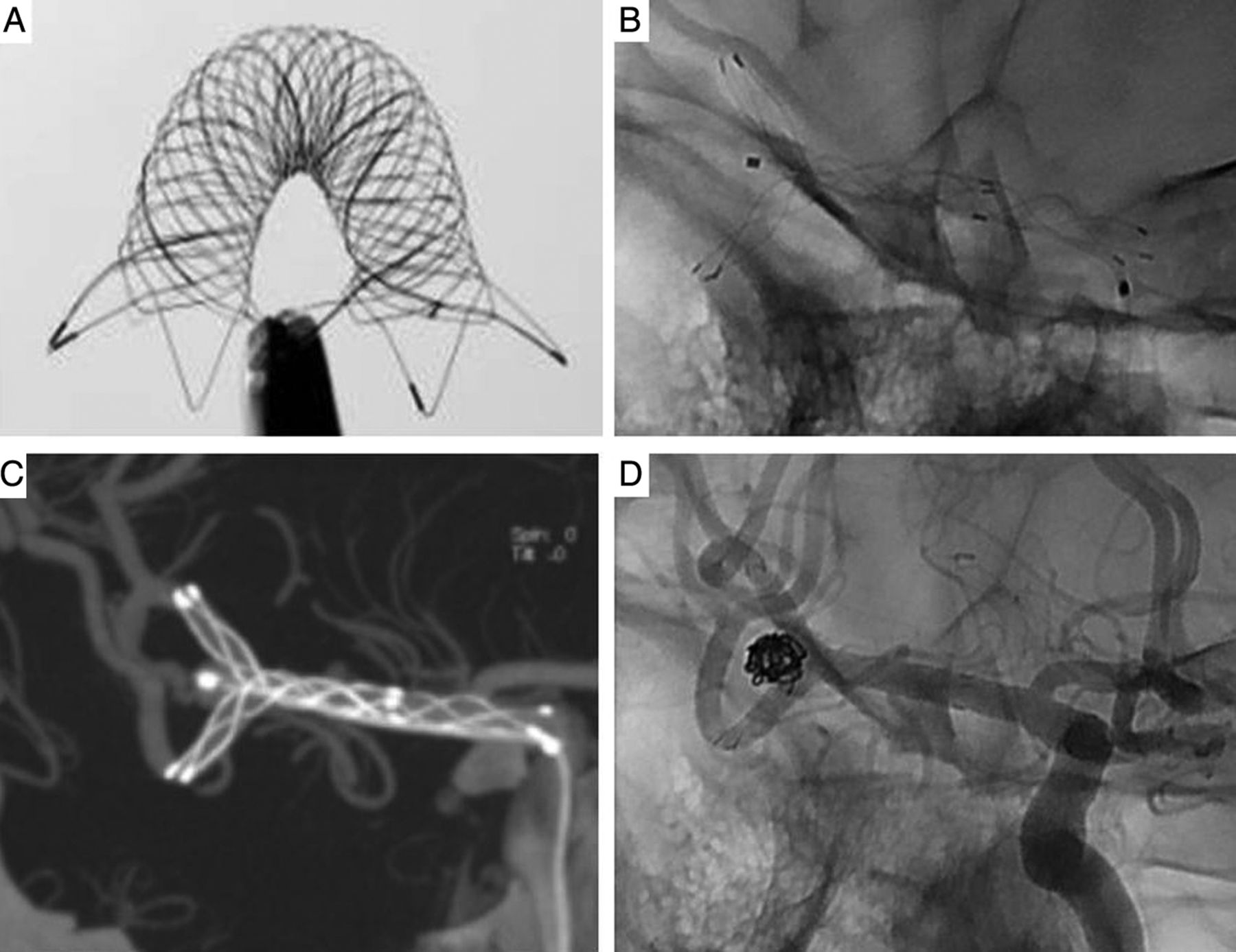
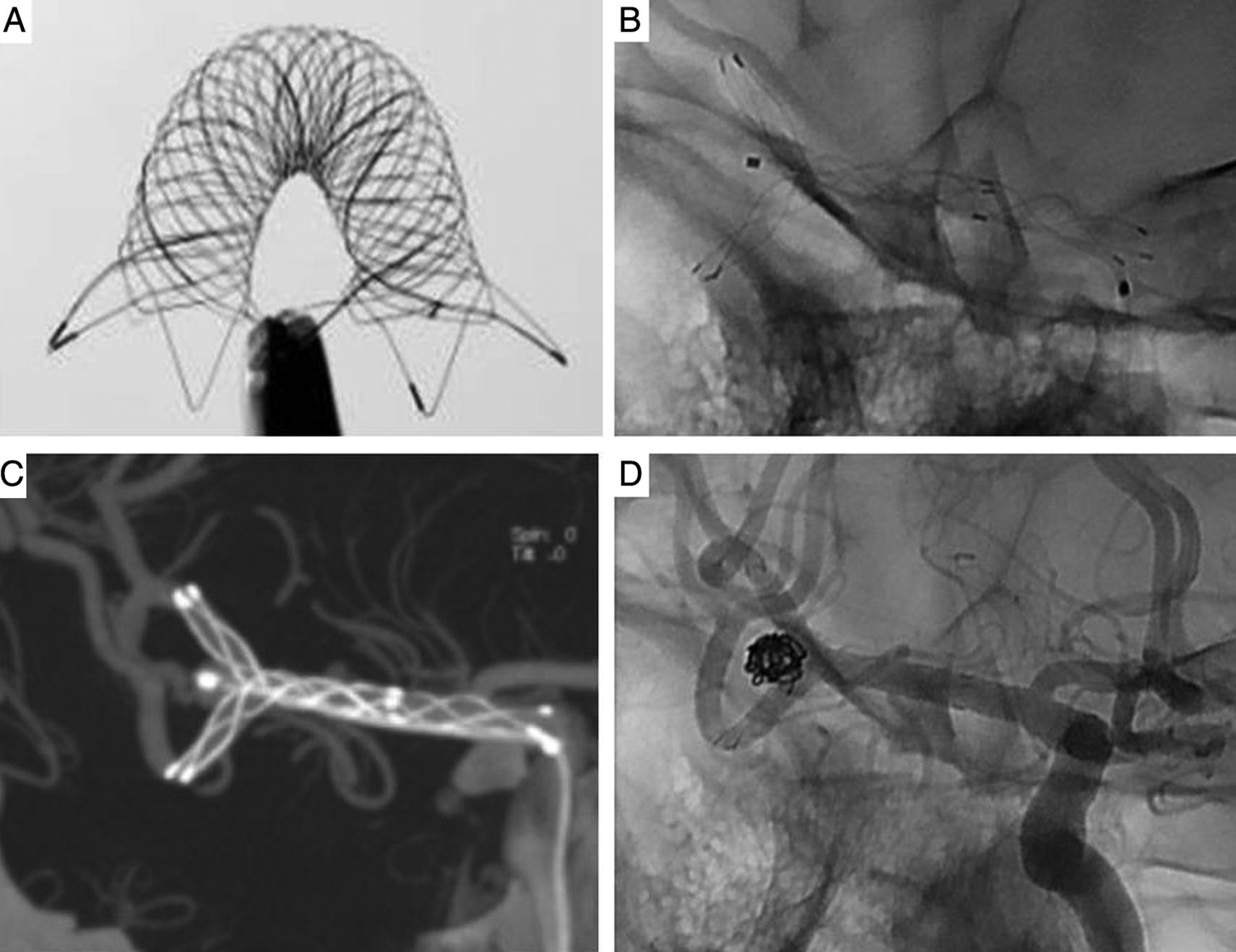
Currently, there are four flow diverters available for the treatment of cerebral aneurysms but only two are available outside of research studies: the pipeline embolization device (PED; ev3) (figure 3) and the silk flow diverter (SFD; Balt Extrusion), which is only available outside of the USA. The PED is manufactured from 48 microfilaments with a consistency of 25% platinum–tungsten and 75% cobalt–chromium–nickel, providing 30–35% parent vessel metal coverage.51 Since the original prospective studies of PED treatment for large (>10 mm) anterior circulation aneurysms, there have been numerous additional reports in a wide variety of aneurysms. A recent meta-analysis of 29 studies of 1451 patients with 1654 aneurysms treated with the PED found an occlusion rate of 76% at 6 months (95% CI 70% to 81%) and an associated morbidity and mortality of 5% (95% CI 4% to 7%) and 4% (95% CI 3% to 6%), respectively.51

Pipeline embolization flow diverting stent (A). Intraoperative removal of the pipeline embolization device during microsurgical clipping of a giant expanding aneurysm despite flow diversion (B). The Surpass flow diverter stent (C). Stagnation of contrast within a giant internal carotid artery aneurysm following placement of the Surpass (D).
As with many procedures, increasing experience leads to decreased complications,56 but novel devices may be associated with previously unseen complications or a higher frequency of commonly observed complications. With the PED, there is particular concern regarding the risk of perforator artery infarction, which was noted to occur in 3% of cases (95% CI 1% to 5%), with a significantly lower rate of perforator infarction in patients with anterior circulation aneurysms compared with those with posterior circulation aneurysms (OR 0.01; 95% CI 0.00 to 0.08; p<0.0001).51 Additionally, ischemic strokes occurred in 6% of patients (95% CI 4% to 9%), also at a significantly lower rate in patients with anterior circulation aneurysms (OR 0.15; 95% CI 0.08 to 0.27; p<0.0001). In particular instances, perforators may remain open following PED treatment, which may represent a significant demand phenomena that continues to pull blood through the perforator artery.54
The rates of postoperative subarachnoid and intraparenchymal hemorrhage after flow diverter treatment are each 3% (95% CI 2% to 4%).51 Most alarming are distal intraparenchymal hemorrhages that have been reported weeks to months after flow diversion. One recent histopathological review of three cases of delayed fatal ipsilateral intraparenchymal hemorrhage following PED treatment demonstrated the presence of foreign material occluding small distal vessels within the hemorrhagic area in all patients.57 Fourier transform infrared spectroscopy demonstrated the presence of polyvinylpyrrolidone in the specimens, a substance that is commonly used for the coating of interventional devices.
Finally, complications have occurred due to the inability to appropriately deploy PEDs, direct parent vessel occlusion, and persistently enlarging giant thrombotic aneurysms despite parent vessel reconstruction.58 ,59 For these instances and other failed treatments with flow diverters, alternative endovascular or microsurgical treatments may be particularly difficult.58 ,59 The next generation pipeline flex embolization device, which is still under FDA review, includes improvements in delivery and potential for post-deployment resheathing.
The SFD was approved for use in Europe in 2008 and is composed of four platinum and 48 nitinol microfilaments.60 Adjunctive intrasaccular coiling is recommended with the SFD, and the device is resheathable up to 90% deployment. Thus far 285 patients with 317 aneurysms treated with the SFD have been reported in the literature, with an associated delayed occlusion rate of 82% at 12 months and morbidity, mortality, and intracerebral hemorrhage (ICH) rates of 12.5% 4.9%, and 1.4%, respectively.61
Two other flow diverting stents, the Surpass flow diverter (Stryker Neurovascular) (figure 3) and the flow redirection endoluminal device (FRED; MicroVention) (see online supplementary figure II), are currently only available as part of clinical trials in the USA. The Surpass provides surface coverage of approximately 30% but with a consistent porosity of approximately 70% across all sizes that may reduce the usage of multiple overlapping stents.61 The only published Surpass series, comprising 37 patients with 49 aneurysms, reported an obliteration rate of 83% at 6 months, with mortality, morbidity, and ICH rates of 0%, 14.3%, and 2.0%, respectively.62 The FRED has a unique overlapping stent design with a high porosity outer stent and a low porosity inner stent comprised of 48 nitinol strands. There have been three reported series with the FRED, including treatment of 51 patients with 59 aneurysms, with 100% occlusion rates in those with more than 6 months of follow-up, and morbidity and mortality rates of 3.8% and 0%, respectively, without any cases of delayed ICH.63–65 Further studies are necessary to better define the optimal aneurysms for specific flow diverting devices, long term obliteration rates, associated complications, and alternative therapies for aneurysms that have failed flow diversion.
Intra-aneurysmal flow diversion
Intra-aneurysmal flow diverting three-dimensional constructs have been developed that are composed of braided nitinol wire that are deployed within the aneurysm sac to disrupt blood flow into the aneurysm and promote thrombosis.66 ,67 These devices are optimal for bifurcation aneurysms that are not easily treated with current flow diverting stents or conventional coil embolization. As these devices are intra-aneurysmal, they may not require dual antiplatelet therapy and are not associated with parent vessel stenosis, as can be found with stents. Both the Luna (Covidien Vascular Therapies, Irvine, California, USA) (figure 4A) and the Woven Endo-Bridge (SequentMedical, Aliso Viejo, California, USA) (figure 4B) have demonstrated promising early clinical results.66 ,67

The Luna (A) and placement within an aneurysm in vitro (B). Woven Endo-Bridge (WEB) (C) and cerebral angiography before and after treatment of a middle cerebral artery aneurysm with the WEB, demonstrating aneurysm obliteration. Arrow demonstrates right middle cerebral artery aneurysm prior to treatment.
Aneurysmal neck reconstruction and coil support devices
Wide necked cerebral aneurysms that are located at bifurcations are particularly challenging for endovascular treatment. Endovascular approaches for wide necked bifurcation aneurysms may require Y configuration stenting which involves placement of a secondary stent within a primary stent,68 a ‘double-barrel’ construct of two side by side stents,69 or intrasaccular placement of one end of a stent to create a ‘waffle cone’ appearance.70 Several case series have reported these techniques, but endovascular treatment of wide necked aneurysms is nonetheless associated with relatively higher rates of periprocedural morbidity and mortality.28 ,68
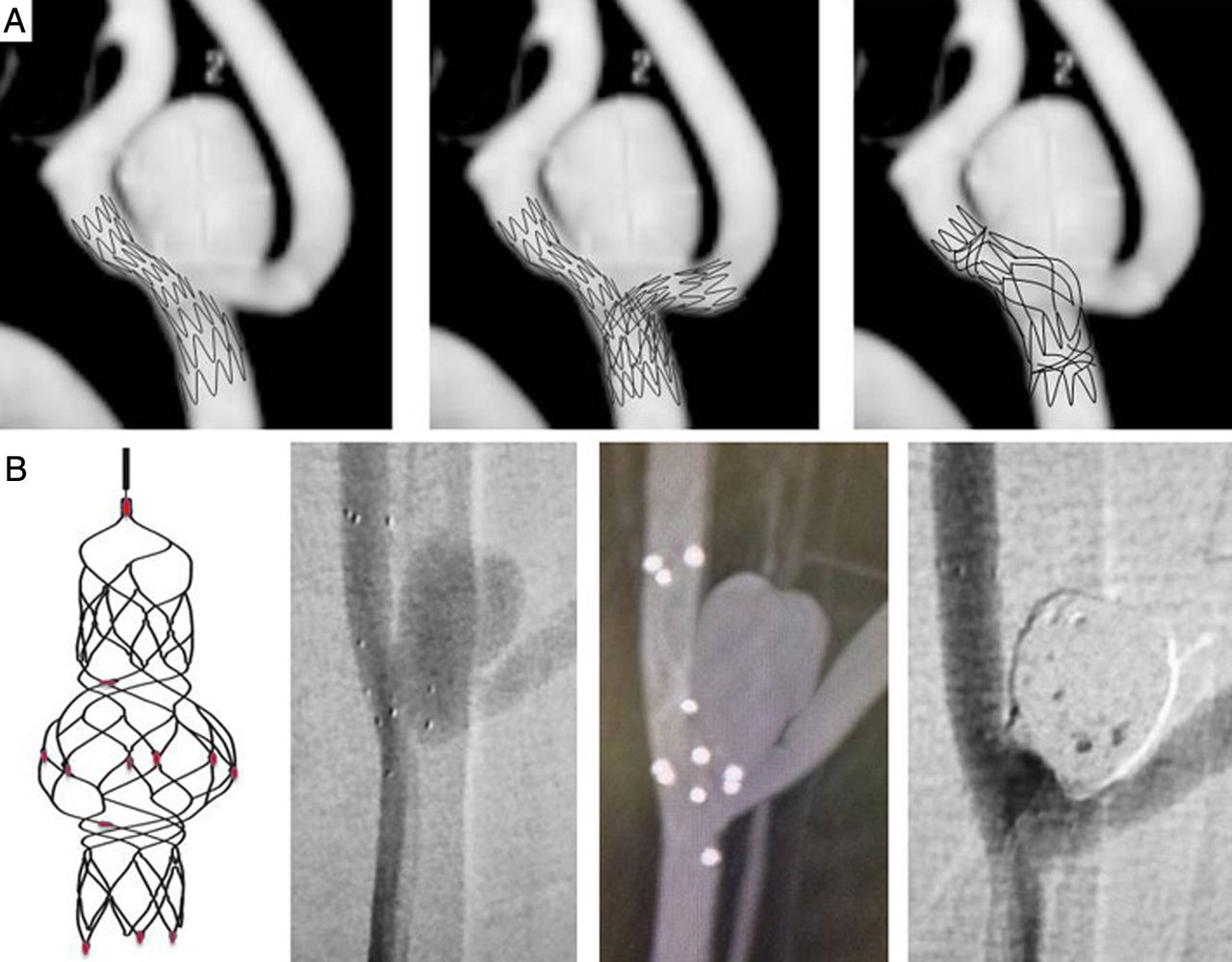
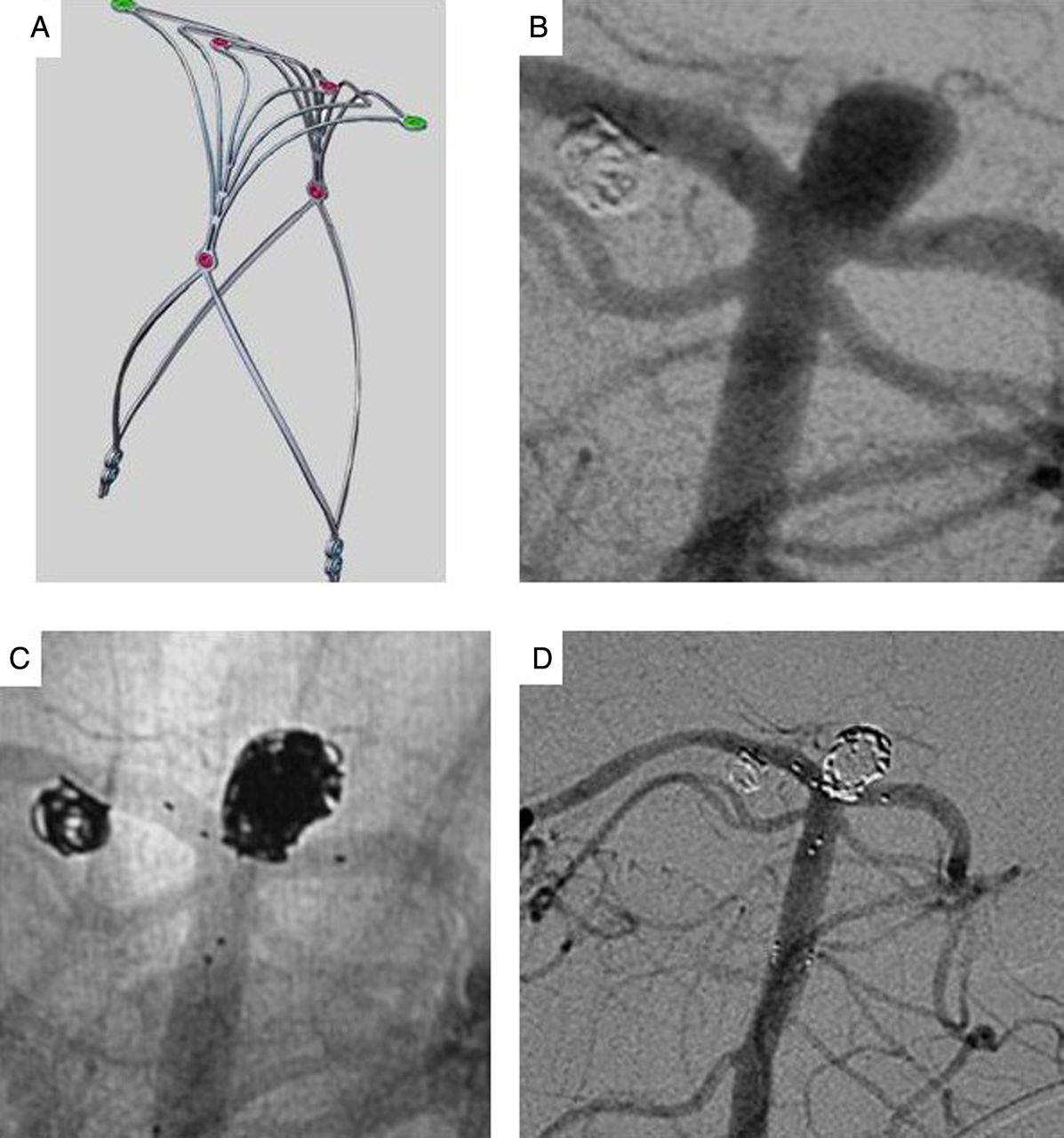
A number of new devices have been created to alleviate the difficulties associated with the treatment of wide necked bifurcation aneurysms. The Barrel stent (Reverse Medical, Irvine, California, USA) (figure 5) is a self-expanding stent that can undergo significant expansion in the central portion of the stent to increase aneurysmal neck coverage and provide a stronger scaffold for stent assisted coiling. The Pulsar vascular aneurysm neck reconstruction device (ANRD; Pulsar Vascular, San Jose, California, USA) and Pulse Rider (Pulsar Vascular) are novel scaffolding devices for the treatment of wide necked bifurcation aneurysms (figure 6).71 The ANRD is a T shaped implant composed of 0.002 inch nitinol, is deployed through a microcatheter, and can support coils placed within the aneurysm. Compared with stents, there is significantly decreased metal surface area. The eClips device (Evasc Medical Systems, Vancouver, British Columbia, Canada) is similar to the ANRD and Pulse Rider in that it is anchored across a wide necked bifurcation aneurysm and, when deployed, creates a high density ‘leaf-like’ structure that can support intrasaccular coils without affecting branch artery patency (see online supplementary figure III). Initial in vivo and human studies are promising but limited. Similarly, the PpCONus (Phenox, Bochum, Germany) is a stent-like structure that was recently approved for the treatment of wide necked aneurysms in Europe. It is deployed with the tip within the aneurysm and may allow for an easier waffle cone stent assisted coiling technique.30 Nevertheless, these novel neck reconstruction devices may improve our ability to treat morphologically complex aneurysms.

Incomplete stent coverage across the neck of a basilar artery aneurysm, ‘Y’ stenting of a basilar artery aneurysm with two stents, and treatment of a basilar artery aneurysm with the Barrel stent (A). The Barrel stent after stent placement for a basilar tip aneurysm, and angiography after Barrel stent assisted coiling (B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The Pulse Rider (A). A basilar artery aneurysm before treatment (B) and after stent assisted coiling with the Pulse Rider (C, D).
Future advances and outcomes
Developments in the management of intracranial aneurysms and in neuroendovascular technology are progressing rapidly. Although advances in interventional therapies have increased the complexity of aneurysms amenable to endovascular treatment, the overall rates of aneurysmal obliteration have been increasing, and rates of recurrence and retreatment have been decreasing over time.21–23 ,72 ,73 Similarly, there have been improvements in overall patient functional outcome over time. In a systematic review of 97 studies of 7172 patients with cerebral aneurysms treated with endovascular therapies, patients treated after 2004 had better functional outcomes (unfavorable outcome 3.1%) than patients treated during 2001–2003 (unfavorable outcome 4.7%) or in 2000 and before (unfavorable outcome 5.6%).32 A review of 60 studies of 9845 patients with 10 845 aneurysms treated with endovascular therapies from 1990 to 2011 also demonstrated a significant decrease in morbidity over time.73 Better outcomes may be attributable to a wide variety of reasons, including improved imaging, endovascular and surgical treatment, and neurocritical care. Further matched and randomized clinical studies are required to determine the overall benefits and changes over time as overall assessment may be limited by overall quality, heterogeneous patient populations, and publication bias.
Despite these advances, increased morbidity has been associated with novel developments, including the use of liquid embolic agents in the endovascular treatment of aneurysms.25–27 ,32 Additionally, complication rates and unfavorable outcomes are increased following treatment of aneurysms with balloon remodeling, stent assistance, and flow diverting devices.32 This may be partially explained by the increased morbidity and mortality associated with the treatment of giant and complex aneurysms. Future studies, including the LARGE randomized clinical trial, which will compare endovascular coiling, stent assisted coiling, and flow diversion for large and giant aneurysms,74 are necessary and may help define the optimal treatment strategies for these patients.
Conclusion
Improvements in cerebrovascular imaging may lead to refined patient evaluation before, during, and after endovascular intervention. Evolution of endovascular devices has greatly increased the potential to treat difficult aneurysms but can also be associated with unique complications. It is imperative to have a comprehensive understanding of these novel devices and to follow preliminary treatment reports in order to assess the long term outcomes and complications. Further studies are necessary to identify the optimal devices for endovascular treatment of intracranial aneurysms.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figures
Footnotes
Contributors All authors: substantial contributions to the conception and design of the work; interpretation of the data for the work; drafting the work and revising it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests AT: consultant for Covidien, MicroVention, Penumbra, Stryker, Siemens, and Codman. ASD: consultant for ev3 and Stryker. PJ: consultant for ev3, Codman, and Mizuho. RDT: consultant for Covidien, Microvention, Codman Neurovascular, Stryker, Penumbra, and Blockade Medical.
Provenance and peer review Not commissioned; externally peer reviewed.